Transplantation Immunosuppression A Casebased Approach January 20 2009
 Professor")
Transplantation Immunosuppression A Case-based Approach January 20, 2009 Paul D. Greig, MD, FRCS(C) Professor of Surgery University of Toronto 1

Saint Cosmas & Saint Damian perform the first transplant 280 CE
 “I have started research into the procedure of vascular anastomoses")
Alexis Carrel (1875 -1944) “I have started research into the procedure of vascular anastomoses in order to be able to transplant certain organs…” 1901 Sir Peter Medawar (1915 -1987) Recognized that lymphocytes were the “immunocompetent cells” that were responsible for rejection – Nobel prize, 1960

Joseph E. Murray, MD First successful organ transplant: 1954, Brigham Hospital, Boston, Mass. Kidney transplant between dizygotic twins (recipient received sub-lethal dose of total body X-radiation)

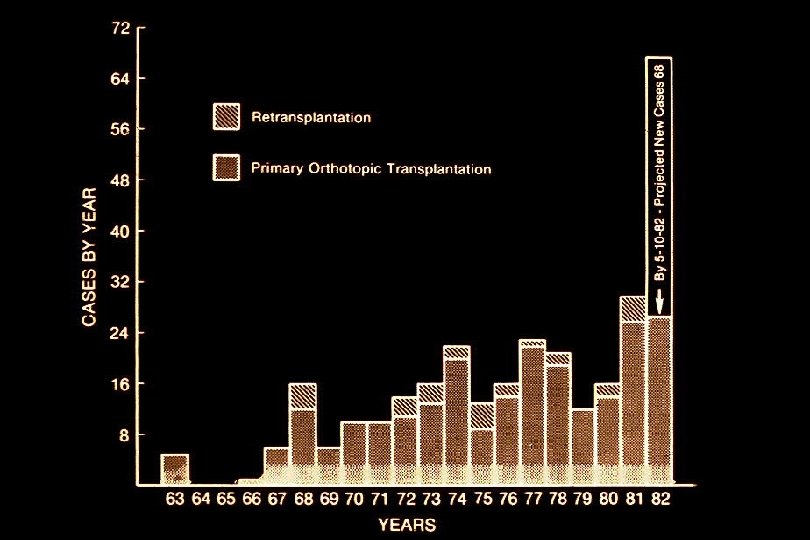
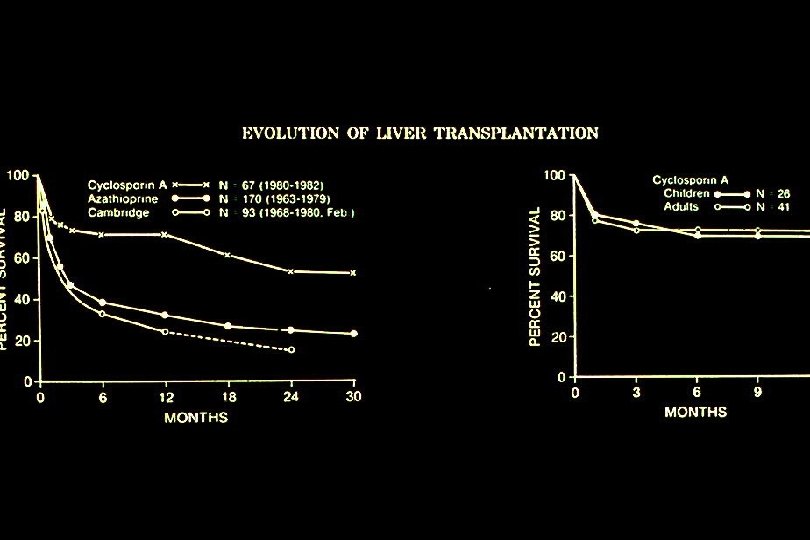
The Pioneers of Liver Transplantation Sir Roy Calne Thomas E. Starzl, MD

Liver Transplant at the University of Toronto 1985 - 2008 Year

Transplantation - Immunosuppression Case 1 • 52 y. o. male – Hepatitis C +ve cirrhosis, ascites (paracentesis q 2 -3 weeks) – Liver transplant • conventional vascular reconstruction • conventional biliary reconstruction: CBD-CBD – ? Initial postoperative immunosuppression 11

