Transfusion Therapies Of Blood Components In ICU Presenter

Transfusion Therapies Of Blood & Components In ICU. Presenter: Dr. Geethika REDDY. P Moderator: Dr. B. S. K. Prust y

Effective blood transfusion therapy depends on availability of different blood components Components used separately or in combination can meet most patients transfusion needs and keep the risk of transfusion to minimum

�Transfusion key element is to decrease in mortality &morbidity in critically ill pt’s by: �Increase in o 2 delivery �Correction of hemostatic abnormalities

Presentation Aims: • To discuss the following: • The various components available • The rational use of blood and components(dosage nd effects) • Complications • Methods to mimimize complications

Theoretical Yield of components � 1 unit of whole blood theoretically gives Whole Blood Processed within 6 hours ) Packed red blood cells Fresh frozen plasma Platelets

Component preparation � Principle : -Differential centrifugation � Red cells ◦ ◦ Plasma + Platelets Packed cells Leukocyte poor rbcs Washed rbcs Irradiated rbcs � Plasma � Platelets � Cryoprecipitate � Pcc(prothrombin complex concentrate) ◦ Fresh frozen Whole blood RBC Buffy

Centrifugation Principle Sediment of blood cells depend on their size as well as the difference of their density from that of the surrounding fluid, viscosity of medium, flexibility of the cells. 30/11/49 MD-3 -49 7
 Platelets")
1. Give only what is needed Red cells O 2 carrying capacity (Anemia) Platelets Thrombocytopenia FFP Multiple clotting factor deficiency CRYO Fibrinogendeficiency

2. Different Storage Conditions Comp. Temp. Red cells 4 -60 C FFP - 40 0 C Platelets Shelf life 35 -42 days 1 year 20 -240 C on platelet agitator 5 days CRYO- 400 C 1 Year

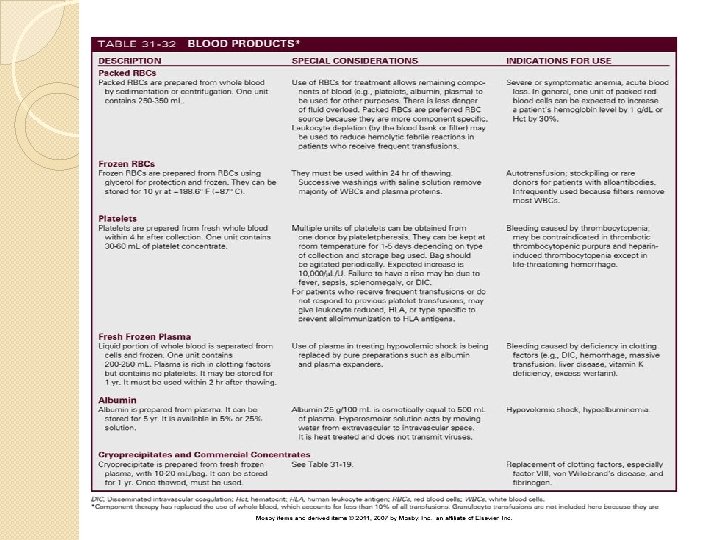
‘Whole Blood : � To replace blood volume and O 2 carrying capacity in � Treat hemorrhage and shock. � Exchange transfusion � Contains PRB’C, plasma proteins, clotting factors and plasma � (few platelets & granulocytes) � Volume = 500 ml/unit � Risks & Benefits: � Possible incompatibility issues � Circulatory overload � **Deficient in some clotting factors � Rarely used � Use Lasix to prevent overload �
 �<50 cc plasma+additive")
PRed cells q 1 unit : 200 ml rbc (no plts) �<50 cc plasma+additive �Total 300 ml �@4 deg c 35 -42 days storage lyf �Neaver preservative agent: adenine � 1 unt: has htcrt app 60% & inc hb by 1 gm%& hrt by 3% �Rate: 1 ml/min �Rtt; 3 -4 hrs per unit of prbcs in hemodynamically stable pt.

