Trends and Issues in Nursing Practice Brenda Mc

Trends and Issues in Nursing Practice Brenda Mc. Millan RN, MS Hinds Community College Associate Degree Nursing Program *

The minimal educational qualification/preparation necessary for a nurse to enter into the profession of nursing. *

* Over the last 100 years the environment in which healthcare is practiced has changed considerably, as has the need for strengthening nursing education. Several factors, such as an aging population, an increasing awareness of economics, and more complex technologies, have contributed to these changes. In this rapidly changing environment technological competence alone is no longer adequate; rather a broader knowledge base is required (American Association of Colleges of Nursing, 2005; Association of California Nurse Leaders, 2000). * http: //nursing. connectwithmhs. org/wp-content/uploads/2013/04/CC 041213 -BSN_Legislating-entry-into-practice_Tina-Barnes 3. pdf

*This broader knowledge base includes the creative decision-making, critical-thinking, and managerial skills needed for dealing with a diverse and multicultural workforce and patient population. Additionally, today’s nurses should also be familiar with such broad ranging topics as cost-benefit analysis and ethical decision making. *

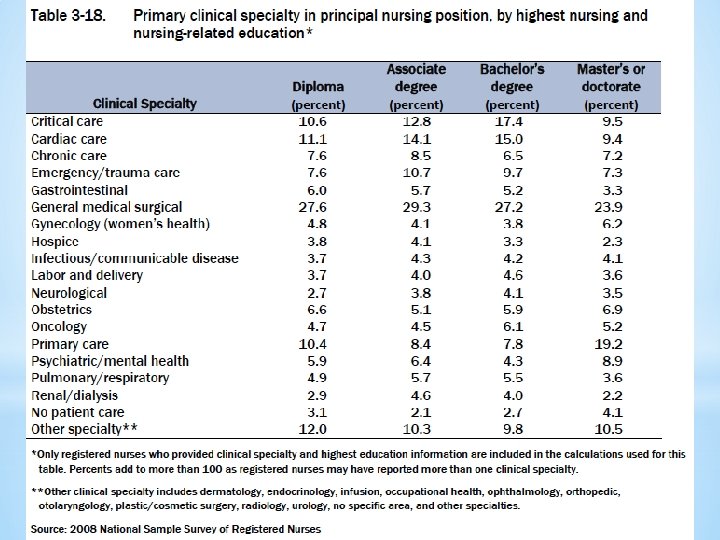
* In most states, basic nursing education is provided at the following levels: * Licensed Practical Nurse (LPN) Diploma Program: A technical/vocational * * * nurse training program administered at the Junior College or vocational school level that ranges, by state, from 9 to 18 month Registered Nurse (RN) Diploma Program: These programs are typically a 23 year experience leading to professional entry into nursing practice. Before the 1970 s there were more than 800 diploma schools in existence; today there are less than 100 Associate Degree Nurse (ADN) Program: A two-year educational program administered at the Junior College level leading to professional entry into nursing practice Baccalaureate Degree Program, generally a Bachelor of Science in Nursing (BSN) Program: A four year nurse education program administered at the upper college level leading to professional entry into nursing practice *

* Currently all state boards of nursing require each nursing graduate to pass the National Council Licensure Examination (NCLEX), developed by the National Council of State Boards of Nursing (NCSBN). The NCLEX is a standardized exam that determines whether or not a candidate is prepared for entry-level nursing practice (NCLEX, 2008). The NCSBN has developed two licensure examinations to test the entry-level nursing competence of candidates for licensure, namely the NCLEX-RN for registered nurses and the NCLEX-PN for licensed practical/vocational nurses. In addition, credentialing programs are offered by the American Nurses Association and a number of specialty organizations. *

* Nursing theory is the body of knowledge that explains the profession of nursing. * Nursing theory is an organized and systematic articulation of a set of statements related to questions in the discipline of nursing. * "A nursing theory is a set of concepts, definitions, relationships, and assumptions or propositions derived from nursing models or from other disciplines and project a purposive, systematic view of phenomena by designing specific interrelationships among concepts for the purposes of describing, explaining, predicting, and /or prescribing. " *