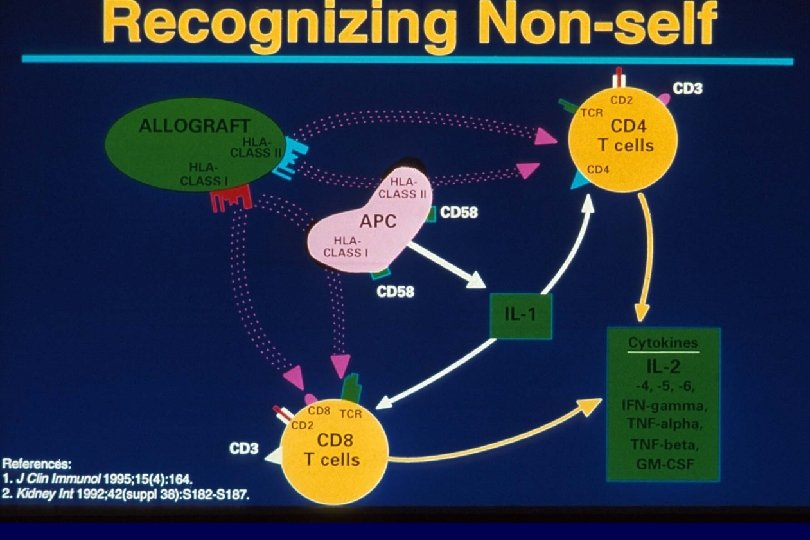
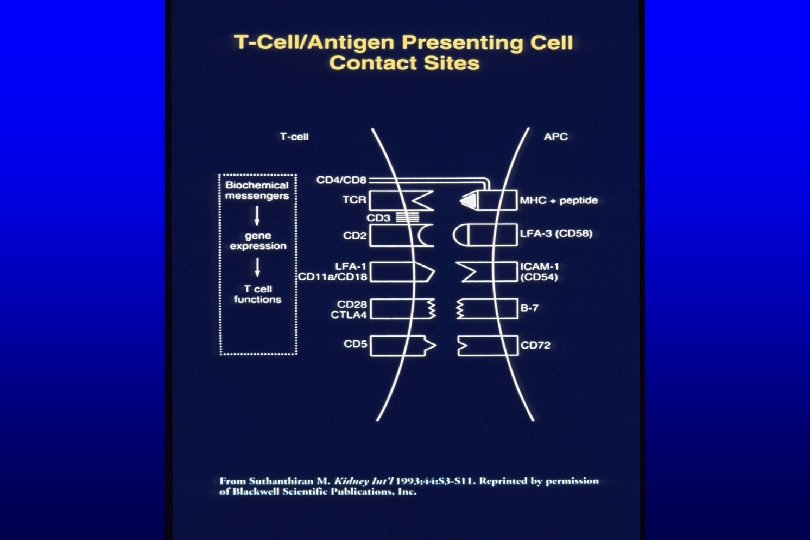
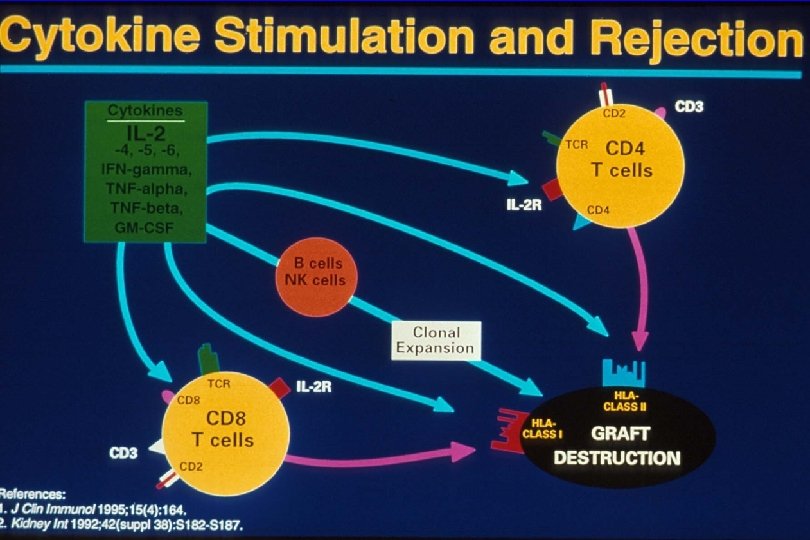
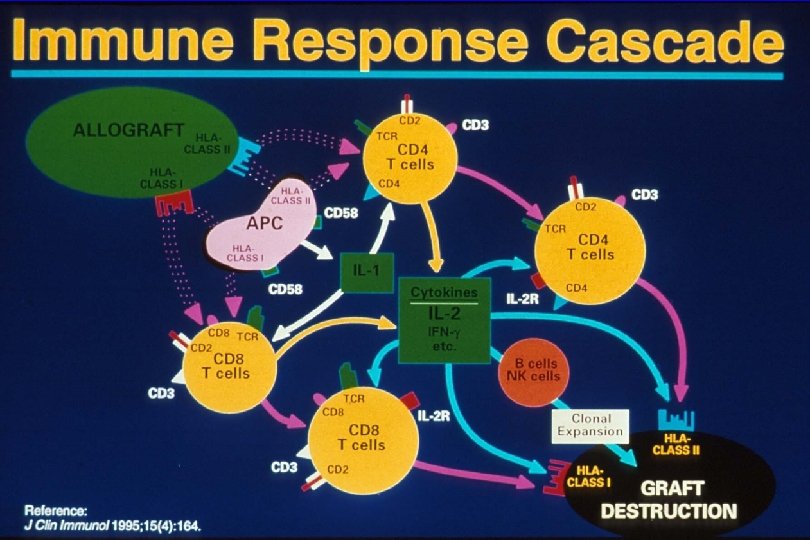
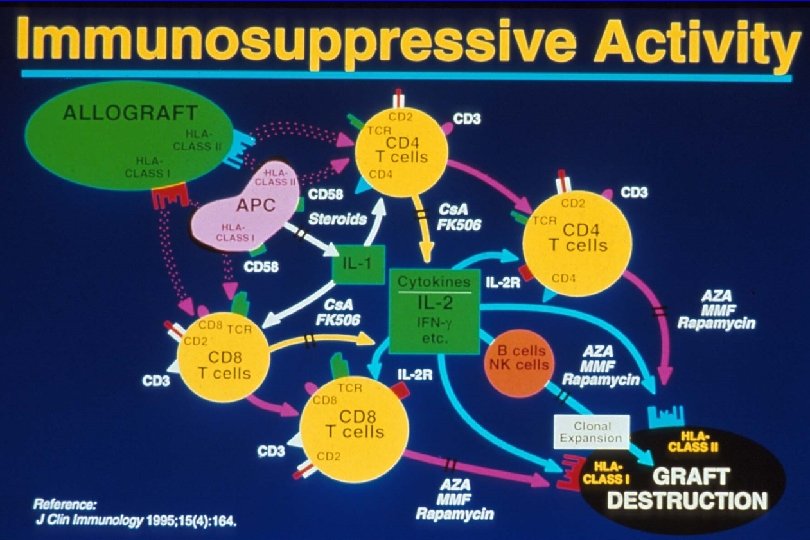
Transplantation - Immunosuppression Question 1 • why is immunosuppression necessary? • Corollary – what are the immunologic mechanisms of allograft rejection? • what are the targets of the allo-immune response? • what are the “steps” of this response? 12

