Trauma to GU Tract Abbas Hassanpour MD Urologist

ﺍﻟﻠ ﺍﻟ ﺣﻤ ﺍﻟ ﺣﻴﻢ Trauma to GU Tract Abbas Hassanpour, MD, Urologist

The Case No. 1 • 23 y. o male • Driver, Seatbelted • High Speed ( 120 Km/h) Other driver dead • Car completely destroyed Patient was conscious at the scene. • On scene: BP=85/50 HR: 120 RR: 22 Sat: 98% • • At hosp. BP: 100/60 HR: 100 GCS=15 Pt is exposed. O 2 - iv – monitor

The Case No. 1 • abdo. Pain + “hip” pain Secondary Survey – Spleen normal. – Mild suprapubic tenderness. – Pelvic instability – Probable right tibial Fx – No gross blood at meatus. • “Doctor, can I put a Foley? ”

Case No. 2 § 42 yo man arriving to the ER with Car accident § GCS of 3. BP and HR stable. § Intubated at scene.

Physical Exam, No 2 • • Abdomen-soft, mild distension, tympanitic. Pelvis-stable GU-nml meatus, nml prostate position. Urinary catherter revealed gross hematuria.

FAST Ultrasound exam § Small amount of fluid in RUQ. Pelvic X-Ray § No evidence of traumatic injury.
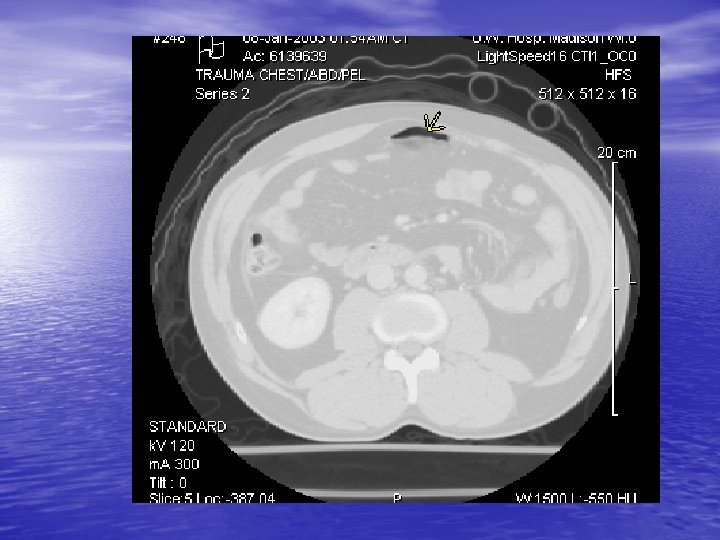

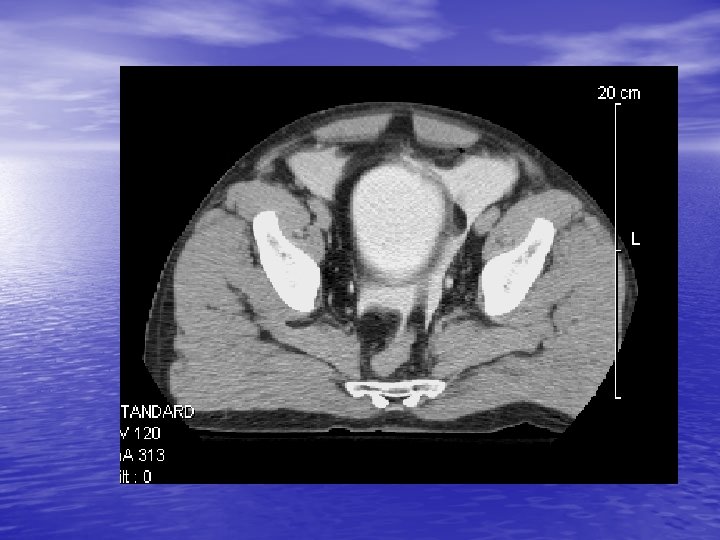

Radiology CT Cystogram § Extravasation of contrast from the bladder in both an intra and extraperitoneal distribution § Free air § Free fluid around liver

Introduction • Urology comes to the scene as a second liner. • All the rules regarding handling Emergency cases applies. • Blunt Trauma to the abdomen, pelvis and lower chest involves the GU tract in less than 10% of cases.

