Traumatic Brain Injury Jason A Demery Ph D

Traumatic Brain Injury Jason A. Demery, Ph. D. Department of Clinical & Health Psychology 04/17/06
![Defining Traumatic Brain Injury § Traumatic brain injury (TBI) is a [mechanically] induced disruption](http://slidetodoc.com/presentation_image_h2/9efb738a0d8e9e1d9b5d3add92ae1513/image-2.jpg "Defining Traumatic Brain Injury § Traumatic brain injury (TBI) is a [mechanically] induced disruption")
Defining Traumatic Brain Injury § Traumatic brain injury (TBI) is a [mechanically] induced disruption of brain functioning, from the head being struck [Acceleration; assault], head striking an object [Deceleration; fall], or the brain undergoing acceleration/deceleration movement w/o external trauma to the head [Pure Impulse Injury; whiplash] and characterized by: Ø Any period of loss of consciousness Ø Any anterograde or retrograde amnesia Ø Any alteration of mental state at the time of the accident (e. g. feeling dazed, disoriented, or confused) Adapted from The American Congress of Rehabilitation Medicine, 1993 § An insult to the skull, brain, or its covering, resulting from external trauma that produces an altered state of consciousness or anatomic motor, sensory, cognitive, or behavioral deficits. Chapter 381. 745 of the 2005 Florida Statutes

Prevalence & Incidence of TBI § Annual costs ~ $56 Billion Per 100, 000 § 5. 3 million Americans living with TBI-related disability CDC, 2004; TBI in the US: ED Visits, Hospitalizations and Deaths

Mechanisms of Injury in TBI CDC, 2004; TBI in the US: ED Visits, Hospitalizations and Deaths

Moderate & Severe TBI in Florida 2, 525 New TBIs in FY 2003 -04 BSCIP, 2004

Biomechanics of TBI
")
Primary Injury in TBI (Focal)

Interior Skull Surface Bony ridges The base of the skull is rough, with many bony protuberances. These ridges can result in brain injury during rapid acceleration. Injury from contact with skull

Cranial Vault and & Epidural & Subdural Spaces The brain requires a rich blood supply, and the space between the skull and cerebrum contains many blood vessels. These blood vessels can be ruptured during trauma, resulting in bleeding. Skull Dura Mater Arachnoid Layer Pia Mater Cerebral Cortex

Normal CT Scan of the Brain www. crash. lshtm. ac. uk

Acute Epidural Hematoma www. crash. lshtm. ac. uk

Evacuation of EDH

Evacuation of EDH

Acute Subdural Hematoma www. crash. lshtm. ac. uk

Acute SDH w/Midline Shift www. crash. lshtm. ac. uk

Evacuation of SDH

Evacuation of SDH

Cerebral Contusion www. crash. lshtm. ac. uk

Intracerebral Hemorrhage
")
Traumatic Subarachnoid Hemorrhage (t. SAH)
")
Primary Injury in TBI (Diffuse)

Diffuse Axonal Injury The brain is a complex network of interconnections. Critical nerve tracts can be sheared and stressed during an acceleration-type of injury. Diffuse axonal injury is a very serious injury, as it directly impacts the major pathways of the brain.

Diffuse Axonal Injury

Secondary Injury in TBI

Neuropathological Classification of TBI Primary injury Trauma • Scalp laceration/abrasion • Skull fracture • Primary axonal injury • Vascular - cerebral contusion - hemorrhage (ED, SD, IC, IV, t. SA) Immediate Delayed Secondary injury • Hypoxia/Ischemia - post-traumatic seizures - elevated intracranial pressure brain swelling & herniation hypotension respiratory failure

Herniation = Ischemia = Brain Death

The Level I Trauma Center § § § § Neurosurgery Service In-House Trauma Surgeon Neurosurgeon Promptly Available Continuously Staffed & Available OR ICU Equipment for Treating Neurotrauma Pts. Continuously available CT Scanner

Shands at UF State-Designated Level I Trauma Center § 9/03 - Applied for L 1 TC Status § 9/04 - Provisional Approval § 5/04 – Final Approval § Shands at UF 1 of 7 SAL 1 TCs § 11 -County Region § 24 -bed trauma unit (2 nd Floor) § Expects ~ 1600 Trauma patients annually

