TREATMENT OF ABNORMAL BEHAVIORS AP PSYCHOLOGY Mental Health

TREATMENT OF ABNORMAL BEHAVIORS AP PSYCHOLOGY

Mental Health Practitioners � Psychiatrist: MD, an prescribe medication, perform surgery. ü Generally take a biological approach to treating mental illness. ü Do not take training in other methods of psychological treatment � Clinical Psychologists: Ph. D. or Psy. D. , training emphasizes otherapeutic treatments of psychological disorders. ü often work with psychiatrists to treat patients with supportive psychotherapy & medicine.
 � Counseling Psychologists: usually have advanced degrees & tend to")
Mental Health Practioners (cont’d) � Counseling Psychologists: usually have advanced degrees & tend to deal with less severe mental health problems in college settings or in marital & family therapy practices. � Psychoanalysts: may or may not be psychiatrists, but follow the teaching of Freud & practice psychoanalysis or other psychodynamic theories. � Clinical or Psychiatric Social Workers: usually have a master’s degree in social work (MSW)

History of Therapy � Trephining: early humans thought that the mentally ill were possessed by evil spirit so they drilled holes in their heads to let the spirits out. � Middle Ages: mentally ill possessed by demons of Satan. Victims were punished with exorcisms or tested by drowning & burning. � Dorthea Dix (19 th cent): humane treatment of mentally ill. Created separate institutions for them & pioneered more individualized & kinder treatment strategies.

Deinstitionalization � Resulted from overcrowding in mental institutions in the 1950 s. � With the use of better psychotropic drugs, patients, not considered a threat to themselves or others were released from mental hospitals. � Goal was that patients would improve more rapidly in familiar community settings. � 1960 s, Congress passed legislation to establish community mental health facilities � Negative consequence: homeless population, many of which are thought to be schizophrenic patients, mostly off their meds & in need of care.

Treatment Approaches � No one approach for treatment of mental disorders appears to be ideal. � An eclectic approach uses techniques from various forms of therapy to fit the client’s problems, strengths, and preferences. � Medications and psychotherapy can be used together, and may help the each other achieve better reduction in symptoms. � Meta-Analysis: Systematic statistical method for synthesizing the results of numerous research studies dealing with the same variables. � Such studies indicate that clients who receive psychotherapy are better off than most of those who receive no treatment.

Psychoanalysis Freud believed that abnormal behavior was the result of unconscious conflicts from early childhood trauma experienced during the psychosexual stages of development. � Involves going back to discover the roots of problems by bringing the conflict into the conscious mind, helping the client gain insight & achieve personality change. � Free association: the patient speaks freely about memories, dreams, feelings � Interpretation: therapist suggests unconscious meanings and underlying wishes to help the client gain insight and release tension

Interpretation in Psychoanalysis

Psychodynamic Theory Catharsis: release of emotional tension after remembering or reliving an emotionally charged experience from the past, which may ultimately result in relief of anxiety. Traditional psychotherapy is too expensive & requires too much time for most people seeking psychological help. Psychodynamic Psychotherapy Shorter in duration, less frequent, with the client sitting up & talking to therapist. Some therapists are more actively involved with patients, talking to them & pointing out associations to gain greater insights. Believe that anxieties are rooted in past experiences, but do not necessarily assume problems stem from infancy or early childhood.
 A further extension of psychotherapy often used to effectively treat depression")
Interpersonal Psychotherapy (IPT) A further extension of psychotherapy often used to effectively treat depression IPT is based on the premise that interpersonal distress is connected with psychological symptoms. The goal is less focused on insight, and more on relational behavior change and symptom relief. The focus is less on the past, and more on current feelings & relationships including interactions with therapist.