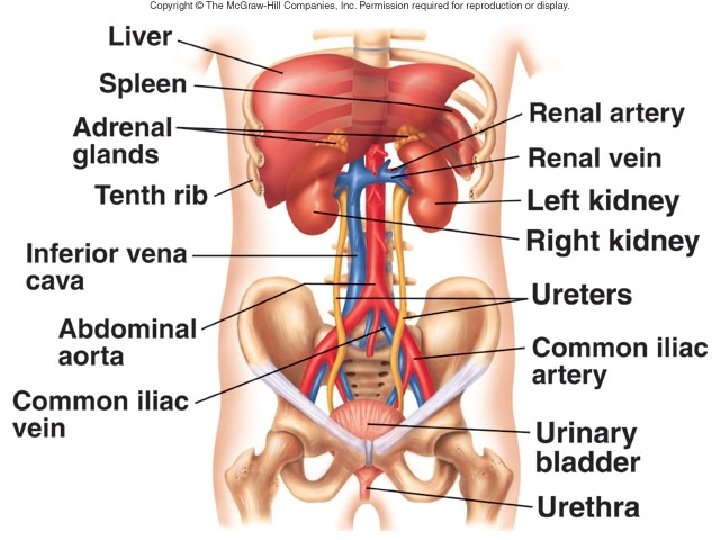
Introduction • The kidney is protected posteriorly by heavy muscles and anteriorily by the bowel. • The mechanism of trauma itself has a clinical implication. • Ureteric injury is usually iatrogenic.

Trauma to GU Tract • • • Kidneys Ureters Bladder Urethra Penis Scrotom

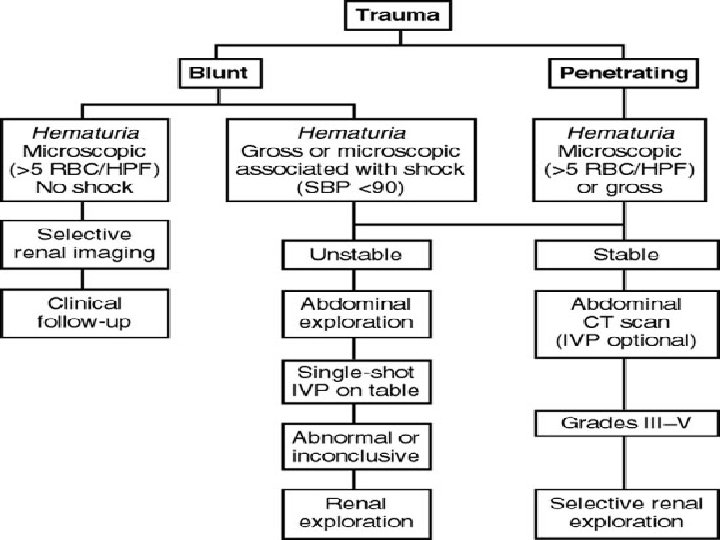
Kidney Trauma • The most common GU trauma • Motor vehicle accident, falling from height, • • • assault Deceleration: Vascular damage Penetrating: Gunshot & stab wound Hematuria> 5 RBC/hpf ( The best indicator of GU trauma) There is no relation between degree of hematuria and Injury

