Translation of research into policy and practice examples






















 attending assessment Number")
: N (%) Maaori Non-Maaori Age group (N=1241*):")
 4 -week CO-validated: N (%)")








 • PM was charged")









- Slides: 44
Translation of research into policy and practice examples from smoking cessation Hayden Mc. Robbie MB Ch. B Ph. D Profession in Public Health Interventions, Barts and The London School of Medicine and Dentistry (UK) Visiting Professorial Fellow, NDARC, University of New South Wales (AUS) Clinical Director, The Dragon Institute for Innovation (NZ) Medical Specialist, Counties Manukau District Health Board (NZ)
Disclosures • In the past 5 years have received honoraria for speaking at smoking cessation meetings that have been organized by J&J and Pfizer • I have no links with any tobacco or e-cigarette manufacturers • I believe that vaping, when used to help people stop smoking, can make an overall positive contribution to public health
Evidence into practice • We often have enough evidence, but… – Policies sometimes take a different approach – We don’t implement what we know, either at all, or effectively • Things change - we need to be able to adapt over time
Examples from smoking cessation 1. Brief smoking cessation interventions 2. Helping pregnant women stop smoking 3. The rise of vaping (electronic cigarettes)
Brief Smoking Cessation Interventions
Increasing ex-smokers ‘The first law of smoking cessation’ Professor Robert West, UCL E=Nx. S number of exsmokers created in a given time period number of smokers who try to stop probability of success in those who try
Importance of brief advice • Brief advice from a healthcare professional prompts people to quit • RR = 1. 66 (95% CI: 1. 42 -1. 94) Stead et al 2013. Physician advice for smoking cessation. Cochrane Database of Systematic Reviews. CD: 000165 • Increases long-term abstinence rates by 1 -3 percentage points (above unassisted quit rates, which are around 2 -3%)
New Zealand Government Health Target Settings: • Primary care • Secondary care • Pregnant women Rationale: • to encourage more people to make more quit attempts, supported with evidence-based treatments, more often. Guided by ABC - Ask about their smoking status - If they smoke, give them Brief advice to quit - Cessation treatment, should be offered to all smokers
Measurement Primary Care Secondary Care GP Practice Management System Maternity Coding of clinical records booking forms (ICD-10) % = Number of smokers given brief advice and/or cessation support Number of current smokers
Primary Care Results 2012/13 2013/14 2014/15
Implementation 1. Systems and tools • Tools to promote implementation of FCTC Article 14 2. 3. 4. 5. on tobacco cessation 1 • New guidelines – based on Effectiveness and Affordability Review 2 Training Audit and feedback Leadership from clinicians and senior management Incentives 1. Raw, Mc. Robbie, West & Mc. Neill. Tools to promote implementation of FCTC Article 14 on tobacco cessation. Version 1 2014 2. West R, Raw M, Mc. Neill A, Stead L, Aveyard P, Britton J, Stapleton J, Mc. Robbie H, Pokhrel S, Borland R. Healthcare interventions to promote and assist tobacco cessation: a review of efficacy, effectiveness and affordability for use in national guideline development.
Use of plain language ‘Helping People to Stop Smoking’ instead of ‘Smoking Cessation’ Use of evidence summarized by international experts Used evidence and recommendations from a review of the effectiveness and affordability of stopsmoking interventions, which was specifically to help countries write national guidelines Revised ABC pathway The latest evidence on providing brief advice suggests that more people will make a quit attempt if the brief advice is followed by an offer of cessation support A step-by-step approach • Provides an example of how to make an offer of help to quit • What to do when a person accepts the offer, appears unsure, or declines • There is no expectation of busy frontline health care workers to provide cessation support – they can simply refer on to Stop-smoking services 6 Pages instead of 56 pages Provides a summary of interventons – more detailed evidence held online http: //www. health. govt. nz/publication/new-zealand-guidelines-helping-people-stop-smoking
Evaluation of this approach • N=412 hospitalised smokers were interviewed about their experience of ABC • 66% reported making a quit attempt. • At four weeks 33% of those who had made a quit attempt had successfully quit (Russell Standard). https: //www. hiirc. org. nz/page/34520/abc-in-secondary-care-outcomes-study/? section=10541&content. Type=251&tab=4203&