= Level I TC = Level II TC

Initial Resuscitation of the Severe TBI Patient GCS 3 - 12 Emergency Diagnostic or Therapeutic Procedures as Indicated ATLS Trauma Evaluation • Endotracheal Intubation • Fluid Resuscitation • Ventilation (Pa. CO 2 35 mm Hg) • Oxygenation • Sedation • Pharmacologic Paralysis (Short Acting) Herniation? Deterioration? CT Scan YES Hyperventilation Mannitol (1 g/kg) Resolution? NO Surgical Lesion? YES To Operating Room NO Intensive Care Unit Monitor ICP Treat Intracranial Hypertension Brain Trauma Foundation (Guidelines), 1998
 • Class I Evidence: Prospective, randomized, controlled trials (PRCT) –")
Classification of Evidence (Prognosis) • Class I Evidence: Prospective, randomized, controlled trials (PRCT) – the gold standard of clinical trials. However, some may be poorly designed, lack sufficient patient numbers, or suffer from other methodological inadequacies. • Class II Evidence: Clinical studies in which the data were collected prospectively, and retrospective analyses were based on clearly reliable data. Types of studies so classified include: Observational studies, cohort studies, prevalence studies and casecontrolled studies. • Class III Evidence: Most studies based on retrospectively collected data. Evidence used in this class indicates clinical series, databases or registries, case reviews, case reports, and expert opinion with some support from animal studies.
")
Glasgow Outcome Scale (GOS)
")
Early Indicators of Outcome (Age)
")
Early Indicators of Outcome (Age)
 Greene, K. A. (1995). J Neurosurg 83: 445")
Early Indicators of Outcome (t. SAH) Greene, K. A. (1995). J Neurosurg 83: 445 -452
")
Early Indicators of Outcome (t. SAH)
")
Early Indicators of Outcome (t. SAH)
")
Early Indicators of Outcome (t. SAH)
")
Early Indicators of Outcome (Hypotension & Hypoxia)
")
Early Indicators of Outcome (CT Scan Features)
")
Early Indicators of Outcome (CT Scan Features)

Outcome Prognostication

Outcome Prognostication

Outcome Prognostication

Neuropsychological Outcome following TBI

Preinjury Functioning C O G N I T I V E L E V E L Mild TBI Brief PTA Anterograde Memory Problems I Moderate TBI N J Severe TBI PTA U R Y Retro. Grade Amnesia Coma 1 Anterograde Memory Problems PTA 7 Days 14 1 3 Months 6 12

Error Score Question Notes What is your name? -2 _____ Must give both first name and surname. When were you born? -4 _____ Must give day, month, and year. Where do you live? -4 _____ Town is sufficient. (a) City -5 _____ Must give actual town. (b) Building -5 _____ Usually in hospital or rehab center. Actual name necessary. When were you admitted to this hospital? -5 _____ Date. How did you get here? -5 _____ Mode of transport. What is the first event you can remember after the injury? -5 _____ Any plausible event is sufficient (record answer) Can you give some detail? -5 _____ Must give relevant detail. Can you describe the last event you can recall before the accident? -5 _____ Any plausible event is sufficient (record answer) What time is it now? -5 _____ -1 for each half-hour error. What day of the week is it? -3 _____ -1 for each day error. What day of the month is it? (i. e. the date) -5 _____ -1 for each day error. What is the month? -15 _____ -5 for each month error. What is the year? -30 _____ -10 for each year error. Where are you now: Total Error: Total Actual Score = (100 - total error) = 100 - _____ = 76 -100 = Normal / 66 -75 = Borderline / <66 = Impaired Developed by Harvey Levin, Ph. D. , Vincent M. O'Donnell, M. A. , & Robert G. Grossman, M. D. Can be a negative number.
 • Language (Production,")
NCSE • Orientation • Attention • Memory (Encoding, Consolidation & Retrieval) • Language (Production, Commands, Repetition, Naming) • Visuoperception/Construction • Reasoning (Similarities & Judgment)