Nursing theory aims to describe, predict and explain the phenomenon of nursing. It should provide the foundations of nursing practice, help to generate further knowledge and indicate in which direction nursing should develop in the future. Theory is important because it helps us to decide what we know and what we need to know It helps to distinguish what should form the basis of practice by explicitly describing nursing. The benefits of having a defined body of theory in nursing include better patient care, enhanced professional status for nurses, improved communication between nurses, and guidance for research and education *

* Assist nurses to describe, explain, and predict everyday experiences. * Serve to guide assessment, interventions, and evaluation of nursing * * * care. Provide a rationale for collecting reliable and valid data about the health status of clients, which are essential for effective decision making and implementation. Help to describe criteria to measure the quality of nursing care. Help build a common nursing terminology to use in communicating with other health professionals. Ideas are developed and words are defined. Enhance autonomy (independence and self-governance) of nursing through defining its own independent functions. *

* Anne Casey - Casey's model of nursing * Betty Neuman - Neuman systems model * Boykin & Schoenhofer * Callista Roy - Adaptation model of nursing * Carl O. Helvie - Helvie Energy Theory * Dorothea Orem - Self-care deficit nursing theory * Helen Erickson * Hildegard Peplau - Theory of interpersonal relations * Ida Jean Orlando (Pelletier) * Imogene King * Isabel Hampton Robb * Katharine Kolcaba *

* Katie Eriksson * Madeleine Leininger * Margaret A. Newman - Health as expanding consciousness theory * Martha E. Rogers - Science of unitary human beings * Paterson & Zderad * Ramona T Mercer - Maternal role attainment theory * Rosemarie Rizzo-Parse - Human becoming theory * Virginia Henderson - Henderson's need theory * Dr. Jean Watson * Erickson, Tomlin & Swain - Modeling and Role-Modeling * Moyra Allen - Mc. Gill model of nursing * Nancy Roper, Winifred W. Logan, and Alison J. Tierney - Roper-Logan* Tierney model of nursing Phil Barker - Tidal Model *

*Purposely omitted from this list is that most famous of all nurses, Florence Nightingale never actually formulated a theory of nursing science but was posthumously accredited with same by others who categorized her personal journaling and communications into a theoretical framework. *Also not included are the many nurses who improved on these theorists' ideas without developing their own theoretical vision. *

Nursing research is research that provides evidence used to support nursing practices. Nursing, as an evidence-based area of practice, has been developing since the time of Florence Nightingale to the present day, where many nurses now work as researchers based in universities as well as in the health care setting. *

*Nurses use research to provide evidence-based care that promotes quality health outcomes for individuals, families, communities and health care systems. Nurses also use research to shape health policy in direct care, within an organization, and at the local, state and federal levels. Nurses conduct research, use research in practice, and teach about research. *

* * Evidence-based practice begins with questions that arise in practice settings. * Nurses must be empowered to ask critical questions in the spirit of looking for opportunities to improve nursing practice and patient outcomes. * In any specialty or role, nurses can regard their work as a continuous series of questions and decisions. * In a given day, a staff nurse may be called to ask and answer questions, such as “Should I give the analgesic only when the patient requests it, or should I encourage him to take it every 4 hours? * Will aggressive ambulation expedite this patient’s recovery, or will it consume too much energy? * Will open family visitation help the patient feel supported, or will it interrupt her rest? ” * A nurse manager or administrator might ask, “Who is the most qualified care provider for our sickest patient today? What is the optimal nurse-to-patient ratio for a specific unit?

* Do complication rates and sentinel events increase with less-educated staff? * Do longer shifts result in greater staff fatigue and medication errors? * Will higher quality and more expensive mattresses decrease the incidence of pressure ulcers? * What benefits promote nurse retention? How does the use of supplemental (or agency) staffing affect the morale of existing staff? * Can this population be treated on an outpatient, rather than an inpatient, basis? * What is the optimal length of time for a comprehensive home care assessment? * How many patients can a nurse practitioner see in 8 hours? ” Likewise, a nurse educator may ask, “Is it more effective to teach a procedure in the laboratory or on an actual patient? * What are the most efficient methods of documenting continued competency? * * Do web-based students perform as well on standardized tests as students in traditional classrooms? ”

*Each type of question can lead to important decisions that affect outcomes, such as patient recovery, organizational effectiveness, and nursing competency. *The best answers and consequently the best decisions come from informed, evidence-based analysis of each situation. *

