Treatment Treatment range from simple enucleation and curretage




















 of dental tissue, it is not")







- Slides: 29
Treatment • Treatment range from simple enucleation and curretage to block resection.
Calcifying epithelial odontogenic tumor • Benign , locally aggressive tumor originated from the rest of dental lamina and/or REE. • Rare tumor ( Less than 1%) , could be mistaken with poorly differentiated squamous cell carcinoma
• • Calcifying epithelial odontogenic tumor Clinically : Affect adult , 40 years. More common in the mandible Molar and premolar region crown of the unerupted teeth. Either central or peripheral Intraosseous lesion mainly produce slowly growing painless mass at the mandible. • Nasal obstruction is some time present in the maxillary lesion. • Peripheral ( Extraosseous) is most commonly present in the anterior part of the mouth.
Calcifying epithelial odontogenic tumor • Radiograph: The lesion appears as radiolucent area with poorly defined margin with fine flecks of radio-opacities (due to calcification). Impacted tooth and flicks of calcification
Histopathology • the Pindborg tumor is quite unique. • islands, strands, or sheets of epithelial cells in a fibrous stroma. • Large areas of amorphous eosinophilic hyalinized (amyloid-like) material are also present. • Calcifications, which are a distinctive feature of the tumor, develop within the amyloid-like material.
• Treatment: • Conservative local resection is the treatment of choice as these lesions are typically less aggressive than the ameloblastoma. • With this treatment the recurrence rate is approximately 15 % and the overall prognosis is good
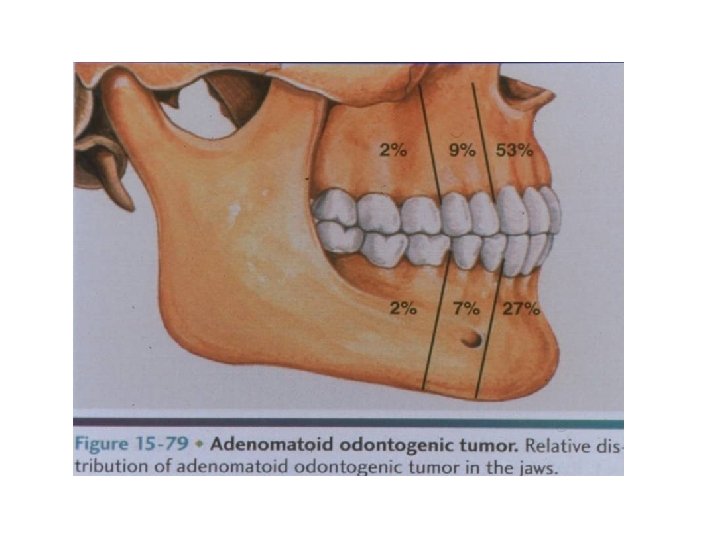
Adenomatoid tumor • Uncommon benign tumor, originated from reduced enamel epithelium during enamel development 3 -7% of all odontogenic tumors REE
Adenomatoid tumor • • • Clinical feature : Associated with an impacted. Asymptomatic Late adolescent or young adulthood. Female. 65% in the maxilla 75% associated with impacted teeth Small slow growing mass on the anterior maxilla, rarely premolar Cause an elevation of the upper lip. Pain and tooth placement. Rarely extra-osseous (Gingival) Radiolucent area surrounding impacted tooth
Adenomatoid tumor Radiography: • AOTs typically appear as pericoronal radiolucencies, which may have radiopaque material (“snowflake” calcifications) within the lucency lesion appears as a wellcircumscribed unilocular radiolucency that involves the crown of an erupted tooth, frequently a canine. radiolucency extend beyond the cementoenamel junction
Adenomatoid tumor • Histopathology: • Sheets or islands of epithelial cells arrange around microcyst ( Ducts or ductules ). • • • Surrounded by thin vascularized stroma. The ductules bordered by ameloblast like cells. The lumen filled by homogenous eosinophilic material. Small foci of calcification. •
TREATMENT � Histologically, the adenomatoid odontogenic tumor is a welldefined lesion that is usually surrounded by a thick fibrous capsule � Owing to this lesion being encapsulated, it separates easily from the surrounding bone. As such, an enucleation and curettage surgery is curative
Calcifying odontogenic cyst • Uncommon. • Developed from odontogenic epithelial remnants within gingiva, mandible, or maxilla. • Affect young patients. • More in females. • Mostly seen in maxilla. • The central (intraosseous ) lesions cause painless expansion of the buccal and lingual cortics. • Rarely, peripheral (extraosseous ) mass presence
Radiographically • Unilocular or multilocular radiolucency with well demarcated margins. • May be associated with crown of unerupted tooth. • Scattered irregular sized calcifications may be seen within the radiolucency. large radiolucency in the posterior maxilla. Calcifying odontogenic cyst. Maxillary radiolucent lesion containing calcifi ed structures.
