TraumaInformed Advocacy Practical Advice for Working with Vulnerable

Trauma-Informed Advocacy: Practical Advice for Working with Vulnerable Populations Lisa Parsons Managing Attorney, Homeless Outreach Project Amanda Walsh and Sarah Hess Staff Attorneys, Chicago Medical-Legal Partnership for Children Legal Council for Health Justice

Agenda - LTF Legal Aid Conference, September 7 & 8 Overview of Trauma and Legal Needs (15 minutes) Practical Tools for Trauma-Sensitive Lawyering (40 minutes) Trauma-Sensitive Lawyering Role Play and Debrief (10 minutes) Secondary Trauma in the Legal Profession and Tools for Self-Care (15 minutes) ● Q & A (10 minutes) ● ● ●

Why do we need to be trauma-informed? ● Trauma impacts all basic attorney-client interactions: ○ Intake and case acceptance ○ Advice and counsel ○ Representation in informal, administrative, and judicial forums ○ Law reform and systemic advocacy ● Trauma exposure is so common, the effects so profound, it calls for a universal stance grounded in “do no harm”

How This Transforms Your Practice ● Case Acceptance - Help more clients by taking and winning cases conventional lawyers may shy away from ● Better Outcomes - Win cases conventional lawyers might lose, but can be won with strong attorney-client relationship and compelling arguments that integrate trauma research when and where appropriate ● Foster Resilience - Protects against the long-term effect of trauma and toxic stress. Every positive relationship can be restorative and help to change people’s beliefs about themselves, relationships, and the world. The challenge is to understand people’s behavior as adaptive responses to difficult challenges, not that something is wrong with them.

Overview of Trauma ACEs, Trauma, and Resilience

Definition of trauma - “The 3 Es” “Individual trauma results from an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being. ” Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14 -4884. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.

Risk factors are not predictive factors because of protective factors.

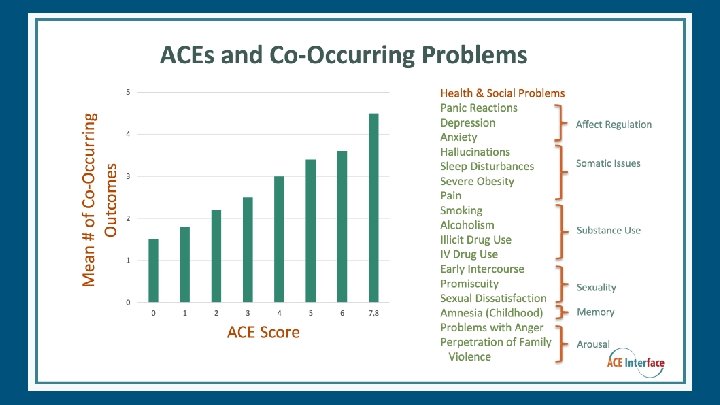
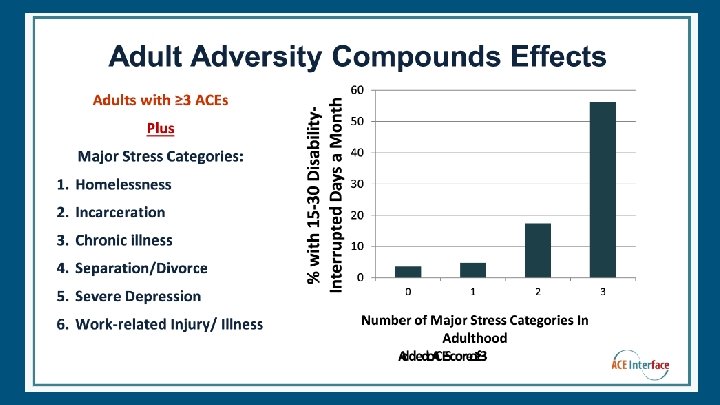
CHALLENGES 50% of the nation’s children have experienced at least one or more types of serious childhood traumas. (National Survey of Children’s Health, 2013) Almost two-thirds of surveyed adults report at least one ACE, and more than one in five reported three or more ACEs. (CDC, Adverse Childhood Experiences)
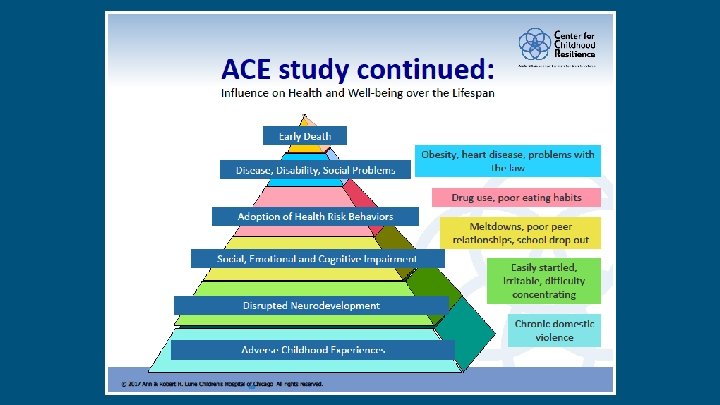
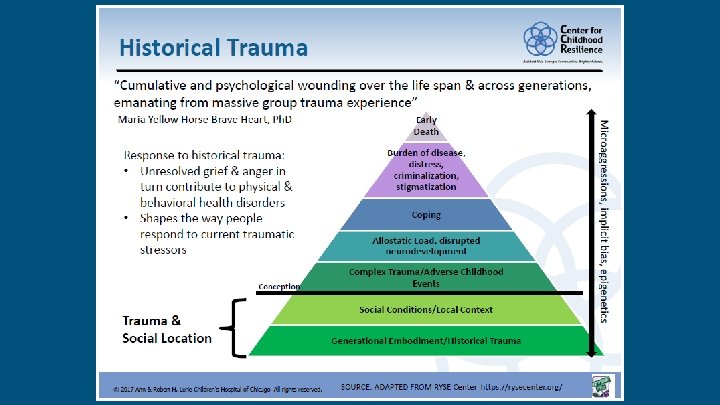

