Transplant Kidneys Sooner Discard Kidneys Less Francis L

















 100 80")


 Effect of Donor Age on Graft Survival Cecka, M. UNOS")
 Turndown Rate for Donor Quality 70 60 50 40 30 20")



")
 of Death Days since transplantation (Equal")
 SRTR 2001")














- Slides: 45
Transplant Kidneys Sooner Discard Kidneys Less Francis L. Delmonico, M. D. , F. A. C. S. Professor of Surgery, Harvard Medical School Director, Renal Transplantation Massachusetts General Hospital Medical Director, New England Organ Bank
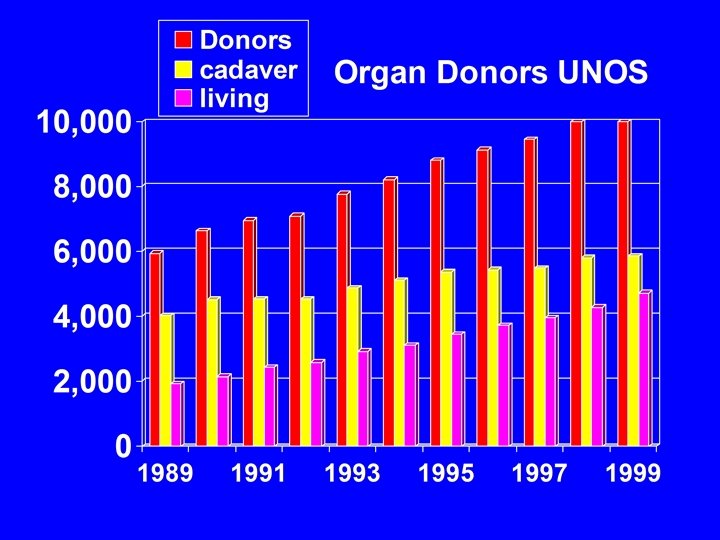
New England Organ Bank For the year 2000: 15 % of donors > 60 years of age Discarded: 45%
New England Organ Bank Year < 60 years > 60 1998 29/285 discarded 20/45 1999 25/279 discarded 21/39 2000 47/289 discarded ______ 101/853 11% 20/45 _______ 61/129 47%
Discard Rates after Recovery of Cadaveric Kidneys SRTR analyses of data supplied by OPTN contractor through November 30, 2000
Recover organs from marginal donor OPO incentives OPO disincentives legal and ethical extensive clinical testing responsibility fewer organs recovered more organs discarded meet HCFA difficult to place performance cost per organ increased standards organ acquisition fee increased disappointing to staff disappointing to families
HCFA Performance Standards Analysis of performance over 24 month period divided by two to yield average "annual" results Donors / million population Kidneys recovered / million population Kidneys transplanted / million population Extrarenal organs recovered / million population Extrarenal organs transplanted / million pop. OPO must achieve > 75% of the national mean for at least three of the five standards
Transplant organs from marginal donor Center incentives Center disincentives increase number delayed graft function of transplants increased rejection longer hospital stay assure financial worse long-term outcome stability recipient informed consent worse center-specific results attract managed managed care disapproval care providers criticism of public press
Effect of DGF Terasaki, et al N Engl J Med 1995
Percent Survival Graft Survival Rates for LRD and LURD grafts 100 90 80 70 60 50 40 30 20 10 0 Cecka, M. UNOS 1994 -1999 82 64 n Relationship 2, 129 Id Sib 1 -haplo Sib 3, 140 Unrelated 2, 071 Cadaver 34, 572 0 1 2 T 1/2 39. 2 16. 1 16. 7 10. 2 3 4 5 6 7 8 Years Post transplant 47 9 10
The New England Journal of Medicine -- August 10, 2000 -- Vol. 343, No. 6 Nondirected Donation of Kidneys from Living Donors Arthur J. Matas, M. D. , Catherine A. Garvey, R. N. , Cheryl L. Jacobs, L. I. C. S. W. , M. S. W. Jeffrey P. Kahn, Ph. D. , M. P. H. As of March 31, 2000, 98 persons had contacted us for information on nondirected donation. 18 of these persons have been evaluated, and 20 are being evaluated or are about to be evaluated; the other 60 persons have not pursued donation. Of the 18 persons who have been evaluated, 6 have been accepted as donors (the transplantation has been performed in 4 cases and scheduled in 2), the evaluation of 1 person is being reviewed, and 11 persons have not been accepted as donors because of medical or psychosocial factors. The donors for our first four nondirected transplantations have remained anonymous. We elected to admit each donor under an alias. With the use of organs from living related donors, both the donor and the recipient are usually admitted on the day of surgery. For our nondirected donations, the donors and recipients (each accompanied by family members) were admitted to different parts of the hospital to maintain anonymity. The operations in the donors and the recipients were performed simultaneously with the use of standard open techniques. The transplanted kidneys functioned immediately. Neither the donors nor the recipients had complications.