Injuries of the Kidneys • Suspect kidney damage if patient has a history or physical evidence of any of the following: • Abrasion, laceration, contusion in the flank • Penetrating wound in region of flank or upper abdomen • Fractures on either side of lower rib cage or of lower thoracic or upper lumbar vertebrae • A hematoma in the flank region
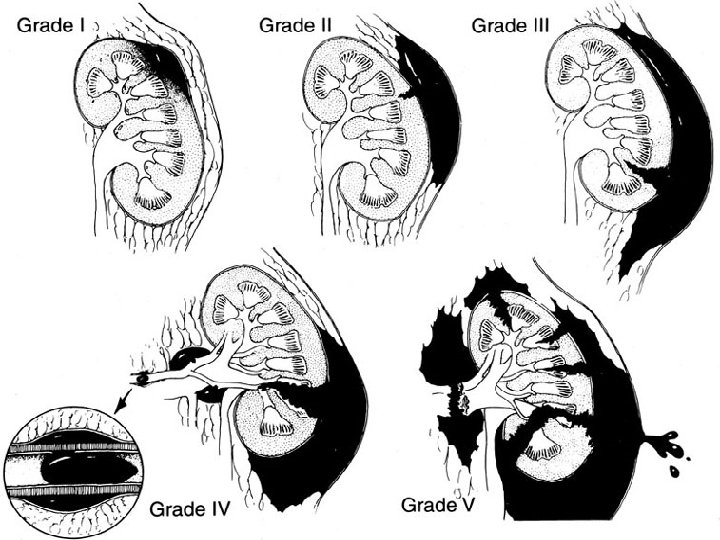

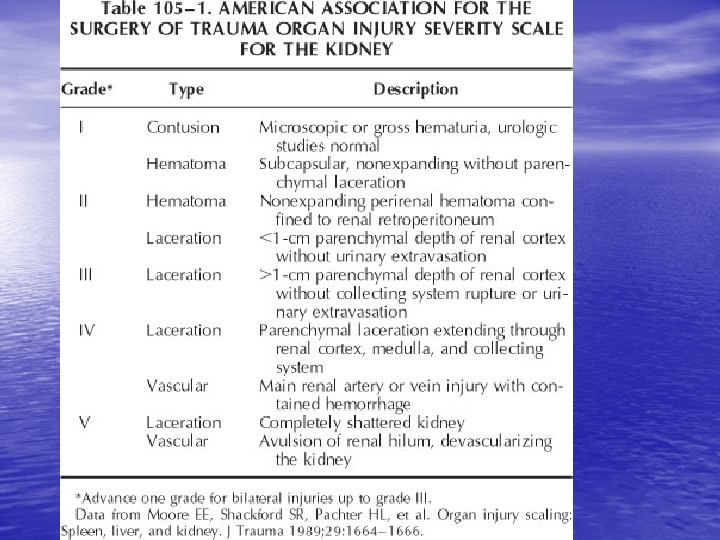
Grade I • Contusion – Hematuria – Urologic studies Nl • Hematoma – – – Subcapsular Non expanding Parenchyma Nl

Grade II • Hematoma – Perirenal – Nonexpanding • Laceration – – – < 1. 0 cm Renal cortex only No urinary extravasation

Grade III • Laceration - > 1. 0 cm No urinary extravasation – Intact collecting system

Grade IV • Laceration – – – Renal cortex Renal medulla Collecting system • Vascular – Main renal artery/vein injury with contained hemorrage.
 which devascularizes")
Grade V • Completely shattered kidney. • Avulsion of renal hilum (pedicule) which devascularizes kidney. Kennon et al. Radiographic assessment of renal trauma: our 15 -year experience. The Journal of Trauma, 154: 353 -355; August 1995.