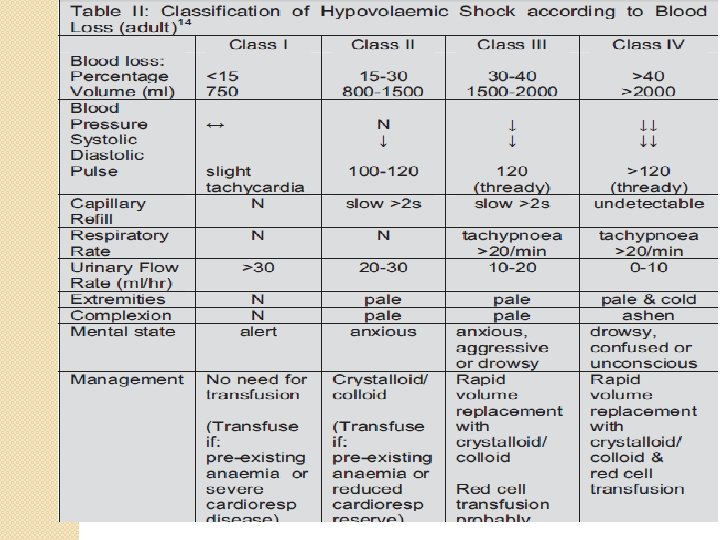
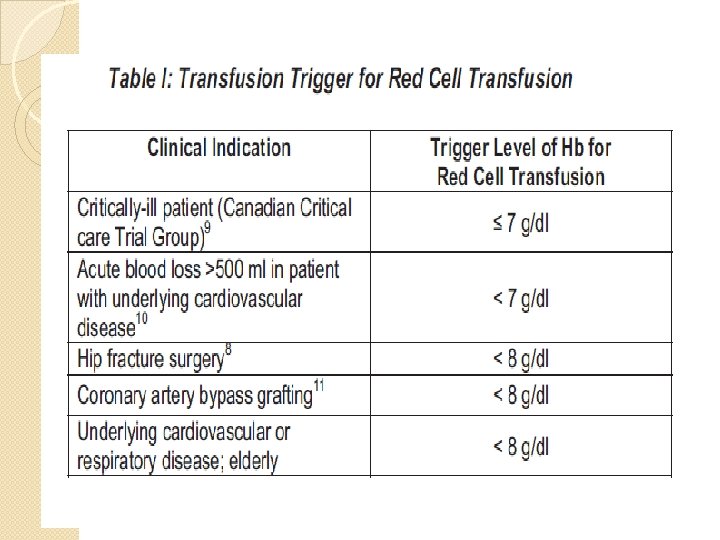
Indications: 1. 2. 3. 4. 5. Hb level alone no more trigger for transfusion. Becoz no relation with oxygenation Or may b becoz of dilutonal effect Indicted: if hb level <7 -9 gm/dl in critically ill pt/trauma pt/with stable cardiac disesase Hb<10 gm/dl in acute coronary syndrome with anemia

Whole blood vs Packed red cells Parameter Whole blood Volume Increment in Hb 350 – 450 ml 1 -1. 5 gm/dl Red cell mass /ml Viable platelets Labile factors Plasma citrate Allergic reactions FNHTR Risk of TTI Packed red cells 200 – 240 ml 1 -1. 5 gm/dl Same as PRBC No No ++++ Same as WB + + No No + + +

PLATELETS �Platelet units can be either �Random donor units �Apheresis units � 1 random donor unit contains 5 k 10 kplatelets � 1 apheresis unit contains 25 k 30 kplatelets

�PRdp=6 -8 units of plts from separate donor into single bag but frm same abotype �Adult dose: 1 unit/10 kg � 4 -6 units of rdp for prophylactic trnsfn � 70 kg: 1 unt inc upto 10 k plt /microl in N spleen �Survival: 3 -5 days �Apheresis plt sdp: 4 -6 pooled units+200250 plasma