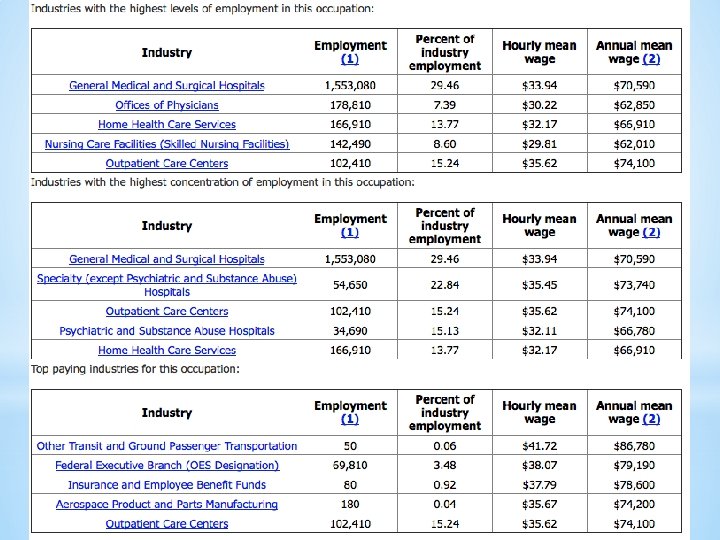
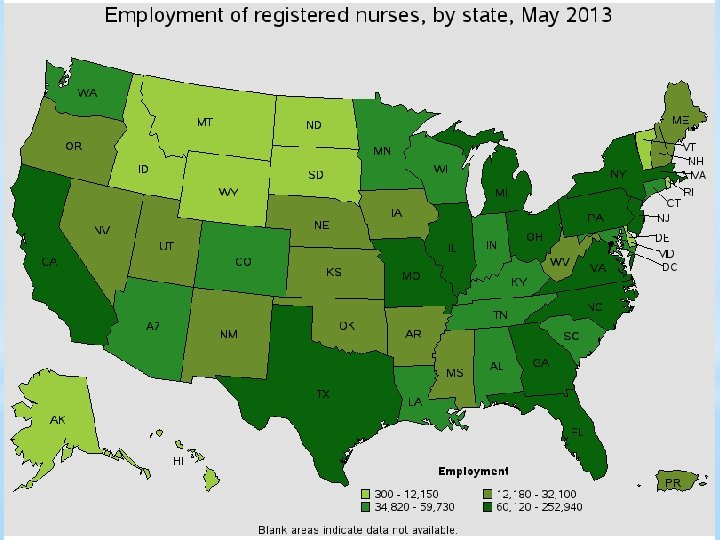
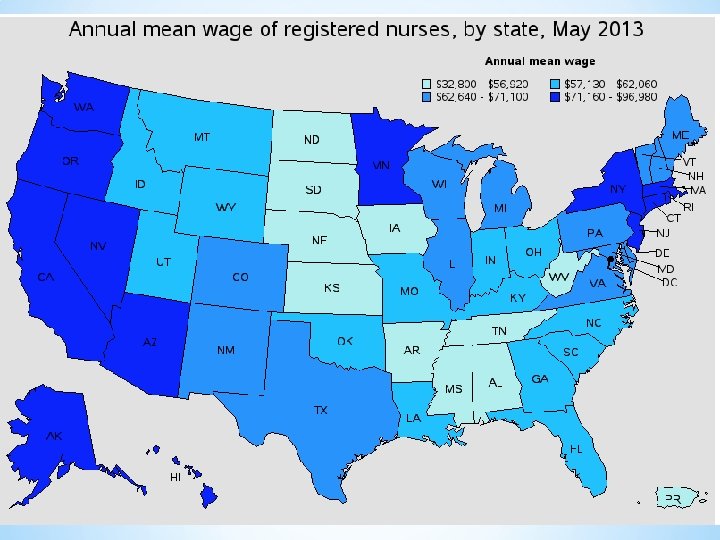
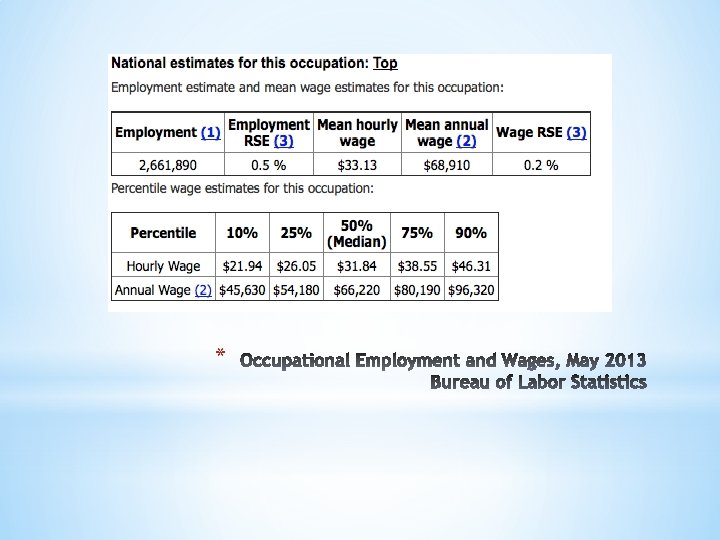
As the largest healthcare occupation, registered nurses held about 2. 6 million jobs in 2014. For registered nurses specifically, the Bureau of Labor Statistics anticipates 19. 4 percent employment growth and 526, 800 brand new jobs between 2012 and 2022. This tremendous growth, when compounded by a low unemployment rate, just 2. 6 percent, and good job prospects, helped registered nurse secure the No. 6 slot on the US News Best Jobs list. Nursinhttp: //www. amnhealthcare. com/uploaded Files/Main. Site/Content/Healthcare_Industry_Insights/Industry_R esearch/AMN%202012%20 RN%20 Survey. pdfg Employment *

