Trauma The First 24 hours James Bonnington Objectives

Trauma – The First 24 hours James Bonnington
 can influence")
Objectives Look at factors determining trauma outcome Focus on factors we (intensivists) can influence Damage Control Resuscitation Permissive hypotension Haemostatic resuscitation NOT covering burns NOT looking in depth at head injury NOT longer term problems

Why is this Important? Trauma is number 1 killer of people aged 1 -44 yr Often previously well Good physiological reserve Dynamic situation Multidisciplinary approach
> 15 -17 Abbreviated Injury Scale (AIS) >2 in at")
Polytrauma Injury severity score (ISS)> 15 -17 Abbreviated Injury Scale (AIS) >2 in at least two body regions

What Determines Your Outcome in Trauma?

Factors We Can’t Influence “You hear that, Mr. Anderson? That's the sound of inevitability”

MHC Class II P 38 MAPK


Mechanism – detail is everything Patient A Patient B 44 yr old male Suicidal intent Driving home for Christmas Drove car at 40 mph into stationary van crash barrier

Platinum 10 Minutes?

Golden Hour? Dr Cowley “The first hour after injury will largely determine a critically injured person’s chances of survival. ” No data/references Reduced pre-hospital time good in: Severe head injury Intra-abdominal bleeds Severe thoracic injury Rural patients Newgard et al 2010: No relationship between EMS interval and in-hospital mortality

0 -62 mph 6. 8, 154 mph….

Aside - FYI Fentanyl 3 mcg/kg Ketamine 2 mg/kg Rocuronium 1 mg/kg “ 3: 2: 1”

Factors We Can Influence

Trauma Patient Mortality Head injury = leading cause of death Largely determined at time of injury Haemorrhagic shock = leading preventable cause of death in trauma

Causes of Shock in Trauma Hypovolaemic Haemorrhage Obstructive Tension pneumothorax Cardiac tamponade Distributive Neurogenic/spinal Cardiogenic Direct cardiac contusion

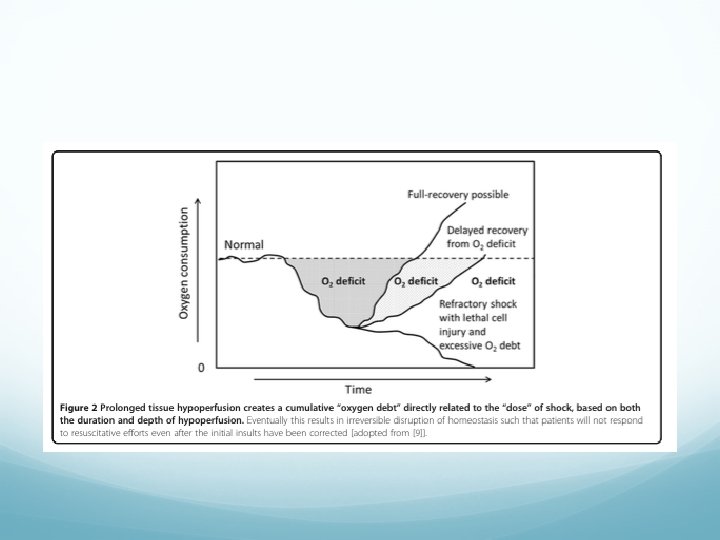
Causes of Haemorrhagic Shock 1. Direct tissue damage 1. Disruption of blood vessels with associated blood loss enough to cause tissue hypoperfusion 2. Coagulopathy 1. Intrinsic – Trauma Induced Coagulopathy (10 -40%) 2. Extrinsic factors 1. 2. 3. Hypothermia Dilution (crystalloids, blood components? ) Acidosis/tissue hypoperfusion

Trauma Induced Coagulopathy “Intrinsic dysregulation of coagulation in the setting of trauma” Needs: Tissue hypoperfusion Physical tissue damage Results in: Factors released by the tissues lead to coagulopathy Anticoagulation (thrombin-thrombomodulin / protein C) Platelet dysfunction Hyperfibrinolysis
 “limiting the amount of damage the surgeon can do to")
Damage Control Resuscitation (DCR) “limiting the amount of damage the surgeon can do to the patient” A systematic approach to major exsanguinating trauma incorporating several strategies to decrease mortality and morbidity

Principles of DCR Rapid physical control of haemorrhage Pressure/splinting/traction/tourniquet DCS Provide adequate tissue oxygenation while reducing likelihood of uncontrolled haemorrhage

Reduce likelihood of Uncontrolled Haemorrhage Recognize patients at risk Clinically obvious Trauma Associated Severe Haemorrhage (TASH) score TEG/coagulation testing Introduce practices to reduce likelihood of… Clot rupture and excessive blood loss: Permissive hypotension Coagulopathy: haemodilution/hypothermia/acidosis Haemostatic resus/massive transfusion protocol
 2. Haemostatic resuscitation (massive transfusion protocol) 3. Haemorrhage")
DCR 1. Permissive hypotension (minimal normotension) 2. Haemostatic resuscitation (massive transfusion protocol) 3. Haemorrhage control (damage control surgery)