What next? Possible options • A focus on a cessation outcome • Greater focus on one of the systems level measures: proportion of children at 6 weeks old living in a smokefree home (i. e. no one in the home smokes)
Adopting a life-course approach Chronic noncommunicable disease risk Early Intervention Later interventions are still important, but have less impact Ideal course Life course Pre-conception - Pregnancy - 1 st 1000 days- Childhood – Adolescence - Adulthood
Helping Pregnant Women Stop Smoking
14% of pregnant women In New Zealand… report smoking at time of registration with an LMC 35% 37% women < 20 years-old Māori women 78% of women smoking at registration are still smoking 2 -weeks after giving birth 80. 5% Ministry of Health. (2017). Report on maternity, 2015. Wellington: Ministry of Health women of Māori
Supporting pregnant women to quit Financial incentives • ABC for smoking cessation • Positive, non-judgmental, mana-enhancing conversations • Show an understanding of the woman’s lived reality • Strongly encourage women to enroll in a stop smoking service – this will provide the best chance of quitting Nicotine Replacement Therapy Face-to-face support
Financial incentives • May be more effective in people from lower socioeconomic groups • High vs. low deprivation • OR = 2. 17 (95% CI: 1. 22 - 3. 85) Incentive schemes may help reduce health inequalities Mantzari et al, Preventive Medicine 75 (2015) 75 -85
Financial incentives for helping pregnant women stop smoking Source: Cochrane Database of Systematic Reviews 2015 http: //onlinelibrary. wiley. com/doi/10. 1002/14651858. CD 004307. pub 5/full#CD 004307 -fig-0003
A recent trial A Randomized Controlled Trial of Financial Incentives to Low Income Pregnant Women to Engage in Smoking Cessation Treatment: Effects on Post-Birth Abstinence Moderate incentive payments for smoking treatment engagement (a mean of ≈$214 paid) increased lowincome pregnant smokers' engagement and success in smoking cessation treatment. – 7 -day biochemically confirmed abstinence rate at 6 -month postpartum Intervention vs. control = 14. 7% vs. 9. 2% p <. 01. Baker et al J Consult Clin Psychol. 2018 Feb 1
Audit • Data from all cases referred between January 2012 and June 2017 were extracted from the service database – Cases completed before August 2013 were without financial incentives and did not have self-reported smoking status biochemical validated Analyses • Pre-post comparisons (chi-squared test) on the following variables: numbers of referrals, attendance, setting a TQD, demographics, tobacco dependence, and 12 -week quit rates (self-reported preincentives vs. CO-validated with-incentives). • Logistic regression was used to adjust for any variables that differed between the periods. Mc. Robbie & Lee. A ‘REAL-WORLD’ EVALUATION OF FINANCIAL INCENTIVES TO HELP PREGNANT WOMEN STOP SMOKING. SRNT Annual Meeting 2018.
Results: referrals and attendance Characteristic Total Number of referrals Number (%) attending assessment Number (%) setting a quit date No Yes 1384 2191 11652 924 (67%) 132 (60%) 792 (68%) p=0. 026 643 (46%) 73 (33%) 570 (49%) p<0. 001 1 over 19 months 2 over 47 months Offered Financial Incentive Statistical Sig
Results: client characteristics Characteristic Ethnic group (N=1337*): N (%) Maaori Non-Maaori Age group (N=1241*): N(%) Under age 30 years 30 + years Time to first cigarette of the day (N=786*): N(%) Within 30 minutes After 30 minutes * due to missing data Total Offered Financial Incentive 794 (58%) No 105 (48%) 114(52%) Yes 689 (59%) 482(41%) 888 (64%) 512(36%) 455 (58%) 331 (42%) 76 (35%) 143 (65%) 20 (57%) 15 (43%) 812 (69%) 359 (31%) 435 (58%) 316 (42%) Statistical Sig p<0. 01 P<0. 001 p=0. 92
Results: quit rates Definition 4 -week self-reported: N (%) 4 -week CO-validated: N (%) 12 -week self-reported: N (%) 12 -week CO-validated: N (%) *adjusted for ethnicity and age Total Offered Financial Incentive No Yes 431 (67%) 308 (48%) 45 (62%) 8 (11%) - 386 (68%) 379 (67%) 300 (53%) 262 (46%) • Quit rates at 12 -weeks were 11% vs. 46% (p<0. 001) • a. OR*=4. 99, 95% CI: 2. 20 -11. 33, p<0. 001 • Incentive cost of $449 per 12 -week quitter
Headlines • Referrals went from 138 per year to 300 per year; more than doubling • Number of women setting a quit date went from 46 per year to 145 per year; approximately tripling • Number of 12 -week quitters went from 5 per year to 67 per year; a 13 -fold increase.