Expanded ACEs ● Experiencing homelessness and severe poverty ● Being a refugee ● Witnessing community violence ● Living in an unsafe neighborhood ● Experiencing bullying ● Having a history with foster care ● Toxic stress - ‘strong, frequent, or prolonged activation of the body’s stress response systems in the absence of the buffering protection of a supportive, adult relationship’. American Academy of Pediatrics quoting Shonkoff

Risk factors are not predictive factors because of protective factors.

Adults ● Anger/Depression ● Unexplained physical pain ● High-risk and impulsive behaviors ● Inability to de-escalate ● Substance and alcohol use/abuse ● Aggression and self-harm ● Alienation/Social withdrawal

Kids ● Child may be difficult to soothe due to chronic arousal ● Non-specific/generalized fears ● Sense of foreshortened future ● Difficulty with peer relationships ● Impulsive behavior, inability to recognize danger or consequences ● Stranger anxiety or indiscriminate attachment

Common Symptoms ● Hypervigilance ● Fight, Flight, or Freeze ● Low Self-Esteem ● Shame, blame, guilt, stigma, feeling powerless or helpless ● Avoidance ● Avoid places , people or other stimuli associated with trauma, refuse/unable to discuss ● Isolation ● Estranged/disconnected from family, social relationships ● Mistrust ● Somatic complaints ● Trauma shatters trust in others and institutions ● Pain/physical complaints

Resilience ● “Resilience is the ability … to recover and show early and effective adaptation following a potentially traumatic event. ” ● Not everyone exposed to adverse experiences is traumatized ● Positive, consistent, safe adult relationships can build resilience in children ● Even as adults, brains are capable of learning and changing National Child Traumatic Stress Network

Healing the traumatized brain ● Mindful meditation as a later-life treatment for early trauma ● Dialectical behavioral therapy (DBT) techniques ● Cognitive behavioral therapy ● Taking good care of your health ● Learning distress tolerance (or how to soothe oneself) ● Arousal-reduction tools (taming anxiety and anger) ● EEG neurofeedback

Practical Tools for Trauma-Sensitive Advocacy

SSI Homeless Outreach Project ● Serves adults experiencing homelessness with serious mental illness and co-occurring substance use ● Aim: Achieve social security and other stabilizing benefits ● Where is trauma? Central - it is the basis of the legal argument and central to providing assistance ● Open ended questions, non-judgmental, collaborative, transparent, use motivational interviewing to “mine the gap”, client choice ● Longitudinal development and avoid/reduce retraumatization in SSA administrative review process