Extravasation


CT + IV contrast Delayed images
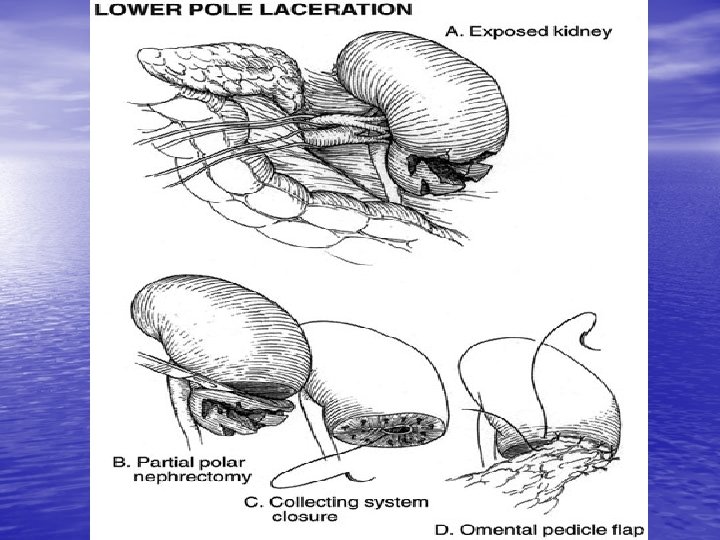
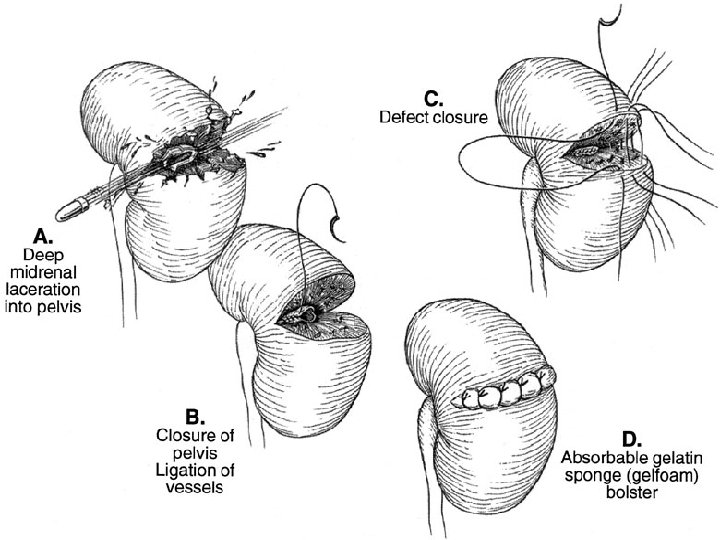
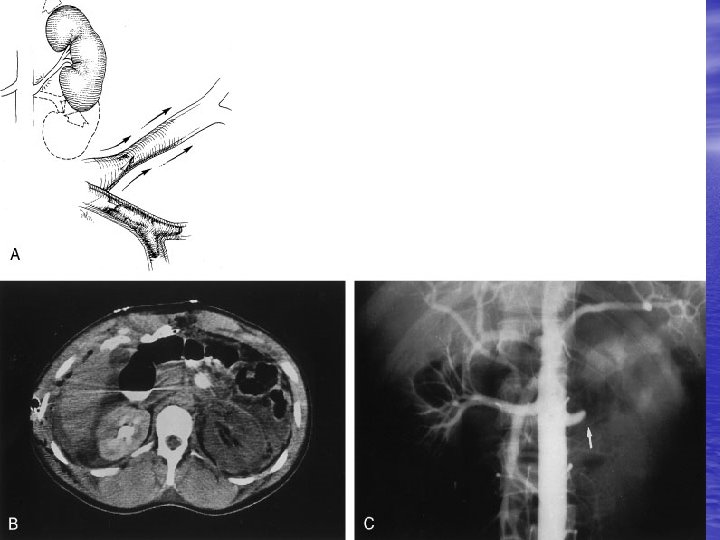

Management of Kidney Trauma • General management for trauma • Indications for exploration: 1 - Absolute: Persistant renal bleeding Expanding hematoma Pulsatile hematoma 2 - Relative: Extravasation Nonviable tissue Delayed Dx of RA injury Segmental arterial injury Incompelet staging