Humanistic Therapies Insight therapies: aimed at improving psychological functioning by increasing a person’s awareness of underlying motives & defenses. ü includes psychodynamic & humanistic therapies ü found to be effective for treating disorders, depression, and marital problems. Humanistic therapies focus on: Boosting people’s self-fulfillment by helping them grow in self-awareness & self-acceptance. Promoting growth, not curing illness. Conscious thoughts rather than the unconscious Present & future rather than the past.
 Also known as person-centered therapy Non-directive therapy that focuses on")
Client-Centered Therapy (Carl Rogers) Also known as person-centered therapy Non-directive therapy that focuses on the person’s conscious self-perceptions Promoted Unconditional Positive Regard by providing an atmosphere of acceptance, empathy, & sharing, permitting the client’s inner qualities to surface, leading the patient to self-actualization. Also encouraged active listening where therapist listens to client & echoes, restates, or clarifies to demonstrate empathy, showing the client that he/she was listening & understands what is being said. Therapy allows the client to take the lead in determining the direction of therapy.

Example of Client Centered Therapy Showing Empathy Through Active Listening Client-centered therapists show that they are tuning in to clients’ feelings and meanings. Summarize, paraphrase “So your father wasn’t around much? ” Invite clarification and elaboration “When you say ‘anxiety, ’ what does that feel like to you? What is going on in your body and thoughts? ” Reflect Feelings “It seems like you are disappointed; am I right? ”

Humanistic vs Psychoanalytic Therapies

Behavioral Therapy that applies learning principles to the elimination of unwanted behaviors. B. F. Skinner: abnormal behavior results from maladaptive behavior learned through faulty awards & punishments. Classical Conditioning Therapies Countercondioning: uses classical conditioning to evoke new responses to stimuli that are triggering unwanted behaviors.

Counterconditioning: Exposure Therapy Exposure therapies treat anxieties by exposing patients to things they fear and avoid. Mary Jones (1924): treats 3 year old Peter who is petrified of rabbits & other furry objects.

Counterconditioning: Systematic Desensitization Client was is taught progressive relaxation techniques With therapist, create an anxiety hierarchy from least to most feared stimulus. Therapy starts with client being introduced to the least fearful stimulus. When he/she can relax with this fear, the process is repeated. Usually takes about 10 sessions to desensitize a person to a phobia.

Counterconditioning: Virtual Reality Exposure Therapy is an anxiety treatment that gradually increases anxiety-triggering stimuli. Common approach to dealing with phobias.

Counterconditioning: Aversive Conditioning Trains the client to associate physical or psychological discomfort with behaviors, thoughts, or situations he/she want to stop or avoid the client directly confronts the anxiety provoking stimulus, extinction is achieved.

Operant Conditioning Therapies Behavior Modification: the client choses a goal, & with each step toward that goal, he/she receives a small reward until the goal is reached. ü Example: weight reducing programs such as Weight Watchers Token Economies: positive behaviors are rewarded with secondary reinforcers such as tokens or points that can be exchanged for extrinsic rewards ü often used in institutions to encourage acceptable behaviors or discourage unacceptable ones.

Other Behavior Therapies Social Skills Learning: based operant conditioning & Bandura’s social learning theory to improve interpersonal skills by using modeling, behavioral rehearsal, & shaping. ü Using modeling, the client observes socially skilled people in order to learn appropriate social behaviors through role playing in structured situations. üShaping reinforces increasingly more complex social situations üHelps people with social problems & former mental patients learn to cope in social situations.

Other Behavior Therapies Biofeedback: involves giving the person immediate information about the degree to which he/she is able to change anxiety-related physiological responses. ü Can provide the client with improved control of the physiological process & as a result lessen physiological arousal. Behavior therapies are effective in treating anxiety disorders, alcohol & drug addictions, bed-wetting, sexual dysfunctions & autism. Psychoanalysts believe that since Behaviorists are curing the symptoms, not the problem, the problem will eventually resurface in in another form.

Cognitive Therapy Cognitive therapy teaches people new, more adaptive ways of thinking. Based on the assumption that thoughts intervene between events our reactions. People interpret events. Their thoughts generate feelings emotions. Actions that follow are a result of these emotions and feelings. Event Thought Emotion Action
 Developed by Albert Ellis who believed that much of")
Rational Emotive Behavior Therapy (REBT) Developed by Albert Ellis who believed that much of defeatist thinking involves the tyranny of “shoulds” – what we believe we must do, rather than actually what is realistic or necessary. REBT vigorously challenges clients’ illogical, self-defeating attitudes & assumptions. ABCs of therapy: Actions, Beliefs about those actions, & Consequences of those Actions.