MLP with Sinai’s Under the Rainbow ● Illinois’ first and only behavioral-health MLP partnered with a child and adolescent mental health provider ● Provides civil legal aid to children experiencing mental health issues and their families, most living in poverty and violence-stricken neighborhoods on the west and south sides of Chicago ● Aim: remove barriers to mental health treatment by addressing legal needs, allowing the child’s mental health treatment team to focus on recovery rather than coping with ongoing stressors ● Where is trauma? It can be simultaneously central to the need for legal services (i. e. trauma is impacting child’s ability to access education) and to the legal argument (i. e. the child is eligibile for SSI due to trauma symptoms)

MLP with UIC’s CHECK program ● Civil legal aid for Medicaid-eligible youth 0 -25 who have chronic illnesses like asthma, diabetes, sickle cell, and/or conditions the result of premature birth ● Aim: to mitigate the causes and consequences of trauma, toxic stress; to avoid retraumatization ● Where is trauma? If it is not central to the representation, advocates don’t attempt to uncover it; but sometimes the need for legal assistance is only because of a student’s trauma, and then we spend a lot of time educating all involved about trauma needs (i. e. , special ed)

Trauma and Legal Needs DON’T ● Do not screen for trauma unless it is essential to your case (and preferably if there is support for the client to address what comes up) ● Retraumatize DO ● Be flexible: many ways to provide trauma-sensitive services ● Adapt your systems and design new ones for these lessons ● You don’t have to be a therapist to be therapeutic
![Therapeutic Jurisprudence Recognizes that “[l]egal rules, legal procedures, and the roles of legal actors](http://slidetodoc.com/presentation_image_h2/695316ed0a1cbb6c58dcc70424537373/image-25.jpg "Therapeutic Jurisprudence Recognizes that “[l]egal rules, legal procedures, and the roles of legal actors")
Therapeutic Jurisprudence Recognizes that “[l]egal rules, legal procedures, and the roles of legal actors (such as lawyers and judges) constitute social forces that, whether intended to or not, often produce therapeutic or antitherapeutic consequences. ” What does this mean to you in your current practice?

Procedural & Substantive Justice ● Procedural Justice ○ Access to the courts and legal representation ● Substantive Justice ○ Achieving a just, fair, and reasonable solution by addressing the broader agencies impacting a legal need ● Being trauma-informed means your client’s goals may not fit into either of these categories

Establish Safety ● Consider the physical environment, position of seating, client’s view ● Be non-judgmental (Not “what’s wrong with you, ” but “what happened to you? ”) ● Continued assurance that information shared is confidential (and any exceptions) ● Preview what’s coming, lay out agenda ● Look to alternative sources to spare the client from retraumatization

Provide Choice ● Provide options at the start of each conversation ● Lay out different paths to get to client’s goal ● Never say “you have to” ● Preserve choice: pass the “pushaway” test
")
Be Trustworthy ● Set aside enough time for conversations (being trauma-informed takes more time) ● Repair disrupted relationships, acknowledge your own shortcomings out loud ● Pass the “push-away” test ● Lay out process and communication expectations, when you’re not available ● Keep promises, acknowledge when you haven’t, and don’t overpromise ● No “silverlinings”

Collaborate ● Ask open-ended questions, allow space and time for the client to share their perspective and story ● Always acknowledge the client’s goals and relate the legal issue to that orientation ● Emphasize choice, even with small things ● Frame representation as partnership

Encourage ● Affirm all successes and achievements, no matter how small or indirectly related to legal issue ● Recognize client wins even when not legal wins ● “How did you do so well in the face of so many challenges? ” ● Empower the client for future needs

Role Play

Scenario: Eviction You have an intake scheduled with Bernard, a 68 -year-old veteran, for later this afternoon. He reports his landlord has verbally threatened to kick him out on the street. The appointment was just scheduled yesterday, but since then, the receptionist tells you he has called your office eight times inquiring about different actions he should take in the meantime. However, you were in court on another matter and have been unaware of the calls piling up, causing Bernard to grow frustrated angry with your services. When you get out of court, you call him back and he demands to see you immediately. He claims if you don’t see him now, his entire life will fall apart.

