TREATMENT OF CONGESTIVE HEART FAILURE CHF DIGITALIS GLYCOSIDES
 DIGITALIS GLYCOSIDES AND OTHER POSITIVE INOTROPIC AGENTS")





 dobutamine digoxin ACEI spironoloactone ARB Phosphodiesterase III")













, at doses equal to")
 Inhibitors (amrinone & milrinone) c. AMP They increase Ca indirectly Phosphodiesterase")

 ACEIs")


 ACEI ↓angiotension II ↑bradykinin ↓sympathetic* vasodilation ↓aldosterone Decreased sodium")

 Physiologic functions of AT 1 receptors according to")
 n Agents include: Losartan and Valsartan n They are recently")
 n ARBs have the same side-effects of ACEIs, except they")
- Slides: 32
TREATMENT OF CONGESTIVE HEART FAILURE (CHF) DIGITALIS GLYCOSIDES AND OTHER POSITIVE INOTROPIC AGENTS
Common Diseases Contributing to CHF Ø Cardiomyopathy - Ø Hypertension Ø Myocardial ischemia & infarction Ø Cardiac valve disease Ø Coronary artery disease
Clinical Features of CHF Ø Reduced force of cardiac Ø Ø contraction Reduced cardiac output Reduced tissue perfusion Edema (congestion) Increased peripheral vascular resistance
n Important definitions : n Afterload: pressure exerted on the left ventricle during systole which is dependent on the peripheral vascular resistance. n Preload : end-diastolic pressure when the ventricle has become filled. (depend on venous return, venous pressure, and blood volume)
As compensation mechanism the heart will increase the incoming volume of blood so the heart can eject more blood The heart can’t eject blood , so it remains inside the heart after systole Congestive Heart Failure Events Dilated heart ischemia of cardiomyocytes ↓contraction ↑ afterload ↑ preload
The Pharmacologic Rationale Which type of drugs do we choose to treat this disease β blockers to decrease sympathetic activity. Especially HR to increase diastolic time To refill left ventricle Positive inotropic drugs to increase contractility Diuretics to relieve the edema ACEI or ARB to inhibit the action of anigiotensin
Drugs used in HF Noninotropic Inotropic (cardiotonic) dobutamine digoxin ACEI spironoloactone ARB Phosphodiesterase III inhibitors βblockers diuretics Used in acute or decompensated HF
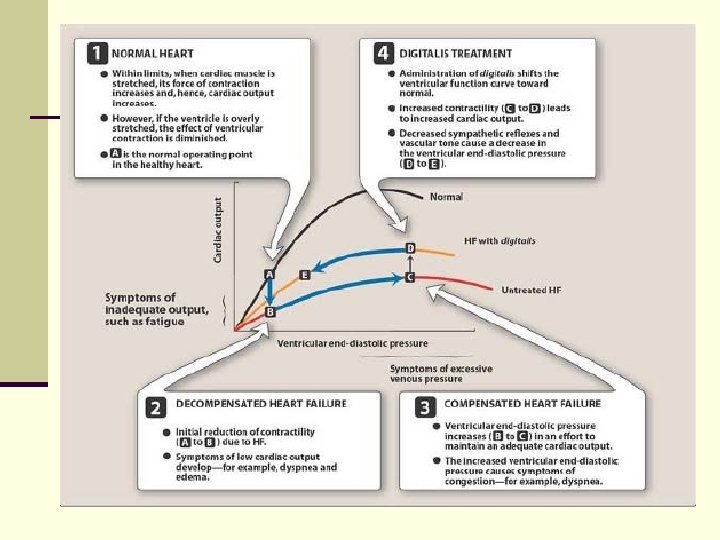
CARDIOTONIC DRUGS Cardiac Glycosides Cardiac glycosides: drugs used in treatment of CHF and cardiac arrhythmia n Mechanism of the beneficial positive inotropic pharmacodynamic effect n The principal beneficial effect of digitalis in CHF is the increase in cardiac contractility (+ve inotropism) leading to the following: increased cardiac output decreased cardiac size (via ↓EDV & ↓ ESV) decreased venous pressure and blood volume diuresis and relief of edema (due to ↑ CO & ↓capillary permeability) o Decrease O 2 consumption. o o
Physiology of contraction As you know 1 st the cell depolarizes then contraction occurs In depolarization Ca++ will enter the cell Ca++ will trigger the release of Ca++ from the sarcoplasmic reticulum In repolarization Ca++ will return to the sarcoplasmic reticulum Intracellular Ca++ leaves by means of Na/Ca exchanger Intracellular Na leavs by means of Na/ K ATPase
continued Na/Ca exchanger depends on Na electricgradient Inside the cell outside Less Na More Na Na Na/K ATPase K Na Ca Na/Ca exchanger This exchanger operates bidirectionally In repolarization In depolarization Ca++ in Na+ out Ca++ out Na+ in
Mechanism of action of cardiac glycosides Cardiac glycosides Inhibit Na/K ATPase ↑ intracellular Na Inhibition of Na/Ca exchanger ↑intracellular Ca ↑contractility
Pharmacological Actions of Digitalis Glycosides pharmacokienetics Moderate binding to plasma protein Good oral absorption Excreted through kidney (slow the elimination ) Not stable in blood because in heart failure there is relative renal impairment* Ø Inotropism. Digitalis exerts positive inotropic effect both in the normal and failing heart via inhibition of Na+-K+ATPase at the cardiac sarcolemma. Cardiac output (CO) Ø Digitalis increases the stroke volume and hence the CO Ø No increase in oxygen Consumption Ø Decreased EDV & hence the dilated cardiac muscle I.