Aaron Beck: Therapy for Depression Cognitive Triad: looks at what a person thinks about his/her self, world, & future. Depressed people tend to have negative perceptions in all three areas. Therapy assisted clients to see how their depression was worsened by errors in thinking such as catastrophizing, (interpreting current events as signs of the worst possible outcome).
 One of the most commonly practiced therapies used today. CBT")
Cognitive Behavior Therapies (CBT) One of the most commonly practiced therapies used today. CBT combines cognitive therapy with behavior therapy in to change the way people think as well as the way the act. For example, using CBT, OCD clients are led to resist the urge to act on their compulsions, & to learn to manage CBT assumes that the vicious obsessional thinking. cycle of negative thoughts, feelings, behavior, and physiological feelings all reinforce each other, pushing the person into deeper depression and/or anxiety.

Group Therapy Assembles clients together in small groups with related needs. Therapist facilitates the groups to work on therapeutic goals together. Helps to know that others experience similar problems. Less expensive, shy, less verbal patients & those resistant in individual settings may find it easier to open up in a group. Peer feedback helpful for clients to gain insights into their own particular problems.

Couples and Family Therapy Treats the family or the couple as a system where each person’s actions trigger reactions of from others. Works with multiple family members to heal relationships & mobilize resources. Such therapy can serve as a training ground for families & couples to practice better communication skills that will lead to improved relationships.

Self-Help Groups Self-help groups are led by group members rather than by a therapist They can be larger than group therapy and have less interaction among members. The focus is on support rather than on working on goals as in group sessions Example ~Alcoholics Anonymous: clients get peer support & have an outlet to share their individual experiences.

Is Psychotherapy Effective? There are different measures of the value & effectiveness of psychotherapy: üwhether the client is satisfied üwhether the client senses improvement üwhetherapist sees improvement üwhethere has been an observable, measured change in initial symptoms What Causes Improvement? Even if clients do improve, is the improvement really caused by therapy? ü Results also may be attributed to: Regression to the mean, drifting from initial crisis back to an average state. ü The client’s motivation to appear better in order to please therapist or to justify the cost of therapy.
 To track the effectiveness of a therapy, there should be a")
Outcome Research (cont’d) To track the effectiveness of a therapy, there should be a comparison between an intervention group and a control, or if possible a placebo group. To measure effectiveness of a therapy, objective, observable measures of symptoms should be examined rather than relying on client or therapist perceptions. Smith et al. (1980) produced the first meta-analysis of some 475 psychotherapy outcome studies which shows the improvement of untreated individuals & psychotherapy clients. ü results indicated that the average therapy client ends up better off than 80% of the untreated individuals on waiting lists (to be treated)

Psychotherapy: Outcome Research People are more likely to improve with treatment Other studies echo the same sentiment that those NOT undergoing therapy do improve, however, those that DO undergo psychotherapy, are more likely to improve more quickly, with less chance of relapse. So the question remains: Which psychotherapy is going to be the most advantageous to a patient with his/her particular set of problems?

Results of Outcome Research Research indicates that NO one therapy is generally superior. Research also suggests clients seem equally satisfied; there is little connection between clinicians’ experience, training, supervision, & licensing and their clients’ outcomes. Behavioral conditioning therapies: better with specific behavior problems such as bed wetting, phobias, compulsions, marital problems, & sexual dysfunction. Psychodynamic therapy: success with depression & anxiety Cognitive & Cognitive-Behavior therapies: effective in coping with anxiety, depression, & PTSD.

Using Outcome Research in Therapy Evidence-Based Practice: clinical decision making that integrates the best available research with clinical expertise & patient characteristics & preferences. Available therapies should be rigorously evaluated & then applied by clinicians who are mindful of their skills & each patient’s unique situation.