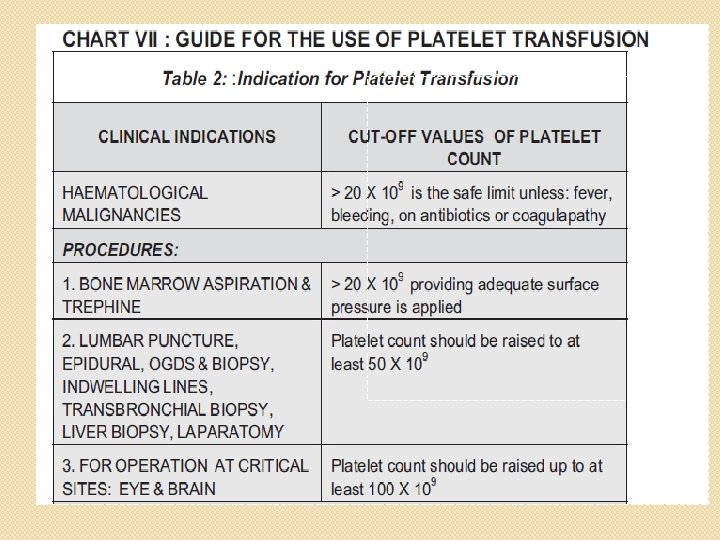
Guidelines for Platelet Tx. Mild - 50, 000 -1, 000/µl Tx - usually not required Moderate - 20, 000 -50, 000/µl Tx-if symptomatic or has to undergo surgery/trauma Severe - < 10, 000/µl Risk of bleeding - high Prophylactic Tx

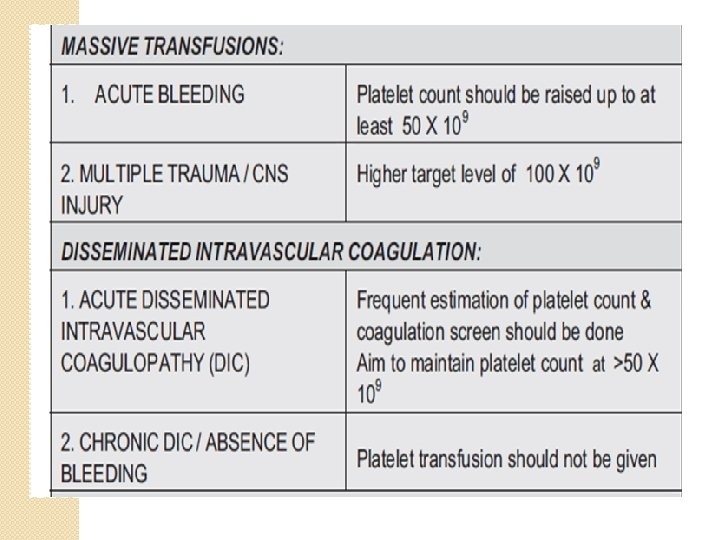
�<50 k in MT inc risk of microvascular bleedi. Ng becoz of dil. thrombocytopenia

IMPORTANT PRECAUTIONS �Stored at 20 -24 Degree celcius. �Constantly agitated �Only last for 5 days �Infused in 30 mins

Indications for platelet transfusion �BLEEDING due to thrombocytopenia �Dysfunctional �Prevention plts of spontaneous bleeding with counts < 10, 000

�Typically in: �Leukemias �Myelodysplasia �Aplastic anemia �Solid tumors �Congenital or acquired/meds inducedplt dysfun �SOMETIMES Cardio pulmonary bypass
, DIC(disseminated")
Causes of thrombocytyopenias Production - Aplasia / Neoplasia Usage - TTP(thrombotic thrombocytopenic purpura), DIC(disseminated intravascular coagulation) Trauma, obs emrgency, sepsis some drugs Destruction – ITP, HIT , HUS, Sequestration – Hypersplenism

platelets �Triggers of transfusion: �Prophlactically in chemotherapy, hematopoetic stem cell transfusion evn with out bleeding �With co morbidities if <10 k �Invasive proceedures: 30 k -50 k �Neurology/opthamology proceedures: 1 lak

C/I �TTP �HUS �HIT �Itp in the absence of bleeding �PROTHROMBOTIC CONDITONS ND TRANSFUSION -FUEL THE FIRE.

