TRAUMATIC PILONIDAL SINUS PRESENTATION BY BALAMURUGAN E 1

? TRAUMATIC PILONIDAL SINUS PRESENTATION BY BALAMURUGAN E 1 ST YEAR PG, S 5 UNIT GUIDE: DR. A. ANVAR ALI M. S. PROFESSOR OF SURGERY

case

CASE SUMMARY �A 37 year old gentleman presented to OPD with c/o swelling in sub mental region following self fall in his home 6 months back �Sudden onset , not progressive �h/o pain present initially and subsides gradually �No h/o fever �No h/o pus discharge per se �No other swelling elsewhere in the body �No h/o loss of weight �Not a case of diabetic/hypertensive

On inspection �Spherical shaped Swelling of size 2*2 cm noted in sub mental region, �surface smooth �edge can be made out, �single in number, �non pulsatile, �no movement with deglutition or protrusion of tongue, �no impulse on coughing, �skin over swelling normal, no sinus , no scar �Oral cavity examination normal

Palpation �Not warmth �Not tender �Size, shape and extent as described �Skin over swelling not pinchable, Surface smooth �Edge can be palpated �Firm in consistency �No other swellings elsewhere in the neck

Diagnosis �Based on these findings , it was suspected to be ? Chronic abscess / ? Sub mental lymph node/ ? Foreign body granuloma

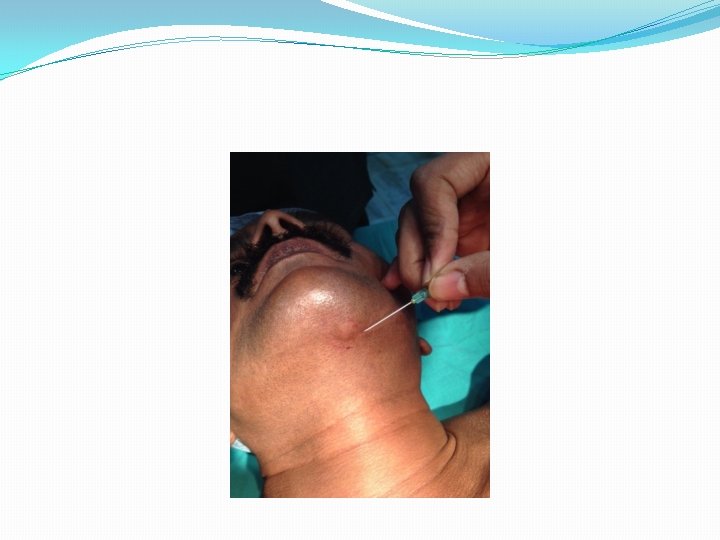
Management �Routine investigations were taken and it was found to be within normal limits �Xray neck – normal �Patient was taken to elective surgery- excision and biopsy after anaesthetic fitness �Speciment sent for HISTOPATHOLOGICAL study



Biopsy report

Report �Collection of inflammatory tissues in sub cutaneous plane �Also seen shaft of hair which is partially degenerating �IMPRESSION: TRAUMATIC PILONIDAL SINUS

Pilonidal sinus �Condition found in the natal cleft overlying the coccyx, consisting of one or more (usually) noninfected, midline openings communicates with fibrous track lined by granulation tissue and containing hair follicles within lumen �Combination of shearing force and friction allows dead fallen hair to pierce through midline skin

Sites of occurence �Inter digits �Axilla �Umbilicus �? Submentum

Clinical features �Intermittent pain �Swelling �Discharge through sinus

management �In acute exacerbation: broad spectrum antibiotics, antiseptic dressings incision and drainage

�CHRONIC PILONIDAL SINUS: Lay open of all tracks with or without marsupialisation excision of all tracks with or without primary closure

Recurrency �Part of sinus complex overlooked during primary operation �New hairs entered through scar �Persistence of midline wound : treated by revisional surgery-- re excision and wound closure by myocutaneous buttock flap(bascom’s procedure)

Thank you
- Slides: 19