Transplantation - Immunosuppression Question 2 a • what are the immunosuppression options? • Corollary – what points in the allo-immune response are the targets of current immunosuppressive drugs? – What are the current (new) immunosuppressive drugs available? – What is the mechanism of action of each of these drugs? 17

Transplantation - Immunosuppression IMMUNOSUPPRESSIVE DRUGS • Traditional Drugs – Steroids – Cyclosporine A – Azathioprine – Anti-lymphocyte antibodies: • polyclonal or monoclonal (OKT 3) • Newer Drugs – Neoral – Tacrolimus – Mycophenolate Mofetil – Sirolimus – anti- IL 2 R antibodies

Transplantation - Immunosuppression Question 2 b • what are the toxicities of these immunosuppression drugs? • Option – balance the immunosuppressive activity with toxicity with different combinations – summary of each drug: 20

Transplantation - Immunosuppression CORTICOSTEROIDS • Mechanism of action – inhibition of cytokine production by APCs • Toxicity – infection, poor wound healing, osteoporosis, aseptic necrosis, hypertension, DM, hyperlipidemia, obesity, cushinoid facies • Currently – minimize dose, alternate day therapy – early steroid withdrawal

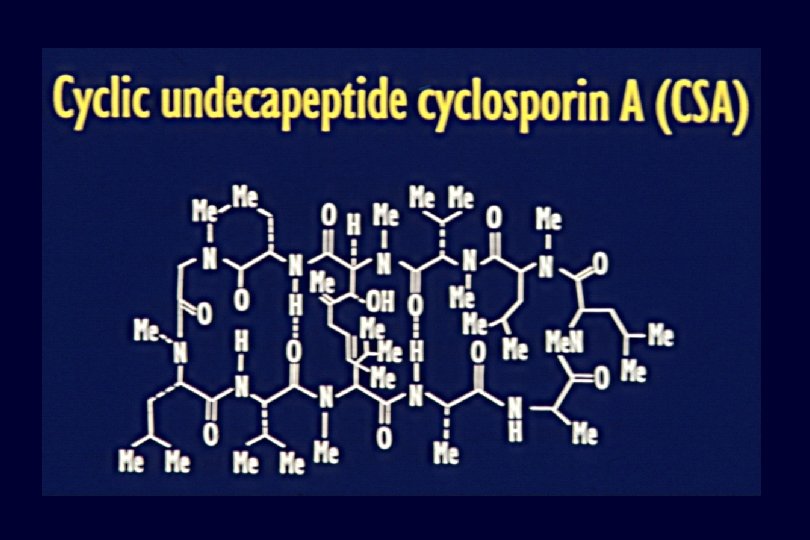
Transplantation - Immunosuppression MICROEMULSION CYCLOSPORINE A NEORAL • Mechanism of Action – inhibits calcineurin --> inhibits IL 2 production – Microemulsion Cs. A (NEORAL) • improved absorption, avoid IV dosing • Toxicity – Nephotoxicity, hypertension – Neurotoxicity (tremor, headache, direct CNS) – DM, hyperlipidemia, hirsutism, gingival hyperplasia • Currently – 10 agent – ? Optimal monitoring using C 2 (peak level) not C 0 (trough levels)

Transplantation - Immunosuppression TACROLIMUS, formerly FK 506 - PROGRAF • Advantages – lower incidence of acute rejection than Cs. A? – useful for refractory or chronic rejection – less hyperlipidemia, hirsutism, gingival hypertorphy than Cs. A • Toxicity – same as Cyclosporine A, possibly higher incidence – More DM, • Currently – primary immunotherapy, esp. those at high risk – for steroid resistant or refractory rejection

Transplantation - Immunosuppression AZATHIOPRINE • Mechanism of action – antimetabolite, inhibits PRPP amidotransterase • Toxicity – marrow: esp. neutropenia, thrombocytopenia – liver: cholestasis • Currently – routine “triple therapy” – added to reduce calcineurin inhibitor – added for rejection despite adequate calcineurin inhibitor levels

Transplantation - Immunosuppression MYCOPHENOLATE MOFETIL CELLCEPT or MYFORTIC • Advantages – no nephro- or neuro-toxicity – Mo. A more lymphocyte-specific than azathioprine – reduced acute rejection • Toxicity – marrow, GI tract • Currently – primary “triple immunotherapy” – add to Cs. A or FK monotherapy following rejection or to reduce dose for CNI toxicity

Transplantation - Immunosuppression Toxicities - in - Common • Infection – esp. viral and fungal • Malignancy – all cancers with time • importance of surveillance – Lymphoproliferative Disease (LPD) • + Epstein Bar Virus (EBV-LPD) • --> monoclonal LPD --> lymphoma

IMMUNOSUPPRESSION Individual Toxicities Obesity HBP Nepro Neuro DM Steroids +++ Lipids Marrow GIT + +++ Inf’n Calcineurin Inhibitors Cyclosporin A +++ +++ + ++ Tacrolimus +++ +++ ++ + TOR Inhibitor Sirolimus +++ ++ Antimetabolites Azathioprine +++ Mycophenolate +++ Antilymphocyte Ab ALG ++ OKT 3 ++ IL 2 R-Ab