FFP �Fresh Frozen Plasma �Plasma collected from single donor units or by apheresis �Frozen within 8 hours of collection �-40 o C �Can last for a year

Fresh Frozen plasma Fresh frozen plasma – labile & nonlabile clotting factors, albumin and immunoglobulin. Factor V&VIII level at least 70 % of normal fresh plasma level Storage - 40 o C for 1 yr, - 65 o C for 7 yrs. - Before use thawed at 37 o C �

Fresh frozen plasma Indications: � Replacement of multiple coagulation factor deficiencies ass wit acute DIC • In the presence of bleeding and abnormal coagulation parameters following massive transfusion or cardiac bypass surgery or in patients with liver disease • Anticoagulant overdose(reversal of warfarin effect in the presence of potentiallylife-threatening bleeding when used in addition to vitamin K)

Managing Patients with High INR Values Minor or No Bleeding Clinical Situation Guidelines INR >therapeutic range but <5. 0, no clinically significant bleeding, rapid reversal not indicated for reasons of surgical intervention Lower the dose or omit the next dose; resume warfarin therapy at a lower dose when the INR approaches desired range If the INR is only minimally above therapeutic range, dose reduction may not be necessary INR >5. 0 but <9. 0, no clinically significant bleeding Patients with no additional risk factors for bleeding; omit the next dose or two of warfarin, monitor INR more frequently, and resume warfarin therapy at a lower dose when the INR is in therapeutic range Patients at increased risk of bleeding: omit the next dose of warfarin, and give vitamin K 1 (1. 0 to 2. 5 mg orally) Patients requiring more rapid reversal before urgent surgery or dental extraction: vitamin K 1 (2– 4 mg orally); if the INR remains high at 24 h, an additional dose of 1– 2 mg

Managing Patients with High INR Values & Bleeding Clinical Situation Guidelines INR >9. 0, no clinically significant bleeding Vitamin K 1 (3– 5 mg orally); closely monitor the INR; if the INR is not substantially reduced by 24 h, the vitamin K 1 dose can be repeated Serious bleeding, or major warfarin overdose (e. g. , INR >20. 0) requiring very rapid reversal of anticoagulant effect: Vitamin K 1 (10 mg by slow IV infusion), with fresh plasma transfusion or prothrombin complex concentrate, depending upon urgency; vitamin K 1 injections may be needed q 12 h Life-threatening bleeding or serious warfarin overdose FFP with vitamin K 1 (10 mg by slow IV infusion); repeat if necessary, depending upon the INR Continuing warfarin therapy indicated after high doses of vitamin K 1 Heparin, until the effects of vitamin K 1 have been reversed, and patient is responsive to warfarin

FRESH FROZEN PLASMA Indication q Clinically significant deficiency of Factors II, V, X, XI q Depletion of coagulation factors in pts receiving large volume transfusion qdilutional and consumption coagulopathy Contraindication Volume expansion Immunoglobulin replacement Nutritional support Wound healing 33

FRESH FROZEN PLASMA Precaution Acute allergic reaction are common Anaphylactic reaction may occur Hypovolemia alone is not an indication for use Dosage - Initial dose of 15 -20 ml /kg Administration Must be ABO compatible, Rh not required Infuse as soon as possible after thawing ( within 6 hrs ) using standard blood administration set

Dosage & Administration for FFP Dosage - 10 -15 ml/Kg(Approx 2 -3 bags for an adult) Administration - Thawed at +37 o C before transfusion ABO compatible Group AB plasma can be used for all patient

cryoprecipitate �Cryoprecipitate – Clotting Factors VIII, XIII, von Willebrand’s factor, & fibrinogen from plasma �Used to treat clients with specific clotting factor deficiencies �May cause ABO incompatibilities �Prepared from FFP �Store for 1 year, once thawed > use

�Supplied in: bags made frm multiple donors nd resuspended in normal saline& pooled prior to transfusion @room temp �Each unit : 10 -15 ml �Concn of fibrinogen in 1 UNIT cryo =1 unt ffpi. e: 150 -250 mg t-half: 100 -150 hr �Fac VIII: 80 -150 U �Fac XIII: 50 -75 U �V-WF: 50 -75 U

�Inds: V-Wd Hemophila Fac-13 def Hypofibrigenomie/dysfibrigenom ia with bleeding

�Amnt of fibrinogen varies/bag depends on donor fibrinogen concn �For fac 8 nd vwf def usual doses 1 bag/10 kg app=150 units of fac-8 & VWf �In elective sx autologus plasma donation for processing to cryo.