* Gender Role Changes in Nursing A new study from the Unite. . .

Licensure in a Compact State, by where registered nurses live and work by Number Percent Live and work in same Compact State 791, 444 96. 0 Live in one Compact State and work in another Compact State 13, 537 1. 6 Live in a Compact State and work in non. Compact State 19, 681 2. 4 Total 824, 662 100. 0

2016 National Patient Safety Goals http: //www. jointcommission. org/standards_information/npsgs. aspx
 were established in 2002 to help accredited")
Background *The National Patient Safety Goals (NPSGs) were established in 2002 to help accredited organizations address specific areas of concern in regards to patient safety *The first set of NPSGs was effective January 1, 2003 *The Patient Safety Advisory Group advises The Joint Commission on the development and updating of NPSGs

The purpose of the National Patient Safety Goals is to improve patient safety in a variety of settings. The goals focus on problems with health care safety and ways in which they can be resolved. *

* *Comprised of a panel of widely recognized patient safety experts, including nurses, physicians, pharmacists, risk managers, clinical engineers, and other professionals with hands-on experience in addressing patient safety issues in a wide variety of healthcare settings *Advises The Joint Commission how to address emerging patient safety issues in NPSGs, Sentinel Event Alerts, standards and survey processes, performance measures, educational materials, and Center for Transforming Healthcare projects

* Changes for 2016 A NPSG focusing on safe clinical alarm management for hospitals and critical access hospitals was introduced in 2014 with a phased implementation *Phase one begins January 1, 2014 *Phase two begins January 1, 2016

*Began January 1, 2014 *Hospitals were required to: * establish alarm safety as organizational priority * identify the most important alarms to manage based on their own internal situations *

*Begins January 1, 2016 *Hospitals will be expected to: * develop and implement specific components of policies and procedures * educate staff in the organization about alarm system management *

Patient safety goals are deleted when they become a Joint Commission Standard of Care. *

Improve the accuracy of patient identification. *

NPSG. 01. 01: Use at least two patient identifiers when providing care, treatment and services. * For example, use the patient’s name and date of birth. This is done to make sure that each patient gets the correct medicine and treatment. • Applies to: Ambulatory, Behavioral Health Care, Critical Access Hospital, Home Care, Hospital, Laboratory, Nursing Care Center, Office-Based Surgery *

*NPSG. 01. 03. 01: Eliminate transfusion errors related to patient misidentification. Applies to: Ambulatory, Critical Access Hospital, Office-Based Surgery *