High Survival Rates of Kidney Transplants from Spousal and Living Unrelated Donors Conclusion: Spouses are an important source of living-donor kidney grafts because, despite poor HLA matching, the graft-survival rate is similar to that of parental-donor kidneys. This high rate of survival attributed to fact kidneys were uniformly healthy. Paul I. Terasaki, J. Michael Cecka, David W. Gjertson, Steven Takemoto N Engl J Med 1995; 333: 333 - 6
Brain dead LURD Cytokine storm none CIT 20 hrs INJURY < 1 hour DGF 25% < 1%
The Effect of Cold Ischemia Time on DGF Percent DGF 60 120 50 1, 282 40 9, 924 30 20 5, 032 10 18, 915 0 Cecka UNOS 1994 -98 12 24 36 48 72 Cold Ischemia Time (hrs)
1999 UNOS 3 m 1 yr 96 – 97 3 yr 5 yr 89 - 97
CIT may not affect outcome but it may affect rate of discard especially of the marginal donor kidney because well known to affect DGF centers have compelling reasons to avoid DGF
Percent DGF Cold Ischemia Time and Donor Age 70 60 50 40 30 20 10 0 Cecka UNOS 1994 -98 Donor age (yrs) 19 -30 51 -65 12 24 36 48 72 Cold Ischemia Time (hrs)
CIT by Age, Mismatch, Sharing, DGF No DGF From Dolly Tyan : Crystal City Conference March 28, 2001 DGF
Effect of CIT on Older Donor Kidneys Percent Graft Survival (Lo. G) 100 80 Donor age 19 -45 60 40 30 CIT(hrs) UNOS 1994 -99 46 -65 N T 1/2 0 -24 12, 773 11. 6 7, 056 8. 2 25 -36 4, 500 11. 5 2, 930 7. 7 445 6. 0 37 -48 609 10. 4 20 10 19 -45 0 1 2 3 4 5 6 7 8 Years Posttransplant 9 10
Percent >18 hr CIT Cold Ischemia Time and Donor Age 70 68 66 64 62 60 58 56 54 52 50 18 Cecka 30 40 50 60 Donor Age >60
Exhibit 5 From Held and Merion: Crystal City Conference March 28, 2001
Percent Graft Survival (Log) Effect of Donor Age on Graft Survival Cecka, M. UNOS 1994 -1999 100 80 60 Age 40 19 -30 31 -45 46 -55 56 -65 >65 30 20 10 55 50 42 32 24 0 1 2 3 14178 12. 7 10699 11. 1 7434 9. 0 4248 6. 7 1285 5. 4 4 5 6 7 8 Years Post transplant 9 10
Turndown Rate (%) Turndown Rate for Donor Quality 70 60 50 40 30 20 10 0 5 15 45 55 Donor Age Cecka 65 >65
Kidney Cold Ischemia by Age, Mismatch, Sharing cold ischemia time L o c 5 5 + Sharing of kidneys by age From Dolly Tyan: Crystal City Conference March 28, 2001
Current system of HLA matching as a basis of allocation priority affects preservation time to determine HLA to identify national match or necessity of payback to make contact with candidate to determine candidate acceptable to transport kidney 12 hours to transplant kidney
Why impose the duration of cold ischemia upon the cadaver kidney? To achieve 0 mm HLA matching and the required payback which has all of the ischemia and none of the HLA match
% 3 Year Survival 3 Year Kidney Graft Survival by Sharing, Age, Mismatch (99) (data NS) (65) (10) (1) (7) < 55 years of age 55 + From Dolly Tyan : Crystal City Conference March 28, 2001
Survival Benefit from Marginal Kidneys Relative Risk (RR) of Death Days since transplantation (Equal time from wait-listing) Ojo et al. J Am Soc Nephrol 2001; 12: 589.
Expected Lifetime According to Donor Characteristics Expected Lifetime (years) SRTR 2001
The Crystal City kidney work group proposal: • Allocate older donor kidneys > 60 years of age to a pre-informed group of patients based upon waiting time only. • Identify the recipients before organ procurement. • Develop a standard UNOS policy whereby a local OPO could adopt the preferential allocation of 60 year old kidneys upon UNOS notification of local OPO approval. • Allocation would occur at the level of the OPO except for the identification of a 6 antigen matched recipient nationally.