Permissive Hypotension When: While there is, or potentially is, uncontrolled haemorrhage Not when there is controlled haemorrhage (goal becomes normotension) How: Titrate small bolus (250 ml) fluid to a hypotensive goal: 70 -90 mm. Hg Palpable radial/brachial pulses Consider fentanyl for hypertension Head injury remains an unknown

Permissive Hypotension – the evidence Multiple animal studies Reliable rebleeding point in pigs at SBP 94 mm. Hg Hypotensive pigs aggressively resucitated (80 ml/kg crystalloids) 3 x blood loss & greatly increased mortality compared with nil resucitation Review of fluid resus in animals (Mapstone) – Permissive Hypotension vs Normotension RR death 0. 37 in permissive hypotension group Anecdotal / Retrospective WWI / WWII / Vietnam War Resuscitation in absence of bleeding control can be harmful Human Studies Penetrating torso with BP<80 mm. Hg RCT (Houston): Delayed vs Immediate resus Delayed: lower mortality (30% vs 38%), less crystalloids (375 ml vs 2. 5 L, nil diff in MAP) Hypotensive trauma patients RCT : SBP target 70 mm. Hg vs 100 mm. Hg No change in mortality (ie. No increased mortality) Note no sig diff in SBP in the 2 groups Evidence suggests effect the same for Blunt & Penetrating

Haemostatic Resuscitation Identify at risk group & act before coagulopathy develops: Massive transfusion protocol Early use of blood components as the primary resuscitation fluid Use in the same ratio as they are lost through haemorrhage (exact ratio’s controversial) PRBC : FFP 1: 1 PRBC : Platelet (adult dose) 4: 1 Fibrinogen Give TRANEXAMIC ACID Prevent hypothermia / significant acidosis Monitor and give maintain i. Ca 2+

Haemostatic Resuscitation –The Evidence Massive transfusion protocol Multiple studies show increased survival Higher crystalloid use >mortatlity Higher ratio of FFP : RBC increased survival More recent wars (Afghanistan) Tranexamic Acid (TXA) CRASH 2 (2010, 20000 patients, RCT) Antifibrinolytic TXA increased survival, no increase in thrombotic episodes 1 g stat then 1 g over 8 hrs Give early, ideally less than 3 hrs Recombinant Factor VIIa Recent Cochrane review found no improvement in mortality

Damage Control Surgery Goes against traditional surgical principles that a single definitive operation is best for patient Laparotomy incision Haemorrhage control Contamination control (temporary) abdominal closure

DCS – Anaesthetic Perspective

Once on ICU “The best place for a sick person is in the ICU” Scalea 2002 “…Unless they have a hole in something major” Bonnington, any day you like

So…. Where are we?

On Arrival All critically injured patients require some degree of support Adequate ventilation Volume loading Intervene to minimize CNS injury Resolve critical acid-base disorders Resolve electrolyte disorders Restore normothermia

Respiratory Support Inadequate oxygen delivery only worsens tissue hypoperfusion Especially deleterious in CNS injury PEEP may critically impede venous return Respiratory acidosis probably a bad thing I would advocate lung protection ventilation

Homeostasis Metabolic acidosis predicts mortality and transfusion needs Best treated by restoring tissue perfusion Massive fluid shifts often produce profound electrolyte disturbances Treat aggressively Hypothermia very common Treat aggressively with passive/active full body warming

Assessment of Haemostasis No value setting any end points if you’ve still got ongoing bleeding Ongoing coagulopathy at ICU admission is associated with increased morbidity and 30 day mortality Increased early transfusion requirements predict subsequent organ dysfunction

Clotting Conundrum Majority of trauma patients present with normal or prothrombotic profiles The seriously injured are likely to present with evidence of hypocoagulability, accelerated fibrinolysis or both Later, patients tend to convert from a hypocoagulable to a hypercoagulable profile

What to Do? Standard laboratory tests? PT/APTT/Platelets/Fibrin Incomplete picture Poor predictors of bleeding Little evidence that they represent targets for resuscitation Viscoelastic? TEG/ROTEM

TEG

Cardiovascular Support Volume loading remains the mainstay Vasopressors seldom improve microvascular perfusion and may mask underlying shock Patients who seem to need vasopressors are often under-resuscitated. A lack of response to fluids may suggest irreversible shock

Fluid Choice 1. Blood 2. Blood 3. Blood 4. Clotting factors Aim for Hb 8 -10 g/dl to allow for margin of error

Need for Further Intervention Can be VERY difficult to differentiate surgical from coagulopathy-associated bleeding Continuing transfusion requirement despite good resuscitation implies: Ongoing surgical bleeding Irreversible shock Profound hepatic dysfunction

Endpoints of Resuscitation Um…. While they’re actively bleeding, “minimally acceptable levels of organ perfusion and haemostasis” After that, “the complete restoration of macro- and micro-circulatory stability and end organ homeostasis Not straightforward when the macro and micro circulation appear to be decoupled!

TRALI/TACO

Final Plea From Me….

Conclusion Poly trauma = Poly problems Prompt resuscitation vital Multidisciplinary Follows principles that may be unfamiliar to you Some uncertainty requiring further research Just ask!
- Slides: 46