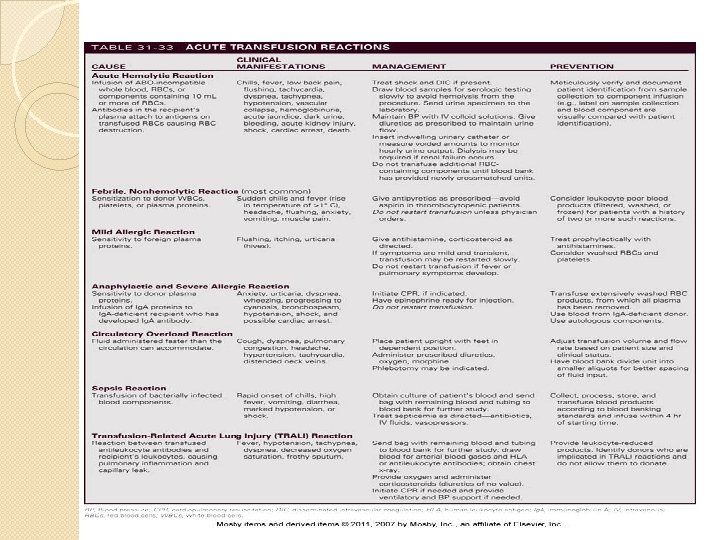
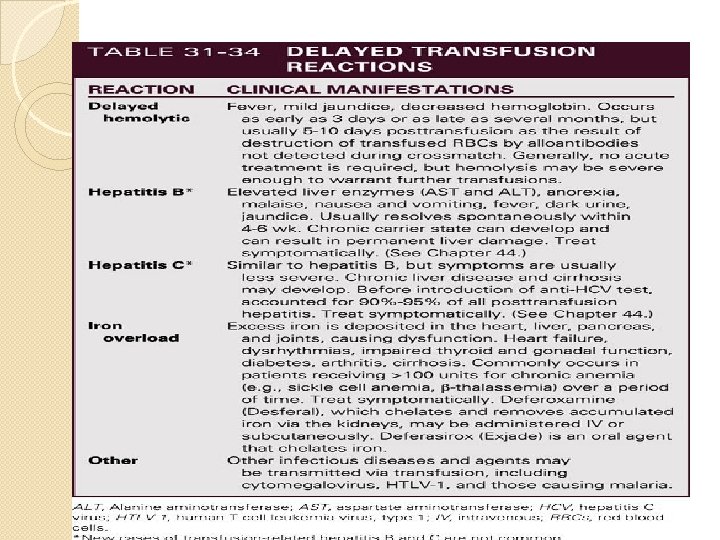
Complications �Infectious: ELISA �Pcr-Hcv, Hiv for anti HIV ab’s r-na �Cmv is a dna virus. Primary infec with body secretions/bp/organ allografts �Contamination with bacteria while sample collection �Plts are more contaminated. �Symptoms nd further?

