TRAUMA Mary Corcoran RN BSN MICN Trauma Overview

TRAUMA Mary Corcoran RN, BSN, MICN

Trauma Overview

Epidemiology � Used to design public policy, legislation and injury prevention programs � Gathers Data such as › › › › Incidence Prevalence Age Sex Race/Ethnicity Geographic distribution Morbidity and Mortality

Epidemiology � Trauma is a disease that remains the leading cause of death for all Americans Regardless of gender, race or economic status � Leading Cause of death for ages 1 -45 yrs › (see chart pg 234)

Factors Contributing to Trauma Age � 1 -3 yrs= MVA › Due to unrestrained/ or improperly restrained � 15 -24= Accidents related to Drugs and Alcohol › Due to poor judgment and risk-taking behavior � 16 -19= MVA › Due to inexperience, lack of seatbelt usage, etoh with driving � 75+= “injuries” › Due to frailer health, pre-existing conditions, Falls (most common cause in 65+ age group) › Drivers 65+ have the highest death rate, per mile driven (except for teenagers) › More likely to sustain a C-Spine injury

Gender Males are 2. 5 times more likely to be injured than females › Related to their participation in hazardous activities, and greater risk taking � The Auto vs Ped, and MVA death rate is 2 x higher across the life span compared to women African American- Homicide, MV (65+), and auto/ped � White/Native American- Suicide � Hispanic- Pedestrian, Homicide � Race Factors Contributing to Trauma �

Factors Contributing to Death by Trauma � Fire Arms � Alcohol � Geography –Urban vs Rural � Chronology- Weekends and Holidays

Patient Assessment � Beware of Adrenaline- pt may at first appear uninjured � MOI- What is the Mechanism Of Injury, and does the injury match? � Trauma Team Criteria?

Patient Assessment � A-Airway � B-Breathing � C-Circulation � D-Disability � E-Exposure/Environment � F-Full Vitals, Family � G-Give comfort measures � H- Head to Toe/ History � I-Inspect Posterior Surfaces

Trauma Assessment http: //www. youtube. com/watch? v=Lcd. Lqfd Ik. Fc
 › › › › › Ejection")
When to notify Trauma Team � Alert (minor) › › › › › Ejection Death in same pass space Extrication <20 min Falls <20 ft Rollover w/ injury Auto Ped/Bike <5 mph Ped thrown or run over MCA <20 mph Age >59 with blunt injury to chest/abd › Children <5 yrs › 2 long bone Fx › Pregnancy 23 wks + � Activation (major) › GCS <13 › Airway Compromise � Intubated PTA › BP <90 s � Age specific in kids › Penetrating injuries to head, neck, torso, and extremities prox to elbow and knee › Traumatic Full Arrest › Paralysis › Amputation prox to wrist and ankle › Bone Injury: � Pelvic FX, open skull › Transferred receiving blood › MD discretion

Summary � Treatment of trauma patients depends on identifying all injuries and rapidly intervening to correct those that are “life threating” � Consideration of mechanisms of injury is essential to identifying patients with possible underlying injuries who require further evaluation and treatment

Head Trauma

Layers of the Brain
 � Leading Cause of Death and permanent disability- considered a")
Traumatic Brain Injury (TBI) � Leading Cause of Death and permanent disability- considered a MAJOR public health problem � 2 million people every year › 8 x more than cancer, 34 x more than HIV � 50, 000 deaths, 200, 000 hospitalizations, 1 million ER visits � $60 billion in costs in 2000 › Average lifetime cost per survivor $111, 578 › Average cost per fatality $454, 717

Head Trauma � Injuries can occur to the skull, brain, soft tissues, vascular structures, and cranial injuries � Mechanism are varied › Car crashes, sports, falls, penetrating wounds › High risk behaviors include ETOH abuse, drugs

Specific Injuries Classified by: � Mechanism › Blunt or Penetrating � Severity › Mild, Moderate or Severe � Type › Fracture, focal brain injury, diffuse brain injury

Minor Injuries � GCS is 14 -15 › Usually discharged after short observation � Normal pupils, may be asymptomatic, intact orientation/memory � Eg: Scalp Lacerations

Moderate Injury � GCS 9 -13 › High potential for increased ICP � Associated with Structural injury/damage � May require more frequent monitoring � Eg: Contusion