Transplantation - Immunosuppression “Standard Combinations” • Calcineurin-inhibitor based – Corticosteroids • Solumedrol 500 mg pre-op, then taper form 200 mg/d to 20 mg/d during 1 st week – Cyclosporin A (NEORAL) • Cs. A 10 - 15 mg/kg/d divided BID, orally OR – Tacrolimus (PROGRAF) • FK 1 - 1. 5 mg/kg/d divided BID, orally – Third agent • MMF (Cellcept) 2 gm/d divided BID • Azathioprine 1 -2 mg/kg/d

Transplantation - Immunosuppression Question 2 c • Do all patients require the same degree and type of immunosuppression? • Rephrased: – what are the risk factors for acute rejection? • Who needs more immunosuppression, who needs less? – What are the risk factors for toxicity? • Any alternates without Nephro/Neuro-toxicity? 30

Transplantation - Immunosuppression Risk Factors for Acute Rejection • Increased Risk – ABO incompatibility (preformed anti- A or B antibodies) – presensitized (+ve crossmatch) • From previous blood transfusions or pregnancy – high PRA • Variable levels of preformed antibody – previous immunologic graft loss (chronic rej’n) – underlying autoimmune disease • PSC, Autoimmune CAH – younger patients • Lower risk – – Uremia Malnourished patient older patient critically ill 31

Transplantation - Immunosuppression Risk Factors for Early Toxicity • Increased Risk – renal failure • Rx: avoid Cs. A or FK by using antibody therapy * 5 - 10 days, introduce low dose CN-inhibitor with MMF or Azathioprine – preop coma, postop depressed LOC • Rx same as above – CMV -ve recipient of CMV +ve organ • Rx, lower immunosuppression or antiviral prophylaxis – EBV naïve recipient • surveillance 32

Transplantation - Immunosuppression Risk Factors for Early Toxicity • Options for patients at Increased Risk – in general: it is the nephro- or neuro-toxicity – avoid (or minimize calcuneurin (IL 2) inhibition • i. e. avoid cyclosporin or tacrolimus – use anti-lymphocyte antibodies • for 5 - 10 days • combine with MMF or Aza • introduce low dose Cs. A or Tac ~ POD 7 33

Transplantation - Immunosuppression Anti-Lymphocyte Antibodies • Polyclonal Products: RATS, ATG, ALS – cocktail of anti-bodies to antigens on activated t-cells – Toxicity: 1. Fever 2. Cross-react with platelets (thrombocytopenia) • Monoclonal Antibody: OKT 3 – murine antibody to the CD 3 receptor – Toxicity: 1. Cytokine storm 2. Anti-murine antibodies • Anti-IL 2 R Antibodies – anti-CD 25 antibody to the a-chain of IL 2 R – chimerized or humanized – toxicity: fever – ? Efficacy without CNI 34

IMMUNOSUPPRESSIVES BACKGROUND What’s The Problem? • Toxicity – major barrier to effective immunosuppression – variable spectrum of toxicities • specific to each drug – objective • juggle the toxicities of the available agents to achieve the lowest doses necessary for each patient – problem • no objective measure of the net immunosuppressive effect in any one individual

Transplantation - Immunosuppression Toxicities - in - Common • Infection – esp. viral and fungal • Malignancy – all cancers with time • importance of surveillance – Lymphoproliferative Disease (LPD) • + Epstein Bar Virus (EBV-LPD) • --> monoclonal LPD --> lymphoma

IMMUNOSUPPRESSION Individual Toxicities Obesity HBP DM +++ +++ Cyclosporin A +++ + Tacrolimus +++ ++ Steroids Nephro Neuro Lipids + +++ ++ +++ + Marrow GIT Inf’n Calcineurin Inhibitors TOR Inhibitor Sirolimus ++ ++ Antimetabolites Azathioprine +++ Mycophenolate +++ Antilymphocyte Ab ALG ++ OKT 3 ++ IL 2 R-Ab