Diagnostic Modalities • • • Ultrasonography IVP CT Scan MRI Angiography

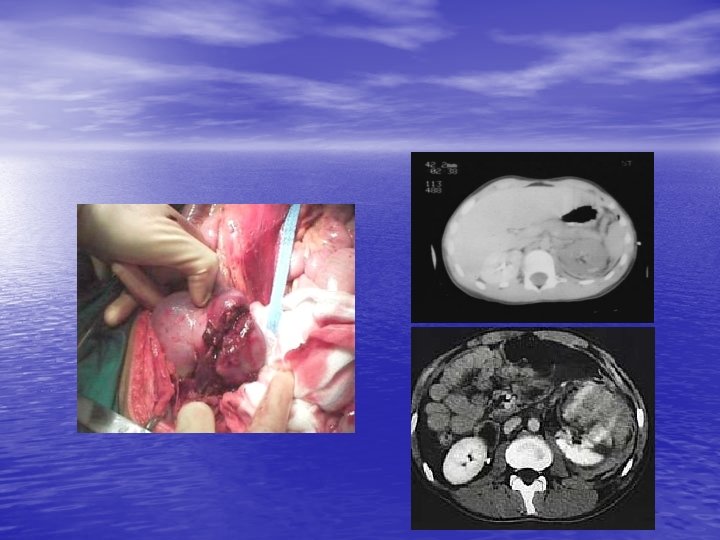
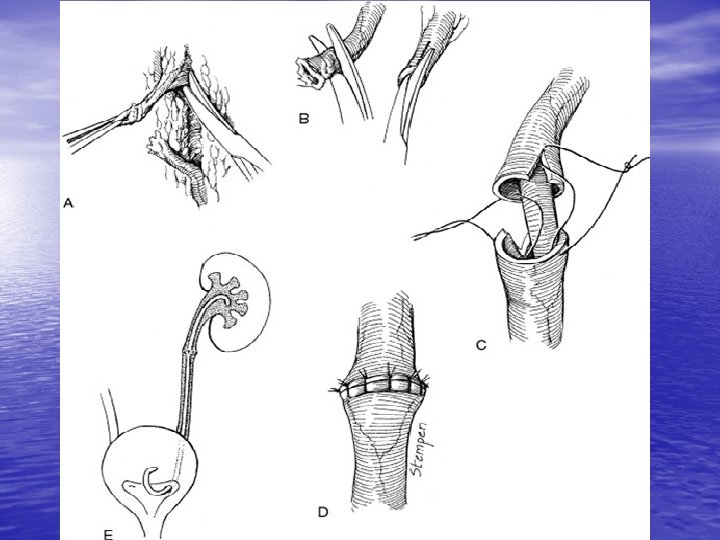
Ureteral Injury • • • Less than 4% of penetrating injuries less than 1% of blunt traumas 2 -4% of the all GU traumas Visceral injury is common UPJ avulsion? Deceleration Open surgical, Laparoscopic, And Ureteroscopic injuries Dx: U/A, APUG, RPUG, IVP, CT Scan Management: UU, TUU, RI, Psoas hitch, Boari flap, Autotransplantation

Proximal Ureteric Rupture

Bladder Injuries • Less than 2% of all abdominal injuries • 6 -10% of pelvic Fx----Bladder rupture • 10 -14% of pelvic Fx---- Urethral rupture • 83 -100% of bladder rupture---- Pelvic Fx • 10 -29% of bladder rupture---- Urethral rupture • 2% of the urethral ruptures is in female
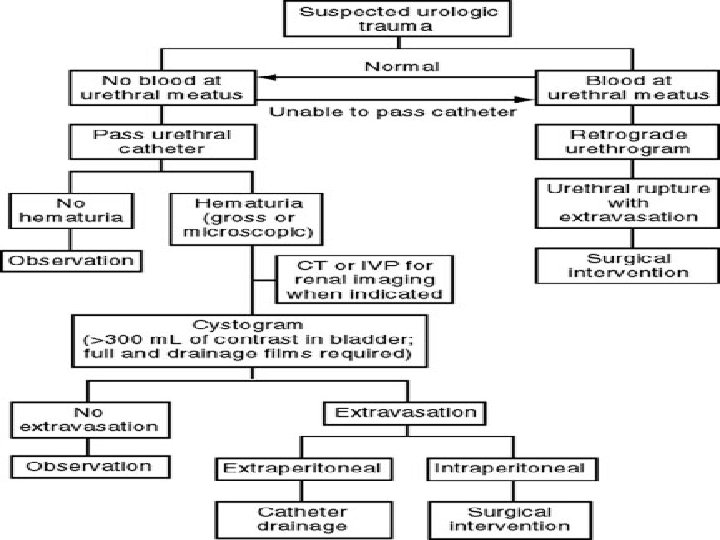