Severe Injury � GCS- 8 or less › Associated with Severe structural damage � High mortality rate � Usually have long term or permanent cognitive and physical disabilities › Aggressive initial management to ensure adequate oxygenation and preventing HTN is essential

Increased Intracranial Pressure � A reaction to a change in any one of the 3 fixed brain volumes › Brain, CSF, or blood If not immediately corrected will compromise cerebral blood flow � Normal ICP is 0 -15, greater than 20=intracranial hypertension �

Increased ICP � Early S/S ~ HA, N/V, ALOC, pupils sluggish � Late S/S ~ Pupils fixed/dilated, arousable only to deep stimuli (gcs <8), posturing, temperature changes › Cushings Triad (High blood pressure, bradycardia, irregular resp rate)

Increased Intracranial Pressure � Treatment › › › › Monitor ABC’s Prepare for intubation (propofol) Medicate with benzo’s Mannitol? Decrease stimulus Consider insertion of ICP monitor Decrease metabolic demands of the brain �Maintain normal temperature �Maintain normal glucose �Prevent seizures (Dilantin)

Skull Fractures � Linnear skull fracture � Non-displaced, most common type, usually benign

Skull Fractures � Depressed skull fracture › Damages underlying brain tissue and vessels by compression or laceration. May precipitate seizures

Skull Fractures � Basilar skull fracture › May occur in anterior, posterior or middle fossa. Leads to infection, hematoma, CSF leakage, SZ › S/S ~ ALOC, pupil change, CSF leak, Battle sign, Raccoon eyes, change in mentation �Change in mentation or combative behavior, is hallmark › Avoid nasal intubation or NGT

Basilar Skull Fracture

Contusion � Bruise on the surface of the brain � Occurs from movement of the brain within the skull � Coup and Contrcoup � S/S are ALOC, N/V, vision changes, weakness, and speech deficit

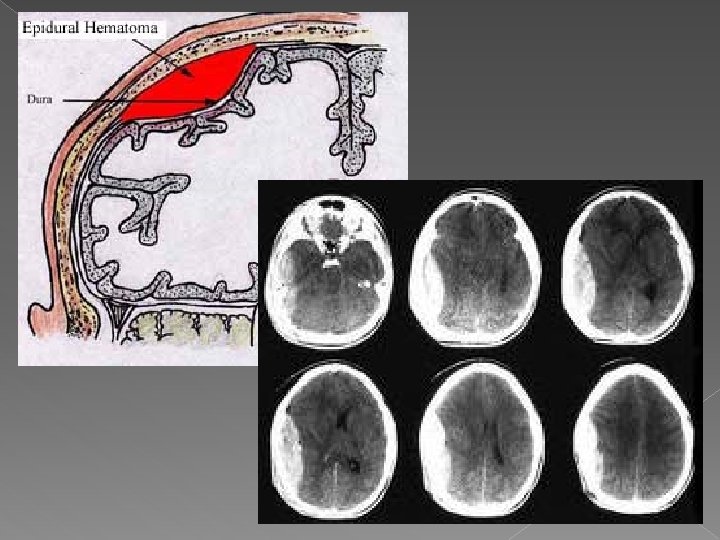
Epidural Hematoma � Collection of blood between skull and dura � Usually r/t laceration of the middle meningeal artery assosciated with a temporal or parietal skull fracture � Mortality is 50% � S/S ~ Initial period of unconsciousness, lucid interval (5 min-6 hrs), rapid unconsciousness, unilateral fixed or dilated pupils, Cushing’s Triad � TX: prepare for evacuation/OR

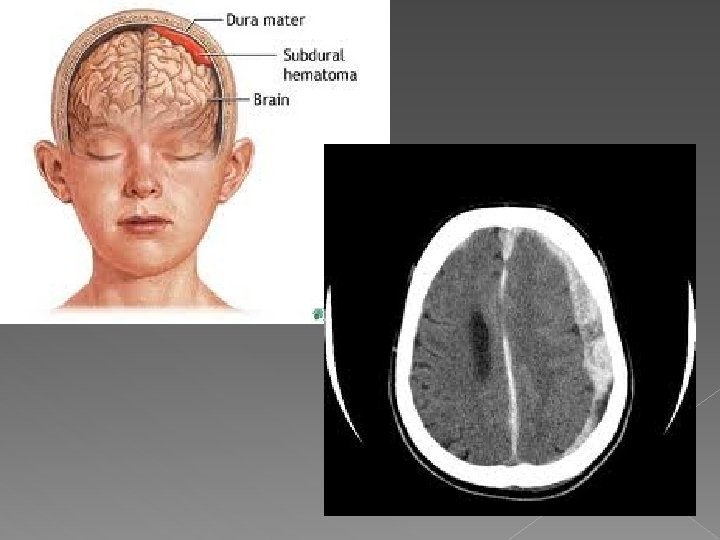
Subdural Hematoma � Collection of blood between dura mater and subarachnoid layer � Usually caused by trauma � Usually venous, therefore a slower bleed � S/S ~ HA, drowsiness, confusion, steady decline in LOC, unilateral fixed and/or dilated pupils � TX: ABC’s, prep for OR (most successful if done within 4 hrs of injury)