Evaluating Alternative Therapies When new “therapies” emerge, they are often promoted with testimonials. PROBLEM: ü Are people better because of the intervention? ü There is no data on how many people received little to no benefit from the SOLUTION: ü Controlled studies with random assignment therapy and nonintervention conditions. CHALLENGE: ü Making sure interventions are performed by clinicians are trained in that area of therapy.
 Developed by Francine Shapiro (2007) while walking in")
Eye Movement Desensitization & Reprocessing (EMDR) Developed by Francine Shapiro (2007) while walking in the park & noticing that her anxious thoughts disappeared as her eyes darted about. ü Offered as an anxiety therapy, the clinician has the client imagine traumatic scenes while triggering eye movements by waving a finger in front of the client’s eyes in attempts to unlock and reprocess previous frozen traumatic memories. ü Shapiro’s studies (4) indicate that 84 -100% of single trauma victims get better within 3 90 minute sessions. Skeptics believe that what is therapeutic is the combination of exposure therapy & a robust placebo effect.

Light Exposure Therapy Research supports the idea that daily exposure to bright light, especially with a blue tint, is effective in treating the depressive symptoms of seasonal affective disorder [SAD].

Commonalities among Psychotherapies Therapeutic Alliance: a bond of trust & mutual understanding between a therapist & client who work constructively together to overcome the client’s problems. Three Elements Shared Psychotherapy also may offer: by all forms of ü a safe place to explore feelings, ideas, self. Psychotherapy ü Hope: therapists assume ü a source of ideas & options the client has resources that can be used for behaving & seeing recovery; improvement is things differently. possible ü exercises in behavioral, ü A new perspective: new cognitive, & emotional interpretations & change. narratives (“victim” to ü Affirmation of self , along “survivor”) can improve with support for change. mood and motivate change ü The relationship: empathy, ü a source of challenge& trust, & caring provide an enrichment to support environment for healthy neural growth and

Culture, Gender, & Values in Psychotherapy Differences become significant when a therapist from one culture or gender meets a client from another. Religion can be a source of conflict between therapist & client. Since therapists certainly differ in values, communication styles, & language, the APA offers accredited training programs in cultural sensitivity & actively recruits members in underrepresented cultural groups.

Biomedical Therapies Biomedical therapies refer to physically changing the brain’s functioning by altering its chemistry with medications, or affecting its circuitry with electroconvulsive shock, magnetic impulses, or psychotherapies. With a few exceptions, only psychiatrists (MDs) can offer biomedical therapies. Psychopharmacology: the study of the effects of drugs on mind and behavior.

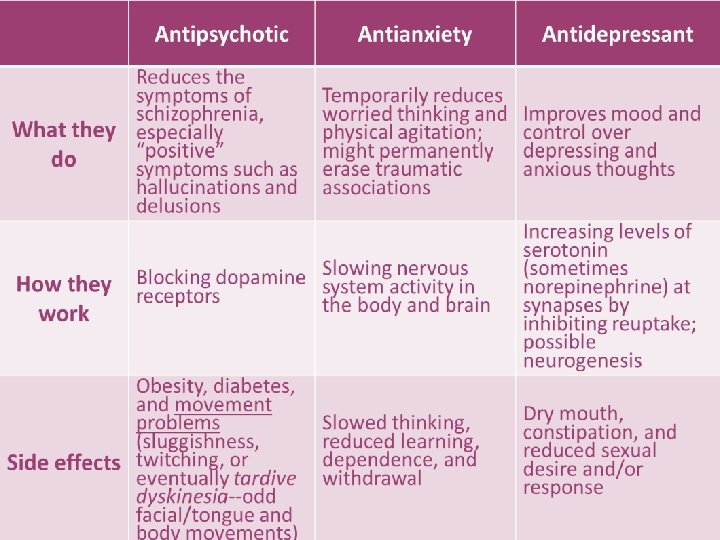
Antipsychotic Drugs Drugs used to treat schizophrenia & other forms of severe thought disorders. Examples include Thorazine, Haldol, & Clozaril, Risperdal, & Zyprexa. Most effective for positive symptoms of schizophrenia as they dampen responsiveness to irrelevant stimuli (lessen auditory hallucinations, delusions, agitated behaviors, & paranoia). Molecules of typical antipsychotic drugs are dopamine antagonists, blocking dopamine receptor sites to decrease neuron firing. Some antipsychotics produce sluggishness, tremors, & twitches similar to those of Parkinson’s disease Long term use can lead to tardive dyskinesia: involuntary movements of the facial muscles, tongue & limbs Newer drugs (risperdal & zyprexa) have less side effects but may cause obesity & diabetes.