II. Heart Rate Digoxin can decrease heart rate by : 1 - slowing SA nodal firing rate 2 - slowing AV conduction. 3 - increase refractory period. Mechanism of action Indirect –vagaleffect through Direct -extravagal-effect on the heart (parasympathomimetic) -slowing SA node firing rate -slowing AV conduction and prolongation of refractory period of AV node ↑ sensitivity of SA node to vagal stimulation thus decrease in firing rate Stimulation of vagal central nuceli
III. Venous Pressure digitalis ↑contractility ↑circulation and perfusion ↓venous pressure ↓EDV IV. Diuresis digitalis ↑cardiac output ↑renal blood flow and so GFR ↓renin angiotensin system edema relieved V. Myocardial Automaticity/Conductivity Ø At high doses, automaticity is enhanced as result of the gradual loss of the intracellular K+
Therapeutic Uses of Digitalis Glycosides q Treatment of congestive heart failure which does not respond optimally to diuretics or ACEI. q Treatment of atrial fibrillation and flutter by slowing SA nodal firing rate as well as AV conduction preventing the occurrence of the life-threatening ventricular arrhythmias. q So we use digitals to treat atrial fibrillation and flutter because they slow automaticity.
Adverse Effects of Digitalis Glycosides i. Ventricular Arrhythmias Digitalis ↑ intracellular Ca ↑ Ca in sarcoplasmic reticulum (become saturated) Result in oscillating in Ca levels inside the cell oscillatory after potential n Arrhythmias resulting from oscillatory after potentials include single and multiple ventricular premature beats and ventricular tachy-arrhythmias
Adverse Effects of Digitalis Glycosides CNS side-effects iii. Gynecomastia n Stimulation of the vagal n Gynecomastia may occur center and chemoreceptor in men either due to trigger zone (CTZ) results peripheral esterogenic in nausea, vomiting, actions of cardiac diarrhea & anorexia glycosides or hypothalamic stimulation n Other CNS effects include blurred vision, headache, dizziness, fatigue, and hallucinations ii. iv. ↓conduction velocity (AV block)
Treatment of Digitalis Toxicity Immediate withdrawal of digitalis I. V. K+ supplementaion to compensate for ↓intracellular K. This may lead to Hyperkalemia ↓slope of phase 4 ↓ automaticity Complete AV block (contraindicated in digitalis induced heart block)
continued If that doesn’t work Lidocaine or phenytoin is effective against K+ digitalis-induced dysryhthmias If that doesn’t work (severe case or resistance to drugs) Use digoxin’s specific Fab fragments • They are antibodies against digoxin. • Produced from sheep(we give the sheep digoxin and then get the antibodies produced against it). • We separate the Fab portion from Fc portion by papain • Fab portion is not antigenic thus, it doesn’t cause allergy (not produced anaphylactic shock). • Antibody will bind to digoxin forming a complex which can be excreted through the kidneys increasing renal blood flow
Digoxin-specific Fab fragments n Digoxin-specific Fab fragments are used safely for Ø Ø the treatment of the life-threatening cardiac glycosidesinduced arrhythmias and heart block Digoxin-specific Fab fragments are produced by purification of antibodies raised in sheep by immunization against digoxin The crude antiserum from sheep is fractionated to separate the Ig. G fraction, which is cleaved into Fab and Fc fragments by papain digestion The Fab fragments are not antigenic and with no complement binding They are excreted fairly rapidly excreted by the kidney as a digoxin-bound complex