Subarachnoid Hemorrhage � Collection of blood between arachnoid mater and the pia mater � Caused by aneurysm rupture, AV malformation. › Aneurysm can be caused by valsalva, sexual activity, heavy lifting, or excitement � Usually 40 -60 y/o. 12% die before reaching hospital, 30% that survive have severe neurologic deficits

Subarachnoid Hemorrhage � S/S ~ › “Worst headache of my life” › Accompanied by N/V or sudden seizure › Meningeal signs (fever, nuchal rigidity)

Subarachnoid Hemorrhage

Concussion � Traumatic, reversible neurological event when there is a temporary loss of consciousness and retrograde amnesia � S/S ~ dizziness, N/V, loss of memory of event � CT to r/o bleed � Education to return if s/s
 Widespread disruption of neurologic function without any focal lesions noted")
Diffuse Axonal Injury (DAI) Widespread disruption of neurologic function without any focal lesions noted � S/S � › › � immediate LOC lasting days-months May see posturing Loss of brain stem reflexes (no gag/cough) HTN, hyperthermia, excessive sweating TX: ABC’s prepare for intubation, mannitol

Spinal Trauma

Spinal Trauma � Damage of spinal cord tissue r/t penetrating trauma, fracture, or dislocation � Most often in males 15 -35 y/o � Costs: $218 -741, 000 for first year with lifetime cost just under $3, 000 yr!

Sensory Dermatomes

Inspection ASSESSMENT � Observe for obvious signs of Spinal injury, including deformity of the vertebral column, cervical edema, and wounds � Ventilatory pattern may indicate spinal injury � Can they feel pain, or move arms and legs? � Priapism � Spinal fluid leakage

Palpation ASSESSMENT � Diaphoretic above level of injury › Indicates sympathetic injury (above T 4) � Poikilothermic- assumes temperature of surroundings › Hypothermia � Sensory status- sharp or dull � Sacral and Perineal sensations � Entire column should be palpated for pain, tenderness and step-off deformity � *use log-roll technique*

Radiologic Intervention � 3 view XR- must see C 7 -T 1 junction � Swimmers View- Open Mouth view › Used for C 1, C 2 views � CT-“Recons” › Done at same time as Chest/Abd CT � MRI- used for suspected Cord injury › Not good at bony injuries › SCIWORA (Spinal Cord Injury without Radiologic Abnormality)

Management � Methylprednisolone- reduces biochemical responses when given within 8 hrs of injury › Suspected to cause infection, PNA, decub etc. � Foley- for incont, or to monitor output � NG/OG with intubation � Warming blanket/fluids- pt can’t thermoregulation � Hypothermia? ? ?

Cervical Fixation � Halo/cervical tongs- provides c/s traction

Spinal Shock � When complete spinal cord injury occurs, all motor and sensory function below the level of injury is lost › Immediate onset � S/S: Flaccid paralysis, a-reflexia, bowel/bladder dysfunction, disruption in thermoregulation › Neurogenic shock (above T 6) s/s include sypathetic NS causes Bradycardia and Hpotension

Central cord syndrome • Results from hyperextension • Bowel and bladder fx intact

Anterior cord syndrome • Results from disruption of the anterior spinal artery • Can feel vibration, touch, and pressure • Posterior cord syndrome light touch impaired by not lost

Brown-Sequard Syndrome § Results from Hemisection of the cord § Most common from penetrating injury § Ipsilateral (same side) paresis or hemiplegia and total loss of function § Contralateral (opposite side) has decreased sensation to pain and temperature changes

