TRAUMA CONNECT CLINIC KATE DALE NURSE PRACTITIONER TRAUMA












 PATIENT DISCHARGING HOME? DO THEY FIT TRAUMA CONNECT CLINIC CRITERIA? •")
 rib #")








- Slides: 28
TRAUMA CONNECT CLINIC KATE DALE NURSE PRACTITIONER TRAUMA SERVICE - GOLD COAST UNIVERSITY HOSPITAL MIDLAND TRAUMA CONFERENCE 2019, QUALITY CONNECTIONS – READY, SET, GROW
CONGRATULATIONS!
1000 patients per year 33% ISS>12
GAP IN SERVICE • No Trauma OPD • GP follow up • Multiple phone calls after DC - Appts - Pain - Requiring services • Presentations to ED • Limited and difficult follow up due to geography
WHAT WE KNOW….
WHAT DOES EVERYONE ELSE DO AND WHEN? Follow up phone calls for weekend Discharges or complicated admissions Consultant and registrar led as part of general Surgical clinic. - PTX resolution, suture removal, wound healing, reporting of radiation doses to obstetric patients 6 weeks post DC - Review of patients + USS with splenic or liver injury post blunt abdominal trauma - PTX resolution with no GP, overseas pt or need to travel - Occasional VAC Consultant led clinic - 1/52 post ICC and rib # review - Some major trauma patients Follow up phone call - Coordination - 1 week then 6 months Phone call at 1/52 Health Tap - Patients text pics of wounds or message requests for advice
Do they fit TRAUMA CONNECT CLINIC Criteria? • • TS patient requiring ongoing case management after DC TS patient with Chest Trauma requiring follow up Patients requiring ongoing analgesia management Ongoing specialised dressing care Face to face Phone Focus • Examination • Wounds • Pain • Social • Psychological Telehealth
NP led with consultant support Co-located with # clinic Dual consult with • Trauma MDT • APMS ABF funding $255 per visit 1 -2 mornings a week, 6 appointments Flexibility to coordinate with other OPD
WHO DASS – 21 Referral Flowchart Normal Range Mild - Moderate Nil Referral Required: Explain results to patient and suggest GP follow-up if they identify any new symptoms. Document in e. MR Inform patient of result and that a copy of these results will be sent to their GP; alternatively, if the patient would prefer a referral directly to a clinical psychologist, forward the same letter. GP/ Psychologist Letter Severe - Extreme Is the patient acutely suicidal or homicidal? Questions to Ask Patient: 1. How long have you felt like this? 2. What thoughts have you had today? 3. Have you had thoughts of harm to yourself/others? 4. Have you felt like this before? 5. Have you been treated for depression previously? No Inform Trauma Fellow/Consultant: Seek advice from Emergency Psych Liaison on 71709 Refer to Community Mental Health Team via 1300 642 255 Document findings and plan in patient’s e. MR. Yes – Extreme Agitation Inform Trauma Fellow/Consultant: Refer to Emergency Psych Liaison on 71709 If a patient is scheduled, contact Security to escort patient and staff to ED for triage. Document findings and plan in patient’s e. MR.
JUNE 2017 to JULY 2018 92 reviews for 52 patients Median ISS = 14 73% of patients scored ISS > 12 Average 14/month (2017/18/19) Admissions from clinic - Admitted for rib plating - Drainage of pleural effusion
Top 5 problems identified - Pain - No follow up arranged - No DC summary - Symptoms of PTSD - Issues with cognition 23 REFERALS 18 18 12 14 9 7 6 6 5 0 1 Allied Health Surgical Specialties GP Clinics (Pain/Throbosis) Psychology F
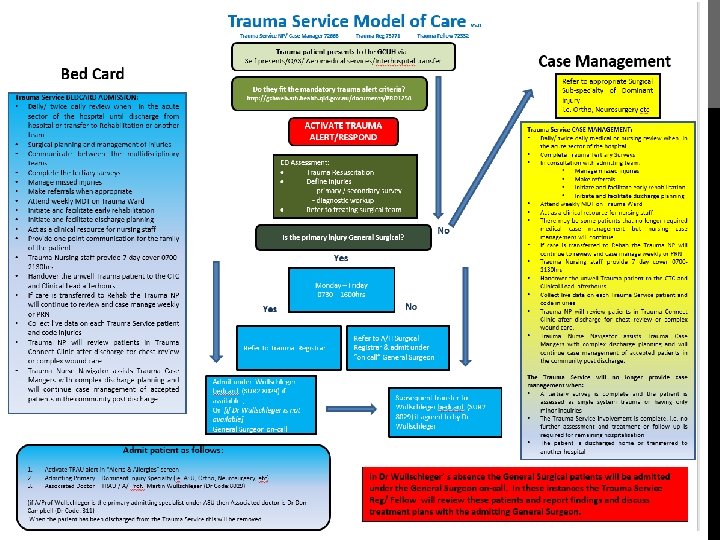
TRAUMA SERVICE (TS) PATIENT DISCHARGING HOME? DO THEY FIT TRAUMA CONNECT CLINIC CRITERIA? • TS patient with Chest Trauma requiring follow up TS patient requiring ongoing case management Patients requiring ongoing analgesia management Ongoing specialised dressing care • • Trauma Service (TS) Patient Discharging home? Do they fit TRAUMA CONNECT CLINIC Criteria? • • • TS patient with Chest Trauma requiring follow up Rib fixation patients (As required, 4 week and 12 month review with CXR) Splenic embolisation patients (As required then 6 month review with CTA) Patients requiring ongoing analgesia management Ongoing specialised dressing care
MC - 17 yo male High speed MVA Trauma Respond Injuries: R) rib # 7 -11 - Rib ORIF D 3 R) pulmonary contusion + HPTX Liver laceration grade 4 - conservative mx R renal laceration - conservative mx Splenic contusion - conservative mx DC ICU D 4 ICC removal D 9 - Persistent PTX DC home D 12 Initial follow up plan: CXR in 1 week Wound review Analgesia weaning Psychosocial support Liver USS 6/52 Urology follow up TCC = safety net
Do they fit TRAUMA CONNECT CLINIC Criteria? ✓TS patient requiring ongoing case management after DC ✓TS patient with Chest Trauma requiring follow up ✓Ongoing specialised dressing care Face to face Phone Telehealth Mode of Visit Directly Refer to • MDT • APMS • Other Specialties Face to face Phone Telehealth
Colin - 68 yo male ATV rollover, pinned under rollcage 4 -5 hours Helicopter retrieval from Tenterfield NNSW Trauma Respond Injuries: R) rib 2 -7 # with flail - ORIF D 3 R) HPTx - managed with ICC Bilateral nasal bone # Rhabdomyolysis DC ICU D 2 DC home D 7 Initial follow up plan: 2 weeks with CXR via telehealth
321 km from GCUH
2 weeks follow up Persistent bilateral pleural effusions R shoulder pain Opioid analgesia Wound review 3 month follow up Complete resolution of effusions Nil further opioid analgesia Shoulder pain improved DC to GP
Telehealth reviews: 2 Total travel time saved: 15 hrs Total distance saved: 1284 km Money saved: Approx. $500 Pain and discomfort Time off work for carer Health professionals providing care in the loop
CHALLENGES • • • Running overtime Leave cover Tech issues Extra steps Formal evaluation coming. .
BENEFITS • • Patients need follow up Knowing the patient helps! Ability to predict needs and involve MDT / APMS Improved discharge planning Ability to coordinate with other OPD Dynamic ABF benefit ($252 vs $117 for phone) Patients and families love it!
THANK YOU. Kate. Dale@health. qld. gov. au