Debrief 1. What was your goal for this interaction with the client? 2. What was the client’s goal of the meeting? 3. What is the client’s goal for the legal representation? 4. What were your communication techniques with this client? 5. What was the outcome of your meeting? 6. What was most challenging about this scenario? 7. What else would you want to know for the case? How would you collect that information? 8. What did you do differently when utilizing trauma-sensitive techniques that you may have not done before? 9 Are there other techniques you might have utilized to assist you with the client? 10. How did the interaction and client’s story make you feel?

Recognizing Secondary Trauma Methods for Self-Care

National Child Traumatic Stress Network

Self-care in the supervision relationship Supervisor ● Check-in with people regularly - don’t wait for someone to bring it up to you ● Model good self-care (do not send emails at midnight, send them in the morning!) Supervisees ● Talk to supervisor about your needs (caseload, suspend intake, etc. ) ● Talk about long-term career goals to avoid burnout

Organizational resistance to vicarious trauma ● How can you adjust your systems? ● Boundaries with clients, professional ethics ● Celebrate the successes, even small ones ● Don’t share traumatic stories/details unless it’s necessary ● Disconnect from email when not working (turn OFF email alerts) ● Use allotted vacation and sick days ● Organization-wide trauma trainings

Methods for self-care ● “De-traumatizing” with a similar demographic where the focus is not trauma ● Meditation ● Exercise ● Nutrition, avoid substance dependence ● Sleep ● Nurture yourself (address the stress, but don’t beat yourself up) ● Reach out for support (friends, family, professionals, IL Legal Assistance Program)

Questions and Discussion
 ● ABA Commission")
Resources Self Care: ● Illinois Lawyers Assistance Program (http: //illinoislap. org/) ● ABA Commission on Lawyer Assistance Programs, Compassion Fatigue (https: //www. americanbar. org/groups/lawyer_assistance/resources/compassion_fatigue. html ) ● CBA Mindfulness and the Law Committee (http: //www. chicagobar. org/AM/Template. cfm? Section=Comm_Pages) ACEs and Trauma: ● SAMHSA - Substance Abuse Mental Health Services Administration (http: //www. samhsa. gov/nctic/trauma-interventions) ● Near@Home Toolkit (free) for bringing Neuroscience, Epigenetics, ACEs, and Resilience to home visiting and client-centered services (https: //thrivewa. org/work/trauma-and-resilience-4/) ● Paper Tigers and Resilience - KPJR Films (http: //kpjrfilms. co/paper-tigers/) ● ACEs Too High (https: //acestoohigh. com/) ● NCTSN - National Child Traumatic Stress Network (http: //www. nctsn. org/ ● ACE Interface - Laura Porter (http: //www. aceinterface. com/index. html) ● Jack P. Shonkoff, “The Lifelong Effects of Early Childhood Adversity and Toxic Stress, ” AAP News & Journals Gateways, December 2011 (http: //pediatrics. aappublications. org/content/early/2011/12/21/peds. 2011 -2663 ). ● Centers for Disease Control, ACEs https: //www. cdc. gov/violenceprevention/acestudy/index. html

Resources Cont’d Trauma Informed Lawyering: ● Bruce J. Winick, The Jurisprudence of Therapeutic Jurisprudence , 3 Psychol. Publ Pol’y & L. 184, 185 (1997) ● Bruce J. Winick, Therapeutic Jurisprudence and Problem Solving Courts , 30 Fordham Urb. L. J. 1055, 1062 (2003 ● William G. Schma, Therapeutic Jurisprudence: Recognizing Law as One of the Healing Arts , 82 Mich. B. J. 25 (2003). ● Sarah Katz & Deeya Haldar, The Pedagogy of Trauma-Informed Lawyering, 22 NYU Clinical Law Review 359 (2016). ● American Bar Association, Trauma-Informed Advocacy Resources: http: //www. americanbar. org/groups/child_law/what_we_do/projects/child-and-adolescenthealth/polyvictimization. html ● American Bar Association and Compassion Fatigue, http: //www. americanbar. org/groups/lawyer_assistance/resources/compassion_fatigue. htm

Trauma-Informed Advocacy Lisa Parsons Managing Attorney, Homeless Outreach Project Amanda Walsh and Sarah Hess Staff Attorneys, Chicago Medical-Legal Partnership for Children Legal Council for Health Justice
- Slides: 43