Autonomic Dysreflexia � Complication of injury at or above T 6 � Life Threating injury- occurs when sympathetic stimulation leads to massive uncontrolled cardiovascular response � Common Causes: Full bowel or bladder at the time of injury

Autonomic Dysreflexia � S/S › › › › sudden severe HA HTN sweating flushing above level of injury coolness below level of injury Anxiety Blurred vision � TX-ABC’s, raise HOB, identify cause, foley

Thoracic/Abdominal Trauma

Thoracic Trauma � Some of the most life threatening injuries � Have a lot of concurrent injuries

Anatomy � Pulmonary System � Cardiovascular System

Patient Assessment � ABC’s � Auscultation of lung sounds � Inspect chest wall integrity � Ultrasound (FAST Scan) of heart and lungs

Chest Wall Injuries

Rib Fractures � Most common type of blunt chest injury � S/S – SOB, localized pain with movement, chest wall ecchymosis or contusion � Bony crepitus � Usually does not require treatment other than pain meds � Elderly may need admission

Flail Chest � Defined as fractures in 2 or more adjacent ribs in 2 or more places, or bilateral detachment of the sternum from costal cartilage. � Usually associated with Massive crush injury, high speed MVC. � Will see paradoxical movement to affected area

Flail chest You. Tube - Flail Chest

Sternal Fracture � Decreased incidence with increased use of seatbelts, shoulder restraints and air bags › Usually caused by steering wheel impact, sporting injury or falls � Increased injury potential for cardiac or pulmonary

Traumatic Asphyxia � Result of severe crush injury to the thorax › Long period of time, such as being pinned � Pathology: › Direct increase in thoracic and superior vena cava pressure from the injury › Combined with closure of the glottis � S/S › Severe cyanosis of face and neck › Subconjunctival and retinal hemorrhages › Transient LOC, SZ, or blindness

Pulmonary Injuries

Laryngeal Injury Rare and Life threating � Caused by “clothesline” type injuries � Females with long narrow necks are predisposed � s/s: � › Hoarseness, stridor, hematoma, ecchymosis, tenderness, sq emphysema, crepitus, or loss of landmarks � Tx: › NPO, HOB 30 -45 degrees, O 2, ETT, Tracheostomy

Pneumothorax � Accumulation of air in the pleural space � S/S – SOB, tachycardia, tachypnea, decreased or absent breath sounds on the injured side, chest pain � Chest tube is indicated for PTX of usually greater than 10% � Needle decompression or chest tube insertion

Open Pneumotorax � “sucking chest wound” › May see bubbles or hear a “hissing” sound � Usually result of penetrating chest wound � Apply 3 sided dressing, allowing air out but not in � If penetrating object still in place *DO NOT REMOVE*

Tension PTX � Life threating � Accumulation of air in one pleural space forces thoracic contents to the opposite side of the chest › Air can get in but not out � Immediate needle decompression is required

Hemothorax � An accumulation of blood in the pleural space � S/S – SOB, Tachypnea, chest pain, decreased breath sounds � TX – chest tube with suction. May need to consider autotransfusion or O. R.

Chest Tube insertion � You. Tube - Chest Tube Insertion. . !

Pulmonary Contusion � Potentially leathal � 75% of pts with chest injury › 40% mortality � Contusions occur when underlying lung parenchyma is damaged, causing edema and hamorrhage � Tx: › Semi-fowlers, suction, ETT (for severe hypoxia) › Usually improve in 3 -5 days

Ruptured Diaphragm Potentially life threatening injury � S/S – SOB, difficulty swallowing, abd pain, bowel sounds heard in the lower to middle chest, decreased lung sounds on injured side �

Cardiac and Great Vessel Injury

Pericardial Tamponade � Collection of blood in pericardial sac � S/S- Hypotension, tachycardia or PEA, SOB, cyanosis › Beck’s Triad ~ Hypotension, JVD, muffled heart tones

Pericardiocentsis http: //www. youtube. com/watch? v=T 1 Lb. Bxxwjak

Aortic Injury � Immediately fatal in most cases, usually die at the scene � Dx done by CXR

Aortic Injuries � Caused by penetrating or blunt trauma � S/S ~ hypotension, decreased LOC, chest pain, decreased quality of femoral pulses

Abdominal Trauma

Abdominal Trauma � Significant source of morbidity and mortality � Patients usually have a lot of pain and high risk for bleeding