Cognitive Rehabilitation

Cognitive Rehabilitation • Any systematic program directed at modifying cognitive function or cognitively oriented activities following acquired brain injury. • Direct Retraining Approach: Repeated engagement in therapeutic exercises and tasks that stress disrupted cognitive systems will eventually enhance or restore the dysfunctional component. • Functional Compensation Approach: Involves the use of any and all strategies, techniques, devices, and adaptive equipment available to increase functional performance and enable to patient to perform tasks that can no longer be performed in the conventional manner. Hanlon, 1994
 • “The National Academy of Neuropsychology supports")
NAN Position Statement on Cognitive Rehabilitation (2002) • “The National Academy of Neuropsychology supports empirically and rationally based cognitive rehabilitation techniques that have been designed to improve the quality of life and functional outcomes for individuals with acquired brain injuries. ” • “…there remains a need for an expansion of the graduate academic curriculum by offering training courses in neuropsychological rehabilitation to adequately prepare clinical neuropsychologists to assess for rehabilitation and to treat individuals with brain injuries. ”

Functional Compensation Strategies for Impaired Attention 1. Get enough sleep as sleep-loss impairs attention. Take a brief nap in the afternoon if necessary. 2. Determine what times during the day you are most attentive and complete mentally demanding tasks at these times. 3. Arrange your work environment to minimize auditory (e. g. , go to quiet room) and visual (e. g. , work facing a wall rather than a window, close curtains) distractions. 4. Use headphones or earplugs to reduce environmental distractions. 5. Avoid multi-tasking. Work on one project at a time and put it away before beginning another. 6. Know how long you can maintain attention and watch for indications…

Sohlberg & Mateer’s Attention Process Training - II • Principles of Treatment • Work from a theoretical model • Use therapy programs that are hierarchically organized • Use repetition (at home if necessary) • Facilitate generalization • Succeed in the community

Sohlberg & Mateer’s Clinical Model of Attention

Attention Process Training - II
")
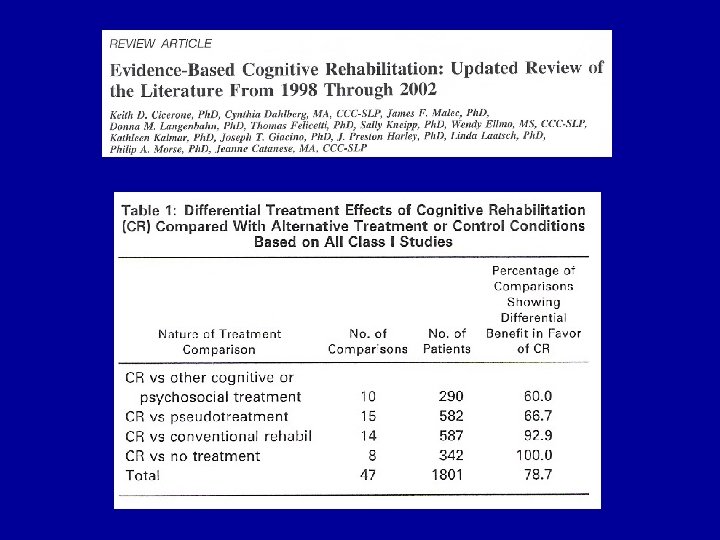
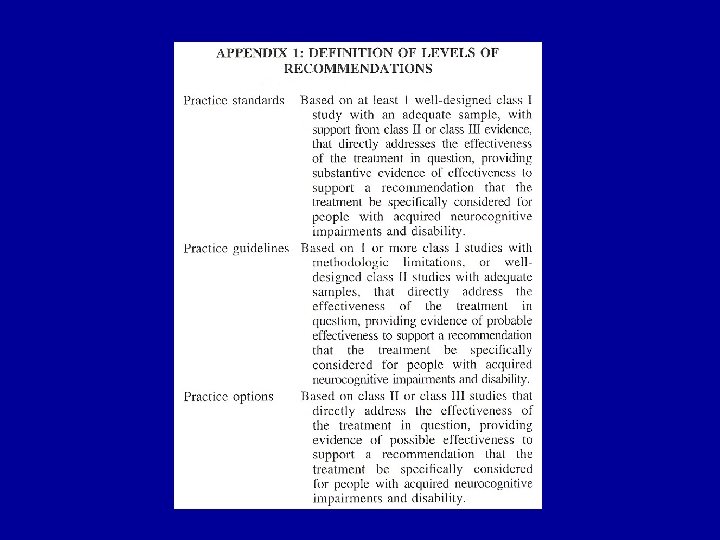
Practice Standards (CR)
")
Practice Guidelines (CR)
")
Practice Options (CR)

Questions?
- Slides: 61