Improve the effectiveness of communication among caregivers. *

*NPSG. 02. 03. 01: Report critical results of tests and diagnostic procedures on a timely basis. * Get important test results to the right staff person on time. • Applies to: * Critical Access Hospital, Laboratory

Improve the safety of using medications. *

*NPSG. 03. 04. 01: Label all medications, medication containers, and other solutions on and off the sterile field in perioperative and other procedural settings. • Applies to: Ambulatory, Critical Access Hospital, Office Based Surgery *

*NPSG. 03. 05. 01: Reduce the likelihood of patient harm associated with the use of anticoagulant therapy. • Applies to: Ambulatory, Critical Access Hospital, Nursing Care Center *

*NPSG. 03. 06. 01: Maintain and communicate accurate patient medication information. • Applies to: Ambulatory, Behavioral Health Care, Critical Access Hospital, Home Care, Hospital, Nursing Care Center, Office-Based Surgery *

Reduce the harm associated with clinical alarm systems. * Make improvements to ensure that alarms on medical equipment are heard and responded to on time. * Clinical Alarm Safety

NPSG. 06. 01: Improve the safety of clinical alarm systems. * Make improvements to ensure that alarms on medical equipment are heard and responded to on time * Clinical Alarm Safety • Applies to: Critical Access Hospital, Hospital

Reduce the risk of health careassociated infections. *

*NPSG. 07. 01: Comply with either the current Centers for Disease Control and Prevention (CDC) hand hygiene guidelines or the current World Health Organization (WHO) hand hygiene guidelines. • Applies to: Ambulatory, Behavioral Health Care, Critical Access Hospital, Home Care, Hospital, Laboratory, Nursing Care Center, Office-Based Surgery *

*NPSG. 07. 03. 01: Implement evidencebased practices to prevent health careassociated infections due to multidrugresistant organisms in acute care hospitals. • Applies to: Critical Access Hospital, Hospital *

*NPSG. 07. 04. 01: Implement evidencebased practices to prevent central lineassociated bloodstream infections. • Applies to: Critical Access Hospital, Nursing Care Center *

*NPSG. 07. 05. 01: Implement evidencebased practices for preventing surgical site infections. • Applies to: Ambulatory, Critical Access Hospital, Office-Based Surgery *

* *NPSG. 07. 06. 01: Implement evidencebased practices to prevent indwelling catheter-associated urinary tract infections (CAUTI). • Applies to: Critical Access Hospital, Hospital (Note: This NPSG is not applicable to pediatric populations. Research resulting in evidence-based practices was conducted with adults, and there is not consensus that these practices apply to children. )

* Make sure that the correct surgery is done on the correct patient and at the correct place on the patient’s body. *Mark the correct place on the patient’s body where the surgery is to be done. *Pause before the surgery to make sure that a mistake is not being made. *

* *UP. 01. 01: Conduct a preprocedure verification process. • Applies to: Ambulatory, Critical Access Hospital, Office-Based Surgery

* *UP. 01. 02. 01: • Applies to: Mark the procedure site. Ambulatory, Critical Access Hospital, Office-Based Surgery

* *UP. 01. 03. 01: A time-out is performed before the procedure. • Applies to: Ambulatory, Critical Access Hospital, Office-Based Surgery

* In early 1999, The Joint Commission solicited input from a wide variety of stakeholders (e. g. , clinical professionals, health care provider organizations, state hospital associations, health care consumers) and convened a Cardiovascular Conditions Clinical Advisory Panel about the potential focus areas for core measures for hospitals. In May 2001, the Joint Commission announced four initial core measurement areas for hospitals, which included acute myocardial infarction (AMI) and heart failure (HF). *
 track a variety of evidence-based, scientifically-researched standards of care")
Accountability Measures (formerly Core Measures) track a variety of evidence-based, scientifically-researched standards of care which have been shown to result in improved clinical outcomes for patients. CMS (the Center for Medicare & Medicaid Services) established the Core Measures in 2000 and began publicly reporting data relating to the Core Measures in 2003. Currently, we report on 22 Accountability Measures. *

