Treatment of the Acromioclavicular Joint Dislocation with External















")
")
 Affected side")




- Slides: 24
Treatment of the Acromioclavicular Joint Dislocation with External Fixation Device Chelnokov A. N. Tyrtseva E. S. Ural Scientific Research Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia
Background • To date there has been no consensus about optimal treatment of the traumatic dislocation of the acromio-clavicular joint.
Many treatment modalities for the ACJ dislocation • From aggressive surgery…
…to nonoperative management – A Prospective Evaluation of Untreated Acute Grade III Acromioclavicular Separations. T. F. Schlegel. The American Journal of Sports Medicine 29: 699 -703 (2001): – 20 of the 25 patients completed the 1 -year evaluation and strength-testing protocol; – objective examination and strength testing of the 20 patients revealed no limitation of shoulder motion in the injured extremity and no difference between sides in rotational shoulder muscle strength
• Aim of this study was to estimate capabilities of small wire monolateral external fixator for closed treatment of complete acromioclavicular dislocations.
Material and methods 6 10 8 • 24 patients – 14 male – 10 female • 3, 2 days after the injury (0 -14)
External Fixation • G. S. Sushko, G. A. Ilizarov, 1977, 1979
Surgery and post-op period • 10 -30 minutes • Regional anesthesia • Discharge in 1 -2 days • Sling for 1 -3 days
Duration of fixation • 4 weeks for acute cases (fixation within 05 days after the injury), • 6 -8 weeks for delayed admission (6 -14 days) • In cases of dislocations older 2 weeks => AC and CC ligaments repair by tendon allografts • Stability test before hardware removal
Results • Self-care, light housework – 3 -5 days • Deep infection 0/24 – 10 patients (42%) sustained skin irritation and serum drainage from acromial wire site only • 23/24 healed – 1/24: missed acromial wire cut-out => symptomatic instability => AC+CC repair (allo tendons) => uneventful healing • 1 year follow up - 15 patients. – All restored their pre-injury status – Occasional pain in hyperabduction – 3/15
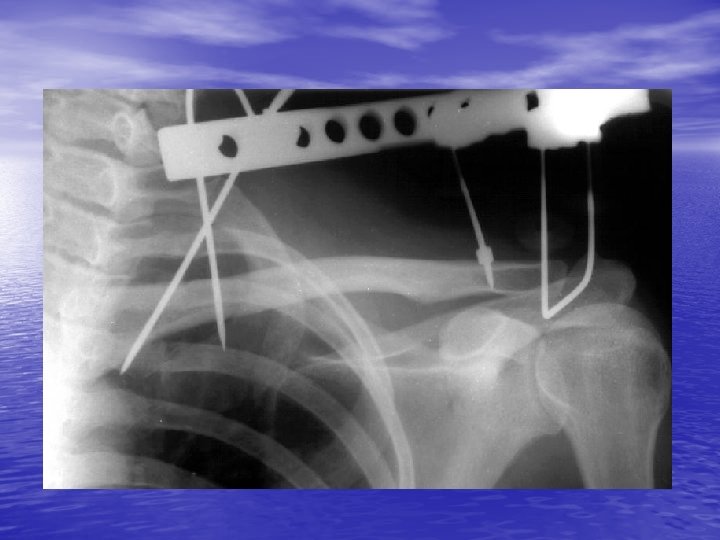
Rockwood type V injury
After 6 weeks
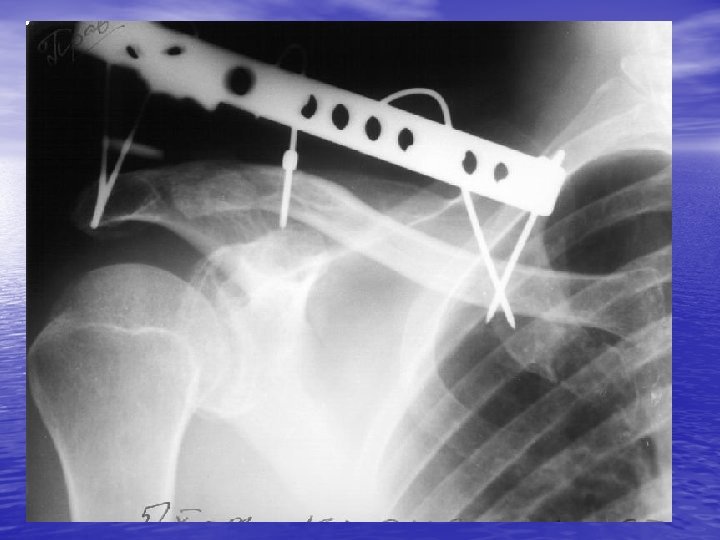
Result
Neer Type II injury
Follow-up (3 year)
Follow-up (3 year)
Follow-up (3 years) Affected side
Discussion: Advantages of the technique • Controllable fixation – With ex-fix we control the situation, without it the situation controls us • Minimally invasive – Fast recovery – Good cosmetic effect • Minimal time and efforts • Short learning curve
Discussion: Disadvantages • Temporary discomfort, decreased quality of life • Pin site care, outpatient visits necessary • Hardware removal
Conclusion • External fixation can be technique of choice for acute cases where operative treatment is indicated
Thank you http: //weborto. net