• A well-defined cystic lesion is found with a fibrous capsule and a lining of odontogenic epithelium. • In some cases, the epithelial lining proliferates into the lumen so that the lumen is largely filled • The epithelial lining similar to that of ameloplastoma composed of outer layer of palisaded columer basal cell and inner layer of stellate reticulum • Presence of ghost cells (enlarged eosinophilic cells without visible nuclei) within the stellate reticulum –like area.
Calcifying odontogenic cyst. The cyst lining shows ameloblastoma-like epithelial cells, with a columnar basal layer. Large eosinophilic ghost cells are present within the epithelial lining.
Benign mixed odontogenic tumors Ameloblastic fibroma • Rare biphasic tumor, because the epithelial and mesenchymal components are part of the neoplastic process. • Resembles dental papillae
• • Clinical feature: Young adult and children. 70% in mandible frequently located at mandibular molar area, often over an unerupted tooth
• Radiography: • Generally, these lesions appear as either a unilocular or multilocular radiolucency. • They tend to be welldefined and may have a sclerotic border. • Approximately, 50 % are associated with an unerupted tooth.
Ameloplastic fibroma • Histopathology : • Microscopically characterize by thin strand cords of odontogenic epithelium that resemble dental lamina at the cap and bell stages of early odontogenesis. • The background compose of loose but cellular fibromyxoid connective tissue wildly separated by fibroblast, which resemble the immature dental papillae.
Odontomas • Odontomas are developmental malformation ( hamartoma) of dental tissue, it is not neoplasim Compound 1. Compound: Composed of multiple small tooth-like structures. 2. Complex: composed of a conglomerate mass of enamel and dentin, which bears no anatomic resemblance to a tooth Complex
Odontomas • Clinical feature : • 70% of odontogenic tumor. • More common in the maxilla. • The compound type is more often in the anterior maxilla. • complex type occurs more often in the posterior regions of either jaw. • Most odontomas are small and do not exceed the size of a normal tooth in the region.
Compound odontoma • many small teeth • Most common sites are anterior maxilla
Complex odontoma • disordered mass of dental hard tissue • Most common site are posterior mandible or maxilla Treatment ; • Odontomas are treated with simple enucleation and curettage. • Not known to recur.
Odontomas • Histopathology: • The compound odontoma is composed of enamel, dentin and cementum arrange in recognizable tooth forms; some enamel matrix may be retained in immature and hypomineralized specimens. • The complex odontoma is composed of enamel, dentin and cementum but these tissues are arranged in a random manner that bears no morphological resemblance to a tooth. Compound Complex
Benign mesenchymal odontogenic tumors Odontogenic fibroma • Benign neoplasm derived from connective tissue of odontogenic origin containing widely scattered islands and strands of embryonic odontogenic epithelium and calcification. Two types: 1. Central ( Intraosseous) type odontogenic fibroma. 2. Peripheral odontogenic fibroma. Peripheral odontomas
Odontogenic fibroma • Uncommon • Patient age ranged from 9 -80 years old with a mean of 40 years. • More common in Female • 60 % in the maxilla , anterior to the first molar. • In the mandible, 50 % occur in the posterior jaw. • Small lesion usually asymptomatic. • The larger associated with localized bony expansion or with the loosening of adjacent teeth
Odontogenic fibroma. • Histopathology: • The odontogenic fibroma appears as a fairly cellular fibrous connective tissue with collagen fibers arranged in interlacing bundles.