Bladder Rupture • More hematuria---- More injury • Any Degree of hematuria and lower abdominal injury • • needs evaluation Dx: Cystography (20%) & CT-Cystography(2 -4%) Management: All intraperitoneal ruptures except? Extraperitoneal when? -Bone Fragment -Open pelvic Fx -Rectal perforation -Clot obstruction -Laparotomy for other reason
")
Mechanism of Bladder Injuries (extraperitoneal)

Extraperitoneal Rupture

Distension of the Urinary Bladder

Intraperitoneal Rupture



CT-Cystogram

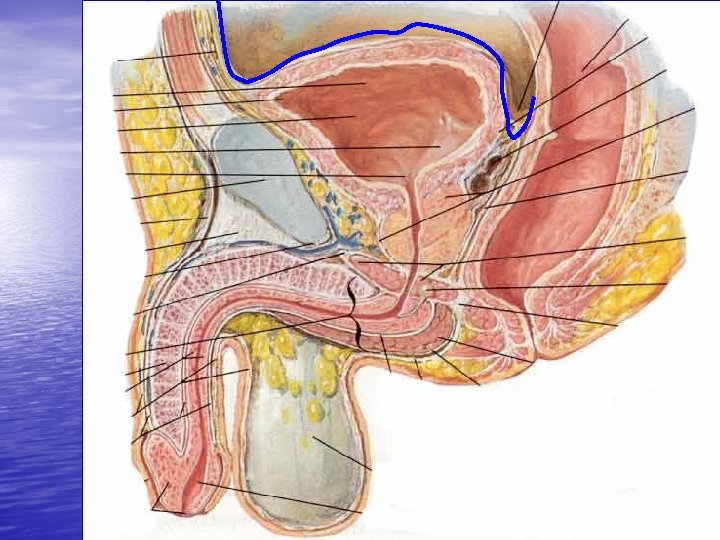
Posterior Urethral Rupture It is the Urologist who has to share the burden of this ultimate disability with the patient when the thoracic, the abdominal, and even the orthopedic aspects are probably long forgotten. Mr. Turner Warwick
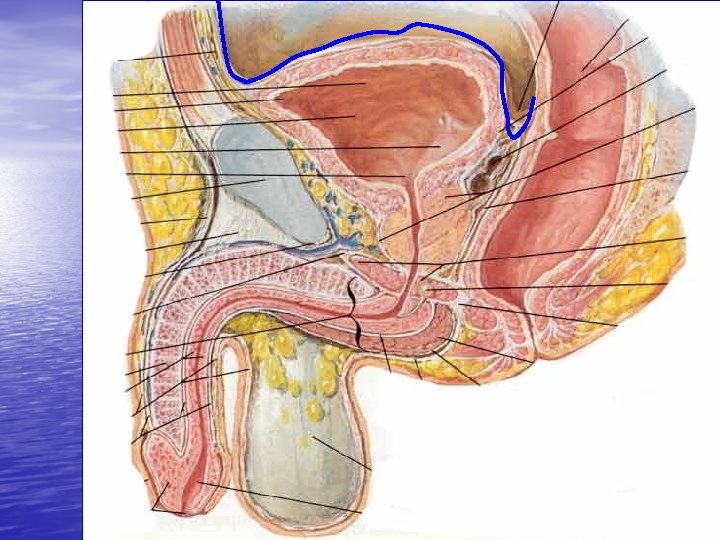