Anatomy Peritoneum � Solid Organs � › Liver, spleen, gallbladder � Hollow organs › Stomach, Bowels, Bladder � Reproductive Organs › Uterus, ovaries, penis, testes � Vascular Structures › Abdominal Aorta

Assessment � History � Mechanism › Blunt, Penetrating, MVA � Auscultation › Abdominal quadrants � Palpation › Start away from area of pain

Interventions � Foley › Check for bleeding first and do rectal for prostate placement � NG/OGT › When to use NG vs OG tubes Wound Care � Medications � › Pain, ABX � Diagnostics › XR, CT, FAST, MRI, ANGIO, DPL, Labs

Splenic Injuries � Associated with fractures to 11 th and 12 th ribs � S/S ~ LUQ abd pain, left shoulder pain, abd wall rigidity. � Severe injuries require surgery
 � RUQ abd pain, abd wall")
Hepatic Injuries � Scaled 1 -5 (p 308) � RUQ abd pain, abd wall rigidity, rebound tenderness � Can have diffuse right shoulder pain

Large and small bowel injuries � Occur in less than 1% of trauma injuries � Assess for Seatbelt Sign � S/S ~ peritoneal irritation manifested by abd wall muscle rigidity, pain, hypovolemic shock, gross blood from rectum � Triple contrast CT

DPL � http: //www. youtube. com/watch? v=FXto. Tr. Lu Fj 8

Renal Injuries � Most common is blunt contusion � S/S Gross or microscopic hematuria � Flank or abd tenderness � Ecchymosis over flank area � 1 -5 Levels (pg 310) › 1=Minor, 5=Major

Renal Injuries

Orthopedic and Neurovascular Trauma
 �Skull, vertebrae, pelvis, ends of long bones ›")
Anatomy � Bones › Cancellous (spongy) �Skull, vertebrae, pelvis, ends of long bones › Cortical (dense) �Long Bones � Ligaments together � Joints & Tendons- connect bones › Nonsynovial (non-movable) › Synovial (freely movable)

Assessment � ABCs � Stabilize and control bleeding � Assess for edema, deformity, abrasion, laceration, puncture � Focused neurovascular › Pain, pulses, paralysis, parasthesia, pallor (5 p’s)
, hard splints (fiberglass), Traction splint (reduce angulation)")
Immobilization � ASAP � Soft splints (pillows), hard splints (fiberglass), Traction splint (reduce angulation) � Neurovascular checks pre and post � Elevate and Ice after splint

Orthopedic Trauma � Immediate › › treatment required for following- Open Fracture Pulseless extremity Compartment syndrome Hemorrhaging

Back Pain � Affects 60 -80% of population beginning at ages 30 -40 � May be chronic or acute � Concern is to R/O serious injury/disease � Red Flags › Trauma, age >50, fever, cancer, muscle weakness or inability to move, loss of sensation, weight loss � TX ~ Rest, Ice, NSAIDS, usually resolves

Dislocations Loss of anatomical position of 2 bone surfaces � Medical emergency due to risk for nerve and blood vessel damage � Usually requires conscious sedation � Affects shoulder, ankle, patellar, elbow �

Shoulder dislocations High incidence of recurrence � Specific mechanisms or historical facts may be suggestive of certain types of dislocations, such as lightning injuries, electrical injuries, and seizure with posterior dislocations � throwing a ball or a punch or forceful pulling of the arm with an anterior dislocation � axial loading of an extremely abducted arm with inferior dislocation. �

Fractures
")
Fracture assessment � General trauma assessment must be completed to r/o other injury (distracting) � Extremity exam (PMSC) › Pulse, Motor, Sensation, Cap refill � S/S ~ pain, deformity, edema, spasm, numbness, tingling, crepitus � TX: Immobilze, splint, pain meds, ice, elevate

Open Fractures � Considered contaminated because of possibility of foreign materials � Graded from 1 -3 � Patient will require pain meds, antibiotics, and tetanus prophylaxis � Usually are in surgery for copious irrigation within 24 hours

Amputations � Need to know history of injury � Straight or guillotine cut has best replantation potential � Contraindications include: de-gloved, mangled, crushed body part, or mishandling of body part � Consider transfer to re-implantation center

Amputations � For body part › Gently lift of contaminates (no soap, no betadine, no peroxide) › Wrap in saline soaked gauze and place in dry plastic bag and seal › Place bag on top of ice › Avoid submersion in ice water and avoid dry ice