The Crystal City kidney work group goals: • Increase utilization of older donor kidneys by increasing procurement rates and decreasing discard rates; • Improve patient outcomes by decreasing cold ischemia times and delayed graft function; thus • Decrease hospitalization (length of stay) and costs.
Not all DGF is the same; data do not reveal adverse affect upon outcome at the CIT of 24 hours; benefit of CIT of 4 hours; Why impose the duration of cold ischemia upon the cadaver kidney?
Factors by Cecka that increase DGF: CIT > 24 hours PRA > 50 % Donor > 50 years of age Dialysis > 3 years
HLA Matching and Cold Ischemia in 4, 000 Kidney Pairs Percent of Kidneys 100 35 30 25 20 15 10 5 0 UNOS 1987 -1999 Zero MM (23. 5 hr) Contralateral (19. 9 hr) Other MM (21. 7 hr) 0 1 2 3 4 5 HLA Mismatches 6
HLA Matching: Number of HLA mismatches Cumulative Frequency Percent Mismatch 0 4825 13. 97 4825 1 1074 3. 11 5899 17. 08 2 3955 11. 45 9854 28. 53 3 7630 22. 09 17484 50. 62 4 8198 23. 74 25682 74. 36 5 5833 16. 89 31515 91. 24 6 3024 8. 76 34539 100 URREA
URREA Cumulative PRA 0 -9 10 -79 80+ Unknown PRA: Frequency Percent 31611 2940 505 2032 ____ 85. 23 7. 93 1. 36 5. 48 ____ 37088 100. 00
Degree of HLA Match Points are assigned based on # of mm between transplant candidate’s antigens and donor’s antigens. 7 points if there are no B or DR mm; 5 points if there is one B or DR mm; and 2 points if there is a total of 2 mismatches at the B and DR loci.
Obstacles to CIT of < 4 - 6 hours for cadaver donor recipient: Identifying recipient by HLA typing and T- cell crossmatching; Communication of organ center with tissue typing lab and transplant center; Acceptance of kidney by transplant center: finding the recipient and evaluating to be medically suitable; scheduling and performing the transplant.
Hypothesis: If the unrelated living donor kidney without the benefit of HLA matching can achieve such a successful outcome usually with < 1 hour CIT and <1% DGF the cadaver donor kidney with < 4 hours CIT, reduced rate of DGF, and improved regimen of immunosuppression, would achieve a much improved outcome for a majority of recipients.
UNOS Region 1 kidney transplants 12. 1. 97 - 7. 31. 00 1063 transplants Kidneys allocated by Region 1 plan by special criteria 0 mismatch Reg 1 not used in Region discarded sent out of Region 54. 1% 5. 4% 3. 1% 19. 7% 14. 7% 5. 2% exported mandatory share 17. 7% 100%
Percent Survival Graft Survival Rates for LRD and LURD grafts 100 90 80 70 60 50 40 30 20 10 0 Cecka, M. UNOS 1994 -1999 82 64 n Relationship 2, 129 Id Sib 1 -haplo Sib 3, 140 Unrelated 2, 071 Cadaver 34, 572 0 1 2 T 1/2 39. 2 16. 1 16. 7 10. 2 3 4 5 6 7 8 Years Post transplant 47 9 10
Kusaka, M. ; Pratschke, J. ; Wilhelm, M. ; …. Hancock, W. ; Tilney, N. Activation of inflammatory mediators in rat renal isografts by donor brain death. Transplantation 69: 405 -10, 2000 Brain death triggers nonspecific inflammatory events. In this study, changes in kidney isografts from BD donors compared to normal anesthetized, ventilated controls. numbers of infiltrating polymorphonuclear leukocytes peaked at 24 hr in parallel with intragraft induction of P - and E-selectin, complement, and proinflammatory chemokines and cytokines. At 5 days, isografts from BD donors infiltrated by host leukocyte populations assoc with up- regulation of products. In contrast, those from control donors remained relatively normal.
HLA Matching and Graft Survival in Recipients of Paired Cadaver Kidneys with Longer or Shorter CIT Percent 30 Shorter Longer 25 20 15 10 5 0 0 1 2 3 4 5 6 HLA Mismatches Percent Graft Survival 100 35 90 80 70 60 50 78 75 CIT n T 1/2 Shorter 3, 109 10. 1 Longer 3, 109 9. 5 40 0 1 2 3 Years Posttransplant Cecka, Clinical Transplants 1999 (p. 13)