Accountability measures are quality measures that meet four criteria that produce the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them. The criteria for classifying accountability measures include: Research: Strong scientific evidence exists demonstrating that compliance with a given process of care improves health care outcomes (either directly or by reducing the risk of adverse outcomes). Proximity: The process being measured is closely connected to the outcome it impacts; there are relatively few clinical processes that occur after the one that is measured and before the improved outcome occurs. Accuracy: The measure accurately assesses whether the evidence-based process has actually been provided. That is, the measure should be capable of judging whether the process has been delivered with sufficient effectiveness to make improved outcomes likely. If it is not, then the measure is a poor measure of quality, likely to be subject to workarounds that induce unproductive work instead of work that directly improves quality of care. Adverse Effects: The measure construct is designed to minimize or eliminate unintended adverse effects. These criteria are based on The Joint Commission’s experience implementing and evaluating the outcomes of quality measures for more than a decade. The criteria provide a more rational approach to the process of collecting and reporting quality data. *
 Stroke Immunizations Hospital")
Acute Myocardial Infarction Heart Failure Pneumonia Perinatal Care Venous Thromboembolism (VTE) Stroke Immunizations Hospital Outpatient Measures * http: //www. jointcommission. org/core_measure_set s. aspx

*Critical pathways, also known as critical paths, clinical pathways, or care paths, are management plans that display goals for patients and provide the sequence and timing of actions necessary to achieve these goals with optimal efficiency. *More simply put, Clinical pathways (CPs) are decision-making tools designed to improve the quality of patient care processes and reduce costs. * http: //www. bing. com/images/search? q=critical+p athways+in+nursing&qpvt=critical+pathways+in+nursing&FORM =IGRE
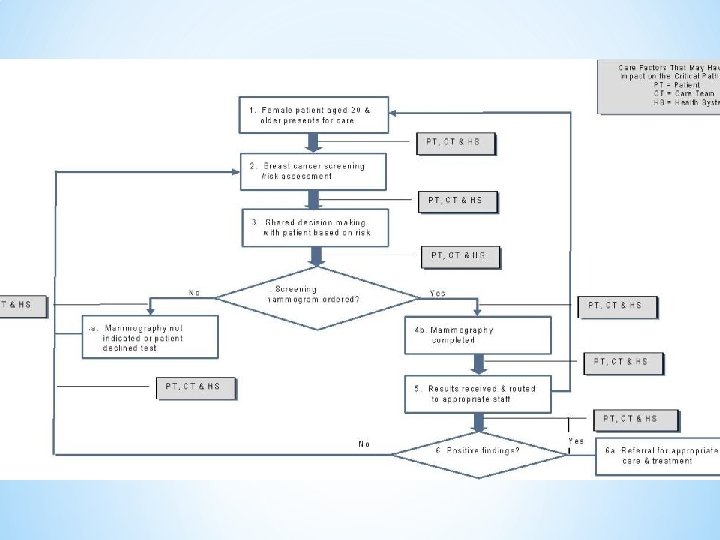

*A review of the literature suggest the use of critical pathways reduces the cost of care and the length of patient stay in hospital. They also have a positive impact on outcomes, such as increased quality of care and patient satisfaction, improved continuity of information, and patient education. *(Renholm, et. al. , Journal of Nursing Administration) *

* The median number of adult critical pathways used by academic * * hospitals, community teaching hospitals, and community hospitals was 25, 18, and 3, respectively. The most common pathways are community-acquired pneumonia, total hip or knee replacement, and stroke or transient ischemic attack. The percentage of hospitals with pathways dedicating staff to manage them was 78% for academic hospitals, 22% for community teaching hospitals, and 14% for community hospitals (P = 0. 02). Evaluation practices varied widely among hospitals with pathways. Measures assessed included monitoring length of stay (85%), total hospital costs (74%), in-hospital mortality (62%), infectious complications (53%), readmission rates (47%), functional status (18%), and adverse drug events (15%). Conclusion. The use of critical pathways varies substantially among hospitals participating in quality improvement consortia. Use was highest in academic centers and lowest in community hospitals. Many hospitals with pathways do not track important clinical outcomes as part of their evaluation practices. (Jonathan Darer, Effective Clinical Practice, American College of Physicians, Bethesda, MD). *