Selective ß 1 - Adrenergic Agonists n Dobutamine (and dopamine), at doses equal to or less n o o than 5 µg/kg/min, have selective ß 1 - adrenergic agonistic activity. Beneficial effects in emergency treatment of acute CHF (decompensated ) include the following: 1 - Increased cardiac output as a result of enhanced contractility without appreciably altering the heart rate. 2 - Reduction of mean arterial blood pressure. 3 - Lowering of the total peripheral vascular resistance and consequently decreasing the afterload? ? Read slide #3 4 - Reduction of ventricular filling pressure dobutamine G- protein receptor Adenlyl cyclase c. AMP PKA
Phosphodiesterase III (PD-III) Inhibitors (amrinone & milrinone) c. AMP They increase Ca indirectly Phosphodiesterase III PD-III inhibitors n PD-III inhibitors are suitable only for acute CHF because they can induce life-threatening arrhythmias on chronic use same ß 1 - Adrenergic Agonists Dobutamine and PD-III inhibitors are taken parenteral and act in a short period
OTHER DRUGS OF USE IN CHF WITHOUT INOTROPIC EFFECT Diuretics n Diuretics ↓cardiac preload by inhibiting sodium and water n n n o retention Cardiac pumping improves with the consequent reduction in venous pressure relieving edema Thiazide (e. g. , hydrochlothiazide) and loop diuretics (e. g. , frusemide) are routinely used in combination with digitalis Potassium-sparing diuretics can be concurrently used to correct hypokalemia Spironolactone+Digitalis+ACEI ↓mortality because spironolactone antagonize aldosterone which cause myocardial and vascular fibrosis
Angiotensin Converting Enzyme Inhibitors (ACEIs) ACEIs
n Action of AT 1 receptor: 1 - vasoconstriction of veins and arteries. 2 - release of aldosteron in renal cortex. 3 - sympathetic activity by NE in nerve terminal. 4 - hypertrophy of the heart. Action of AT 2 receptor: 1 - release of NO so vasodilatation. 2 - prevent hypertrophy.
Effect of ACEIs on Bradykinin Angiotension II activate sympathetic nervous system in the brain and synapses
Angiotensin Converting Enzyme Inhibitors (ACEIs) ACEI ↓angiotension II ↑bradykinin ↓sympathetic* vasodilation ↓aldosterone Decreased sodium and water retention n Ultimately both preload and afterload are reduced n Clinical trials showed that the use of ACEIs in CHF has significantly reduced morbidity and mortality
Adverse Effects of ACEIs n 1. Postural hypotension n 2. Hyperkalemia n 3. Renal insufficiency (don’t forget that in heart failure there is renal insufficiency caused by decrease renal blood flow but still we use ACEI) n 4. Persistent dry cough n 5. ACEIs are contraindicated in pregnancy Ø ACEIs include agents like: captopril, enalapril, lisinopril and many others
Angiotensin II Type-1 Receptor Antagonists (ARBs) Physiologic functions of AT 1 receptors according to their location LOCATION FUNCTION Kidney Glomerulus Mesangial cell contraction ↓GFR Proximal tubule Increased reabsorption of sodium Juxtaglomerular apparatus Decreased renin secretion Heart Inotropic effect and release of growth factors with ensuing stimulation of cardiac myocyte hypertrophy and increased extracellular matrix production Blood vessels Vasconstriction with an increase in afterload as well as local release of growth factors Adrenal gland Aldosterone and catecholamine release Brain Vasopressin release, stimulation of thirst; autonomic activity and cardiovascular reflexes Sympathetic nervous system Increased sympathetic outflow
AT-1 Receptor Blockers (ARBs) n Agents include: Losartan and Valsartan n They are recently approved for treatment of CHF n They have the same beneficial effect of ACEIs except they don't increase bradykinin. n They don’t cause cough n They enhance AT-2 function.
AT-1 Receptor Blockers (ARBs) n ARBs have the same side-effects of ACEIs, except they don’t cause cough. Nitrovasodilators n Sodium nitroprusside I. V. infusion is used at a dose of 0. 1 - 0. 2 µg/kg/min only in acute CHF to lower preload and afterload. n Nitrates can be used also to decrease preload (nitrates and hydralazine were used to decrease preload and afterload).