Crush Injuries � Caused by prolonged entrapment or crushing blow � Cellular destruction and damage to vessels and nerves make crush injuries difficult to treat

Compartment Syndrome � 6 › › › P’s Pain Pallor Paresthesias Pulses Pressure Paralysis

Treatment � Steinman Pin › Provides temporary reduction of long bone fx’s, until open reeducation or internal fixation can be done

Treatment � Casts › Place splint if severe swelling expected � Clean skin well prior to placement � Education pt to look for compartment syndrome and not to scratch inside cast

Ambulation � Crutches › Proper fit is key � Cane › Minimal assistance � Walker � Wheelchair › May be used temporarily until ambulation therapy or training complete

Maxillofacial Trauma

Anatomy � Principle facial bones include frontal, nasal, maxilla, zygoma, and mandible

Assessment � ABCs › Mandibular fx may cause tongue to be displaced blocking the airway › Remove dentures or other foreign bodies � Suction secretions � Palpate facial structures � Check vision and perception � Obvious deformity or inury

Soft Tissue Trauma � Repair Lacerations within 8 -12 hrs › Unless combative- wait until more cooperative � Road Rash › Debridement done asap � Hematomas › Should be drained and dressed to prevent scaring � Avulsions › May require plastic surgery followup

Mandibular fractures � Mainly R/T MVA, altercations � S/S › › › Pain, tenderness (often referred to ear) Inability to open mouth (trismus) Malocclusion Ruptured TM or blood behind TM Numbness to lower lip

Mandible Fracture

Mandible Fracture � TX: › Assure airway clearance › Prep for OR › Possibly wiring of the jaw in the ED

Orbital Fractures � “Blowout” fracture � Usually caused by ball, baseball bat, or other blunt blow � High risk for nerve and tissue damage/entrapment � S/S › Double vision, facial anesthesia, pain, limited vertical eye movement, enopthalmos

Orbital Fracture

Orbital Fracture � TX › › › Ice to area ABC’s/CSP Instruct not to blow nose Pain meds, antibiotics Prep for OR ~ usually a few days after once swelling has gone down

Zygomatic Fracture � Mainly R/T MVA, altercations � Sometimes presented with orbital fx � S/S ~ pain, assymmetry of the face, flattened cheek, epistaxis, double vision, numbness to cheek � TX: ABC’s, ice, eventual OR

Zygomatic Fracture

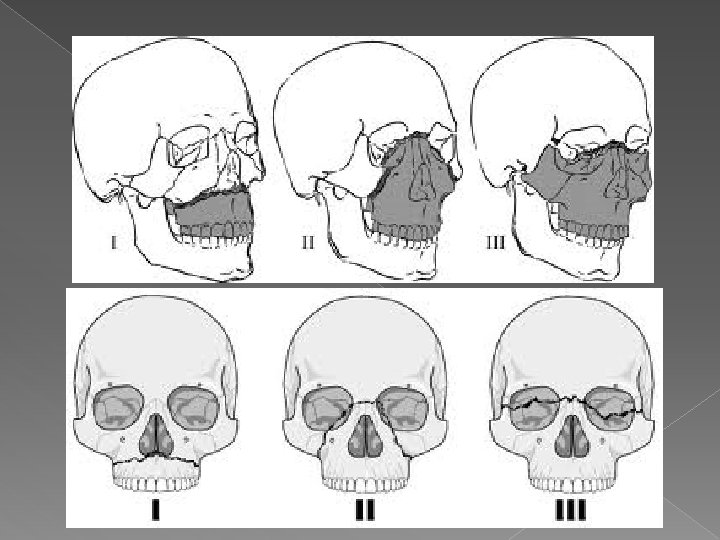
Maxillary Fractures � R/T MVA, assaults � Classified into “Le. Fort” 1, 2, or 3 › Le. Fort 1 ~ transverse detachment of entire maxilla above teeth at level of nasal floor › Le. Fort 2 ~ fracture of midface that involves a triangular segment of the mid face and nasal bones › Le. Fort 3 ~ complete separation of the cranial attachments from the facial bones

Maxillary Fracture � S/S › › › Facial edema Nasal swelling Malocclusion Nasal swelling CSF rhinorrhea (II, III)

LUNCH
- Slides: 120