* * Mc. Cue, et. al conducted a retrospective analysis to determine whether multidisciplinary CPs had improved core measure scores. Comparative data to document secular trends were obtained from 45 Maryland hospitals. There were 6013 discharges with community-acquired pneumonia (CAP), congestive heart failure (CHF), or acute myocardial infarction (AMI) for the 3 -year data collection period ending in 9/30/05. The 72. 5% of cases in which CPs were employed to manage CAP, CHF, or AMI were significantly more likely to meet the Appropriate Care Measure (ACM) standards than the 26% that did not (81% vs. 67. 8%, p <. 001). Scores for all 10 ACM components for CP-managed patients were better than Maryland state averages. Improvements were stable over a 3 year period of time. (Journal of Healthcare Quality) *
 is part of the Centers for Medicare & Medicaid")
* Hospital Value-Based Purchasing (VBP) is part of the Centers for Medicare & Medicaid Services’ (CMS’) long-standing effort to link Medicare’s payment system to a value-based system to improve healthcare quality, including the quality of care provided in the inpatient hospital setting. * The program attaches value-based purchasing to the payment system that accounts for the largest share of Medicare spending, affecting payment for inpatient stays in over 3, 500 hospitals across the country. *

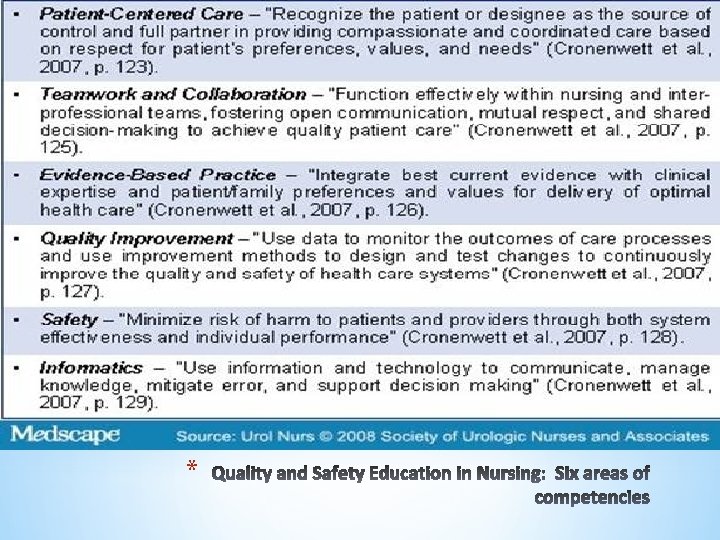
* The mission of QSEN is to address the challenge of assuring that nurses have the knowledge, skills, and attitudes (KSA) necessary to continuously improve the quality and safety of the healthcare systems in which they work. QSEN is a national movement that guides nurses to redesign the ‘what and how’ they deliver nursing care so that they can ensure highquality, safe care. Linda Cronenwett, Ph. D, RN, FAAN, the founder of QSEN, often states that QSEN helps nurses to identify and bridge the gaps between what is and what should be and helps nurses focus their work from the lens of quality and safety. *
: Errors arising from decisions that affect organizational policies, procedures")
Latent Failure (the blunt end): Errors arising from decisions that affect organizational policies, procedures and allocation of resources. Also included are management, organizational culture, protocols/policies, transfer of knowledge Active failure (the sharp end): Errors arising from direct contact with the patient (i. e. memory failures, attentional failures, competing demands, fatigue). *

Organization: Safety is a priority. Teamwork, patient involvement, transparency and accountability are key. Individual (i. e. Nurse): Decrease dependence on memory and vigilance. Avoid Vigilance: checklists, well-designed alarms, rested Avoid Memory: Standardizing and simplifying procedures and tasks. Plan and problem-solve! *
 Environment (staffing levels and skills, workload and shift patterns,")
Equipment (design, availability and maintenance) Environment (staffing levels and skills, workload and shift patterns, administrative and managerial support, physical space) Processes: As the problem was developing, when were key factors occurring? Management/Organization: (financial resources and constraints, organizational structure, policy standards and goals, safety culture and priorities) Regulation: (economic and regulatory situation, availability and use of protocols, availability and accuracy of tests) People/Teamwork: (knowledge and skills/training, competence, physical and mental health, verbal and written communication, supervision and assistance) *
 *")
Standardize/Simplify/Make Protocol Automation/Computerize Education/Training Improve or Change Devices/Equipment Communication Other (Describe) *





- Slides: 81