Antianxiety Drugs Antianxiety drugs such as Xanax, Valium, & Klonapin depress CNS activity & are used to control anxiety & agitation. increase availability of GABA to the limbic system & reticular activating system where arousal is too high, reducing anxiety. Using visualization, relaxation, & time management can help to taper drugs off over time to minimize side effects & tolerance Often used in combination with psychological therapy. Side effects can include slowed thinking, reduced learning, dependence, and withdrawal In recent years, the rate of outpatient treatment for anxiety disorders, OCD, & PTSD has nearly doubled. Interestingly, the new standard for drug treatment of

Antidepressants Originally used to lift people up from a state of depression. Now, being used to successfully treat anxiety disorders, OCD, & PTSD Include Prozac, Zoloft, Paxil & are known as SSRIs (selective serotonin reuptake inhibitors). Work by increasing the availability of certain neurotransmitters such as norepinephrine & serotonin by blocking re-uptake at the synapse, which are often scarce when a person is depressed /anxious. Take 4 -6 weeks to be effective; side effects can include constipation, reduced sexual desire &/or response. Some of the older antidepressants are dual-action, blocking both norephinephrine & serotonin. These have greater potential side effects, including dry mouth, weight gain, hypertension, and/or dizzy spells.

Biology of Antidepressants

ü Mood Stabilizing medications are often used for bipolar disorder ü Lithium is effective in reducing the highs & lows of bipolar disorder but it also reduces the patient’s risk of suicide. ü Other mood stabilizers include anti -seizure medications such as Depakote, Tegretol, and Lamictal ü ADHD stimulants include methlyphenidate (Ritalin, Concerta) &
 Biomedical therapy for severely depressed patients in which a brief electric")
Electroconvulsive Therapy (ECT) Biomedical therapy for severely depressed patients in which a brief electric current is sent through the brain of an anesthetized patient. Used for depression when the patient does not respond to drug therapy Although researchers are not sure how ECT works, it may allow neural re-wiring & boost neurogenesis. Evidence some memory loss, but no discernable brain damage
 r. TMS is the application of repeated pulses")
Repetitive Transcranial Magnetic Stimulation (r. TMS) r. TMS is the application of repeated pulses of magnetic energy to the brain; used to stimulate or suppress brain activity. Patients are wide awake; performed over several weeks Produce NO seizures, memory loss, or other serious side effects. r. TMS sends a painless magnetic field through the skull to the surface of the cortex. Repeated stimulation may cause nerve cells to form new functioning circuits through LTP.

Psychosurgery removes or destroys brain tissue. Because its effects are irreversible, it is the most drastic & least used biomedical intervention for changing behavior. Lobotomy: cutting the nerves connecting the frontal lobes with the emotion-controlling centers of the inner brain. üThis decreases depression, but also destroys initiative, judgment, and cognition. No longer used as a psychotherapeutic method. Today, microscale psychosurgery may be helpful in disrupting problematic neural networks involved with aggression or obsessive-compulsive disorder.

Therapeutic Lifestyle Change We can indirectly affect the biological components of mental health problems. ü Exercise can boost serotonin levels and reduce stress. ü Changing negative thoughts can improve mood and even rewire the brain. ü Mental health problems also can be reduced by meeting our basic needs for sleep, nutrition, light, meaningful activity, and social connection.
- Slides: 50