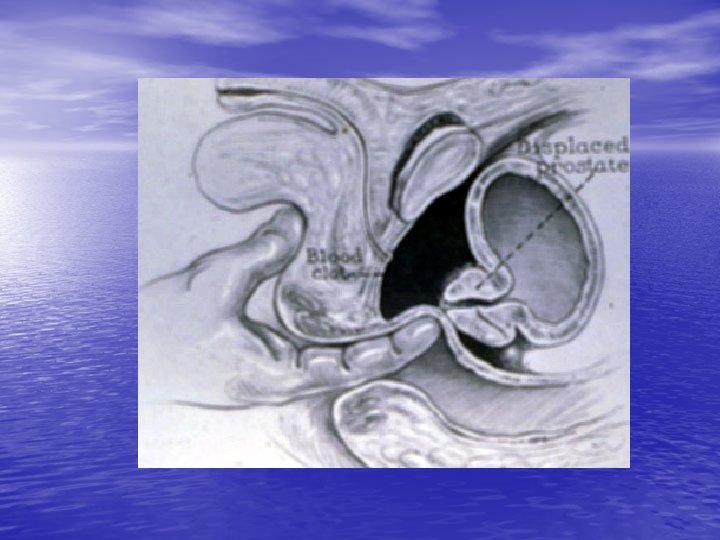
Posterior Urethral Rupture • Etiology: Pelvic Fx, especially ramus • • Shear injury Triad: Blood at the meatus Inability to urinate, probably full bladdert Dx: Immediate RUG Management: Cath. , One try by a urologist No primary open repair Endoscopic or open realignement Secondary DVIU or Urethroplasty Complications of primary repair and Urethroplasty: Impotence, Incontinence, urethral stricture, rectal injury

Saddle Injury
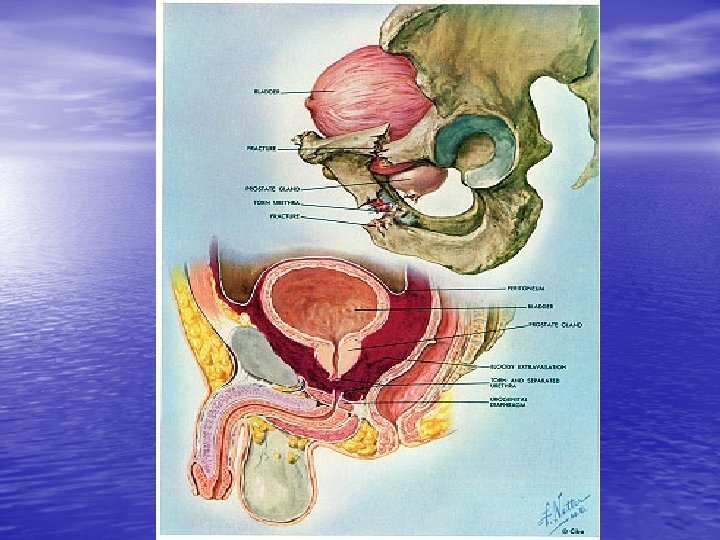

Posterior Urethral rupture From Mc. Anich JW. In Tanagho EA, Mc. Aninch JW, editors: Smith’s general urology, ed 14, Norwalk, Conn, 1995, Appleton & Lange.

RUG, A Posterior Urethral Rupture

Posterior urethral injury
")
Anterior Urethral Rupture • - 10% of LUT injuries • - Etiology: Straddle (bulbar) • • Direct penile trauma Penetrating - Dx: Large hematoma, Extravasation into the fasciae and the scrotom, Urethral bleeding, Inability to void Management: Blunt, Cath realignement or cystostomy Gunshot (low velocity), Primary surgery Gunshot (high velocity), Suprapubic and delayed reconstruction

Butterfly Hematoma


Kozin, Berlet. Handbook of Common Orthopaedic Fractures, 4 th ed. , 2000.