Transplantation - Immunosuppression Standard Combinations • Corticosteroids – Solumedrol 500 mg pre-op, then taper form 200 mg/d to 20 mg/d during 1 st week • Cyclosporin A (NEORAL) • Cs. A 10 - 15 mg/kg/d divided BID, orally OR • Tacrolimus (PROGRAF) • FK 1 - 1. 5 mg/kg/d divided BID, orally • Third agent • MMF (Cellcept) 2 gm/d divided BID • Azathioprine 1 -2 mg/kg/d • Sirolimus (Rapammune)

Transplantation - Immunosuppression Case 1 • 52 y. o. male, HCV+ve, Liver transplant – Steroids: methylprednisilone or prednisone • 500, 100, 80, 60, 40, 20 -->7. 5 mg/d by POM 4 – Calcineurin (IL 2) inhibition • Tacrolimus 5 mg bid, adjust to 10 - 15 ng/ml • POD 20: – Bili: 13 --> 28, – AST 35 --> 125, • DDx? ALP 96 --> 170 ALT 40 --> 140 39

Transplantation - Immunosuppression Case 1 • DDx: – Hepatic artery thrombosis • U/S liver & Doppler, CT & arterial phase, Angiogram 40

Transplantation - Immunosuppression Case 1 • DDx: – Hepatic artery thrombosis • U/S liver & Doppler, CT & arterial phase, Angiogram – Biliary Stenosis, Leak • U/S, MRCP, ERCP 41

Transplantation - Immunosuppression Case 1 • DDx: – Hepatic artery thrombosis • U/S liver & Doppler, CT & arterial phase, Angiogram – Biliary Stenosis, Leak • U/S, ERCP – Infection • CMV --> CMV antigenemia, Liver Bx • recurrent HCV --> Biopsy 42

Transplantation - Immunosuppression Case 1 • DDx: – Hepatic artery thrombosis • U/S liver & Doppler, CT & arterial phase, Angiogram – Biliary Stenosis, Leak • U/S, ERCP – Infection • CMV --> CMV antigenemia, Liver Bx • recurrent HCV --> Biopsy – Acute Rejection • Biopsy 43

• Rejection Activity Index: • infiltrate, phlebitis, ductitis

Transplantation - Immunosuppression Risk Factors for Acute Rejection • Increased Risk – – – ABO incompatibility (preformed anti- A or B antibodies) presensitized (+ve crossmatch) - ** not with liver high PRA - ** not with liver previous immunologic graft loss (chronic rej’n) underlying autoimmune disease • PSC, Autoimmune CAH – Younger, well nourished patients • Lower risk – malnourished, older patient – critically ill 45
 HLA Matching Effect (1995 -2001) 100 63 58 52 47")
Percent Graft Survival (log) HLA Matching Effect (1995 -2001) 100 63 58 52 47 50 10 HLA mm n 0 8, 196 1 -2 7, 835 3 -4 23, 776 5 -6 13, 173 0 1 2 16% t 1/2 16. 0 13. 2 11. 1 9. 8 3 4 5 6 7 8 Years Posttransplant 9 10 Cecka, Clinical Transplants 2002 (p. 10)

Transplantation - Immunosuppression Risk Factors for Early Toxicity • Increased Risk – renal failure • Rx: avoid Cs. A or FK by using antibody therapy * 5 - 10 days, • introduce low dose CN-inhibitor with MMF or Azathioprine – preop coma, postop depressed LOC • Rx same as above – CMV -ve recipient of CMV +ve organ • Rx, lower immunosuppression plus antiviral prophylaxis – EBV naïve recipient • surveillance 47

Transplantation - Immunosuppression Risk Factors for Early Toxicity • Options for patients at Increased Risk – in general: it is the nephro- or neuro-toxicity – avoid (or minimize calcineurin (IL 2) inhibition • i. e. avoid cyclosporin or tacrolimus – use anti-lymphocyte antibodies • for 5 - 10 days • combine with MMF or Aza • introduce low dose Cs. A or Tac ~ POD 7 48

Transplantation - Immunosuppression Case 1 • 52 y. o. male, HCV+ve, Liver transplant • POD 20: – Bili: 13 --> 28, – AST 35 --> 125, ALP 96 --> 170 ALT 40 --> 140 • Bx = Acute Rejection – Grade 5 -6 / 9 • Treatment? 49