�Trnsfsn rxns: AHTR �DHTR �FNHTR �TRALI �A&A �TAGVH.
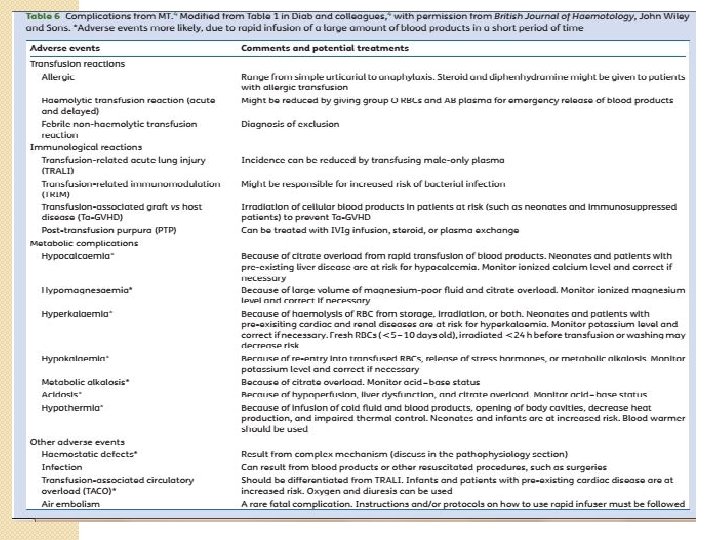
, Citrate in blood binds with calcium & is excreted. �Hyperkalemia:")
�Hypocalcemia (massive blood transfusions), Citrate in blood binds with calcium & is excreted. �Hyperkalemia: stored blood liberates potassium through hemolysis �Acid base disorders: lactic acid contributes to overall acidosis �Hypothermia �Ards

MASSIVE TRANSFUSION PRTOCOL:

pathophysiology

�Early use of rbc, plasma, platelets@1: 1: 1 ratio nd reduced crystalloid use in resuscitation proven dec morbidity&mortality in MT �This rationale more closely resembles wb. �Helps to treat&prevent ETIC �Demonstrated improved pt survival reduced organ failure nd post traumatic complications

�MASSIVE HAGE M/C/C OF SHOCK IN OBGY PTS �MT CAUSE: GI-H’AGE, MAJOR Srxsi. e CARDIAC SPINAL, LIVER, multivisceral transplatation. �Early recognisation results in improved outcomes in mb pts �Predictors of mt in trauma pts: �Trauma associated sev h’age score: 7 lab findings �Most rapidly by penetrating trauma, sbp<90, hr>120, +ve sonography for trauma

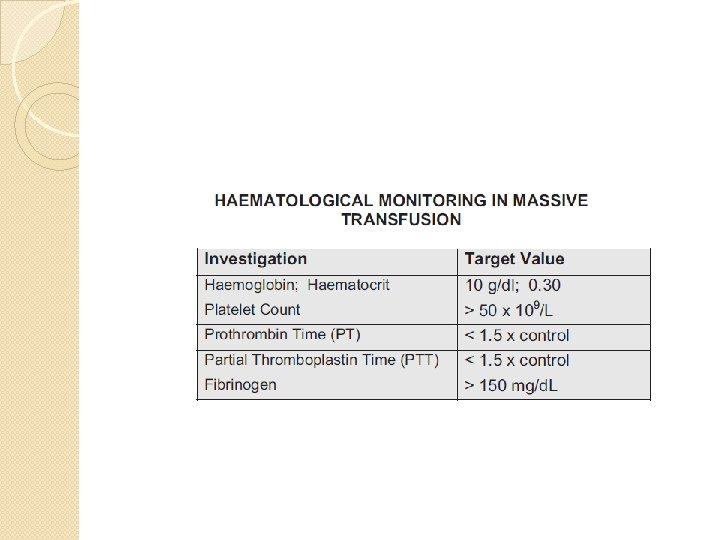
Coagulation Factor Depletion: � �� Only mild reductions in total coagulation facto caused by � dilutional effect in massive transfusion. Disordered haemostasis is more likely to be due to disseminatedintravascular coagulation (DIC): � Platelet count <50 x 109/L � Prolonged PT and APTT (>1. 5 x control) � Hypofibrinogenaemia <150 mg/dl � Elevated fibrinogen degradation products � Clinically widespread microvascular bleeding � DIC is more likely if resuscitation is delayed or inadequate

Bibilography Annals of intensive care-a springer open jornal � National blood center ministry of health guidelines � Boston medical center icu manual by allen walkey � The new england journal of medicine � Indian journal of anesthesia for blood transfusion in critical care � British journal of anasthesia � society of critical care medicine � Clinical transfusion guideliness for mrdical interns � Irwine nd rippe 6 th edition , paul l marino, washington manual of crtical care medicine, harrison. �

SPL THANKS TO DR. NANDA KISHORE SIR. .
- Slides: 54