Conclusion • Financial incentives implemented within a stop smoking service can have a positive impact on priority groups, such as pregnant women who smoke
Vaping New Zealand’s Response
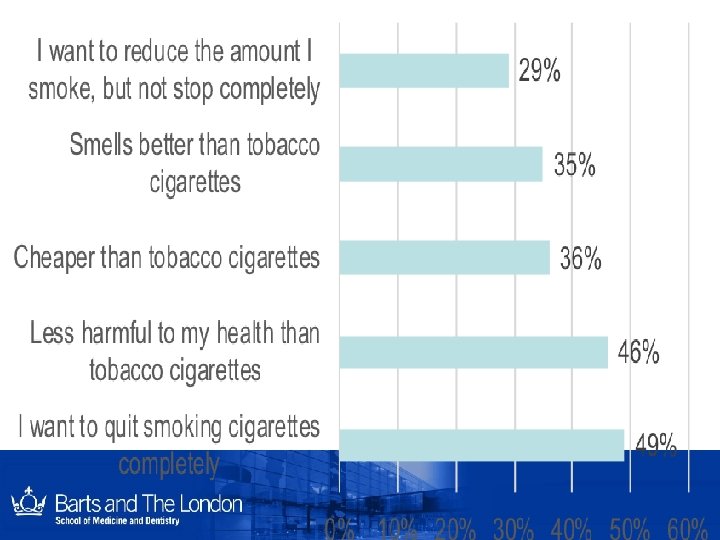
Current Use Prevalence Reasons for use Top 5 reasons for vaping among vapers who vape at least monthly Ever use Current use* 65% *vape daily, weekly, monthly or less often than monthly reported using nicotine containing e-cigarettes HPA 2016 Health and Lifestyles Survey
Youth experimentation 7% 20% 28%
Government response Ministry of Health undertakes public consultation – 250 submissions received June 2016 Cabinet Social Policy Committee (SOC) agrees, in principle, to nicotine ecigarettes being lawfully available for sale and supply, with appropriate controls August 2016 March 2017 Considered again at SOC; agree to start the process to start legislative changes New coalition government September 2017 October 2017 Technical Expert Advisory Group on Electronic Cigarette Product Safety established to support the introduction of an electronic regulatory scheme
Public Consultation Vapers / Vaping Organizations 39% % agree with allowing sale of nicotine EC % agree with R 18 restriction % agree with tobacco-like ad restrictions 100% 84% 37% 14% 23% 87% 98% 250 submissions Non-vapers 61% 97% 90% 65% * % agree to point of sale display ban % agree to prohibit use in smokefree areas % agree to good manufacturing standards 43% * 58% * 84% Agree with legalizing the sale and supply of nicotine e-cigarettes * Statistically significant difference
Mo. H position statement • The Ministry of Health believes e-cigarettes – have the potential to make a contribution to the Smokefree 2025 goal, and – could disrupt the significant inequities that are present. • The potential of e-cigarettes to help improve public health depends on the extent to which they can act as a route out of smoking for New Zealand’s 550, 000 daily smokers, without providing a route into smoking for children and non-smokers. http: //www. health. govt. nz/our-work/preventative-health-wellness/tobacco-control/e-cigarettes
Legal status Ministry of Health vs. Philip Morris (March 2018) • PM was charged with selling ‘Heets’ – contrary to section 29(2) of the SFEA, which reads – • • • No person shall import for sale, sell, pack or distribute any tobacco product labelled or otherwise described as suitable for chewing, or for any other oral use (other than smoking). The Ministry’s argument was that the words ”other than smoking” refer to an ignited product, which Hn. B are not The defence argues that s 29 was never meant to capture inhalation based products The judge agreed with the defence, stating: – “…it can be said that the use of ‘Heets’ while it may have associated risks in itself, is not as harmful or potentially harmful as ordinary cigarette use. This finding would fit squarely with the purposes stated in s 3 A (1)(a) and (c) and s 21 (b) of the Act. http: //www. districtcourts. govt. nz/all-judgments/2018 -nzdc-4478 -moh-v-morris/
Court Decision • This means that vaping and heated tobacco products may be legally imported, sold and distributed in New Zealand
Implications • Vaping and heated tobacco products may be legally imported, sold and distributed in New Zealand • The same SFEA regulatory controls apply to smoked tobacco, heated tobacco and vaping products that are manufactured from tobacco • This includes the ban on sales to minors and restrictions on advertising
Implications • However, the ban on smoking in indoor workplaces, early childhood centres and schools only applies to smoking, and not to vaping or products that are not smoked • Individual employers and business owners decide whether or not to include vaping in their smokefree policies.
Difficulties for policy makers • Evidence base – Do vaping products help people quit? – Safety of long-term use – Use by never smokers (especially young people) • Current legislation
Vaping as a cessation tool • Vaping is a popular quitting tool • Vaping can help some people to quit smoking Cochrane Review “There is evidence from two trials that ECs help smokers to stop smoking in the long term compared with placebo ECs. However, the small number of trials, low event rates and wide confidence intervals around the estimates mean that our confidence in the result is rated ’low’ by GRADE standards. ” Hartmann-Boyce J, Mc. Robbie H, Bullen C, Begh R, Stead LF, Hajek P. Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews 2016,
Health Harm
Moving forward • The SFEA needs to be amended to account for these new products • Need for proportionality in regulatory controls – The greater the harm the more tightly regulated • Need for some degree of flexibility – Adjustments may be required in the light of new evidence • Need for standards for vaping products – These are in development and are expected to become mandatory when the Smoke-free Environments Act is amended • Strengthen surveillance
Final words • Academic institutions have an important role in assisting policy makers in: – translating the evidence into practice – finding the appropriate response when the evidence is not as strong as we would like it to be • Whilst there are differences in opinion, finding the common ground is likely to be more productive in changing policy • The research priorities should address the key challenges in the policy environment
Thank you hayden@thedragon. institute