Transplantation - Immunosuppression Treatment of Acute Rejection 1 Treat Rejection – Increase CNI • If RAI < 4 – Corticosteroids • methylprednisilone 500 mg/d * 3 2 Prevent Recurrence – depends on reason for Ac. R – if Tac or Cs. A levels sub-therapeutic • increase Tac or Cs. A – if Tac or Cs. A levels adequate • add a third agent: MMF or Rapamycin 50

Transplantation - Immunosuppression Treatment of Acute Rejection • Outcome – normalization of liver biochemistry – + liver Bx confirmation • For high RAI • Steroid - Resistant Rejection – antilymphocyte anti-body therapy: – Polyclonal anti-lymphocyte antibodies • RATS, ATG, ALS – Monoclonal ALG • OKT 3 51

Transplantation - Immunosuppression Treatment of Acute Rejection • Sequelae of an episode of Ac. R – treatment increases risks of all immunotherapy related complications • viral infections – CMV, EBV • DM, psychosis, – Renal Tx • reduced graft 1/2 life • Also Lung & Heart • “Cumulative graft injury” – Liver • Increase recurrence of Hepatitis C • fewer long term sequelae • ? Induce tolerance 52

Transplantation - Immunosuppression Case 1 • 52 y. o. male, HCV+ve, Liver transplant • POD 20: – Acute Rejection , Grade 5 -6 / 9 – Treatment: corticosteroid (2 cycles) • POD 90: – fever (39 O), generally unwell – WBC = 2. 8, Liver enzymes d 25% – PE: unremarkable • DDX? 53

Transplantation - Immunosuppression DDx: 1 Bacterial Infection – CXR, Urine C&S, Blood culture – U/S or CT scan abdomen – Treat on speculation? 54
 Cytomegalovirus (CMV) • risk in")
Transplantation - Immunosuppression DDx: 2 Viral Infection a ) Cytomegalovirus (CMV) • risk in CMV +ve recipients = 25% • risk in -ve recipients of +ve organ = 50 - 100% (should receive prophylaxis) • CMV syndrome (antigenemia) • CMV disease (Bx confirmation) – liver (Bx), lung (BAL), brain (CT or MRI) – Treatment • reduce immunosuppression • Gancyclovir (IV --> PO) 55
 Epstein Barr Virus (EBV) •")
Transplantation - Immunosuppression DDx: 2 Viral Infection b ) Epstein Barr Virus (EBV) • • • presents as lymphoproliferative disease (LPD) lympadenopathy CT: head, chest, abdomen Biopsy graded: LPD --> monoconal B-cell lymphoma – Treatment • reduce (stop) immunosuppression • antiviral therapy (Gancyclovir) • chemotherapy for lymphoma 56

Transplantation - Immunosuppression DDx: 3 Fungal Infection – candida, aspergillosis, cryptococcus, mucormycosis – image and culture 57

Transplantation - Immunosuppression DDx: 4 Other Infection – TB – cat-scratch fever – Herpes simplex 58

Transplantation - Immunosuppression Chronic Rejection • Advanced graft injury • Secondary to repeated episodes of acute rejection and/or persistent low grade immunologic injury • Additive to previous injury • In donor • Preservation/ischemia/reperfusion • Liver: duct loss: “ductopenic rejection” • Target = duct or small arterioles • Lung: bronchiolar loss: “Brochiolitis obliterans” • Cumulative injury • Heart: accelerated atherosclerotic change: “graft vasculopathy” • Kidney: “chronic graft nephropathy” • Probably multifactorial • Including donor injury, preservation injury, postop injury… 59

Transplantation - Immunosuppression TOWARDS TOLERANCE • Partial Tolerance – “adaptation” allows reduction in total immunosuppression during first 3 months – = microchimerism? • Tolerizing Strategies – objective • drug-free, donor-specific hyporesponsiveness – needs: • stem or dendritic cell • induction therapy with tolerizing antibodies • continuous antigen exposure

Transplantation - Immunosuppression FUTURE • Multi-drug Regimens – variety of “protocol” therapies – increased patient-specific individualization • New Drugs – less toxicity • or non-overlapping toxicities – increased efficacy • reduced chronic rejection – more “patient-friendly” • for improved long-term compliance
- Slides: 60