Partial Tear

Bulbar Urethral Stricture

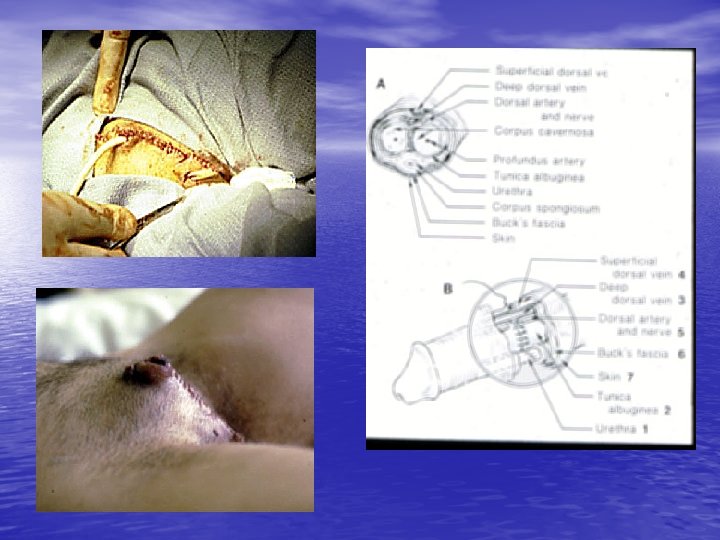
Penile Injury • - Gunshot & penetrating injuries: Urethrography for all of them Low velocity, immediate repair High v. and Massive, Stagd reconstruction • - Amputation: Self-mutilation (the most common) • How can we preserve the tissue? Replantation (16 -24 hrs)

Penile Fracture • - Cause ( CC from 2. 4 to 0. 25 -0. 5 mm) • - Hx: Popping sound, Pain, Fast detumescence • - P/E: Corporeal defect, eggplant deformity, Butter-fly • • • sign - 38% associated urethral injury (? RUG) - Paraclinic: Sono? , MRI? - Management: Observation v/s Immediate repair - Complications for observation: Deformity, Prolong penile pain, Pulsatile hematoma, Residual mass, Cavernosal diverticulum - Late complications: Veno-occlusive dysfunction, Arterial insufficiency, Curvature, Impotence, Angulation

Penile Trauma • Skin loss • Angulation • Fracture • Amputation • Foreign body entrapment

Penile Trauma

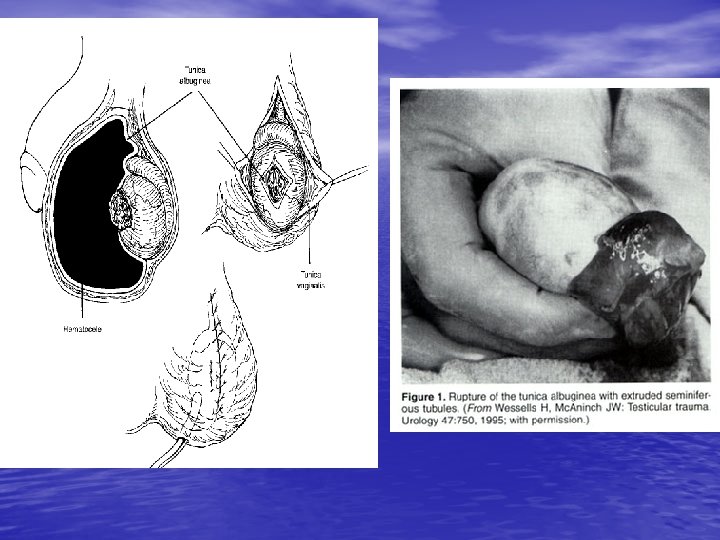
Testes Injury • • • - Each testis withstand 50 kg of blunt trauma - Assault> Sport injuries> Motor vehicle acident - The most common genital self-mutilation is testis injury - S &S: Severe pain, Hematoma, Hematocele - Imaging: 1 - ultrasono in large hematocele, gross rupture and dislocatin is not indicated 2 - Radionuclide - When should be explored? Significant hematocele, Intratesticular hematoma, Frank rupture


The End
- Slides: 72