Transitions of Care What We Need to Why











- Slides: 13
Transitions of Care: What We Need to Why are. Know we involved? www. ntocc. org
Current State of Healthcare Ø Ø Care is complex Care is uncoordinated Information is often not available to those who need it when they need it As a result patients often do not get care they need or do get care they don’t need IOM, Crossing the Quality Chasm
What is “Transition of Care” Ø Ø The movement of patients from one health care practitioner or setting to another as their condition and care needs change Occurs at multiple levels – Within Settings l l – Between Settings l l l – Primary care Specialty care ICU Ward Hospital Sub-acute facility Ambulatory clinic Senior center Hospital Home Across health states l l Curative care Palliative care/Hospice Personal residence Assisted living (c) Eric A. Coleman, MD, MPH
What is “Transitional Care? ” Ø Ø Ø A set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location Based on a comprehensive care plan and availability of welltrained practitioners that have current information about the patient's goals, preferences, and clinical status. Includes: – Logistical arrangements – Education of the patient and family – Coordination among the health professionals involved in the transition Coleman EA, Boult C. J Am Geriatr Soc 2003; 51: 556 -7.
Ineffective Transitions Lead to Poor Outcomes Ø Ø Ø Wrong treatment Delay in diagnosis Severe adverse events Patient complaints Increased healthcare costs Increased length of stay Australian Council for Safety and Quality in Health Care. Clinical hand-over and Patient Safety literature Review Report. March 2005. Available www. safetyandquality. org/internet/safety/publishing. nsf/Content/ AA 1369 AD 4 AC 5 FC 2 ACA 2571 BF 0081 CD 95/$File/clinhovrlitrev. pdf
Transition Issues Dramatically Impact Patient Care Patient ER ICU OUTPATIENT: • Home • PCP • Specialty • Pharmacy • Case Mgr. • Care Giver In-Patient SNF Patient ALF
Transition Issues Dramatically Impact Patient Care NO Discharge Care Plan Patient ER NO Medication Reconciliation NO Personal Medicine List NO Coordinated Care Plan ICU OUTPATIENT: • Home • PCP • Specialty • Pharmacy • Case Mgr. • Care Giver In-Patient SNF Patient ALF NO Care Plan NO Medication Reconciliation NO Personal Medicine List
What Can We Do …
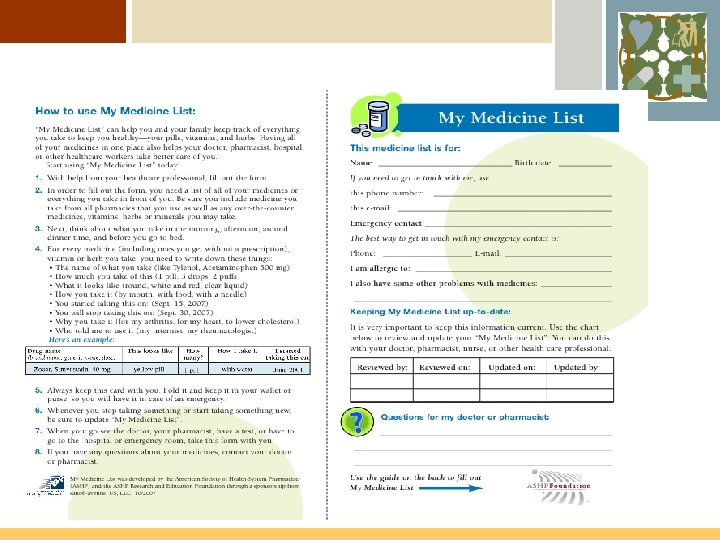
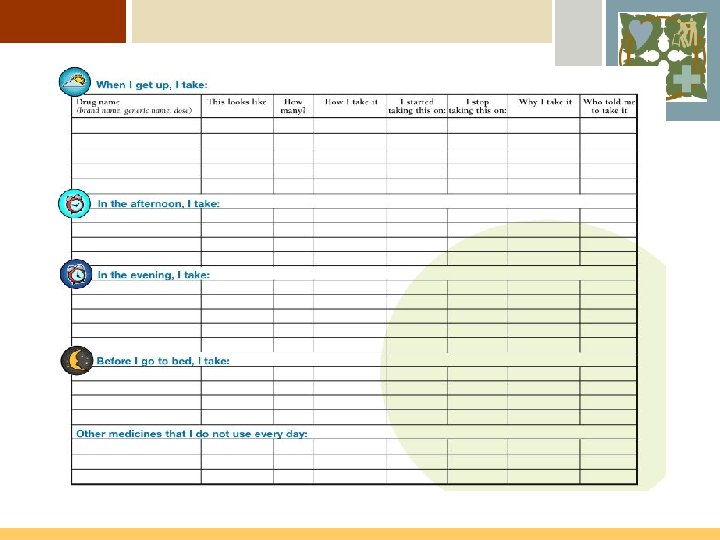
Keep A Medication List Ø Ø Ø Develop your “My Medicine List” You can get started with a simple tool by NTOCC Download the tool from the website Complete the tool with your personal medications Share that information with each clinician you see whether in the ER, hospital, doctor’s office, clinic or pharmacy
The NTOCC Tools Make it Possible to Address the Transition Issues Medication Reconciliation Data Elements + Care / Case Transition Process My Med List ER ICU In-Patient OUTPATIENT: • Home • PCP • Specialty • Pharmacy • Case Mgr. • Care Giver Patient SNF ALF
Watch for New Patient Tools Over the Next Few Months www. ntocc. org