TRANSFUSION RELATED ACUTE LUNG INJURYTRALI BY DR PARESH
 BY: DR. PARESH PATEL UNIQUE HOSPITAL SURAT.")
TRANSFUSION RELATED ACUTE LUNG INJURY(TRALI) BY: DR. PARESH PATEL UNIQUE HOSPITAL SURAT.

Definition � TRALI is defined as an acute lung injury that is temporally related to a blood transfusion; specifically, it occurs within the first six hours following a transfusion. � It is typically associated with plasma components such as platelets and Fresh Frozen Plasma, though cases have been reported with packed red blood cells since there is some residual plasma in the packed cells. � TRALI is now among the three leading causes of transfusion related fatalities along with ABO incompatibility and bacterial contamination. � TRALI is associated with a significant mortality rate, often approximated at 5 to 10%

Incidence � The true incidence of TRALI is unknown because of the difficulty in making the diagnosis and because of underreporting. It is estimated to occur in 1: 1300 to 1: 5000 transfusions of plasma-containing products. � The mortality rate from TRALI ranges from 5% to 10%. Most patients recover within 48 -72 hours and CXR returning to normal within 72 -96 hours � Plasma containing blood product such as whole blood, platelet concentrates, fresh frozen plasma (FFP) , packed red cells, cryoprecipitate and intravenous immunoglobulin have all been implicated as a possible cause of TRALI.

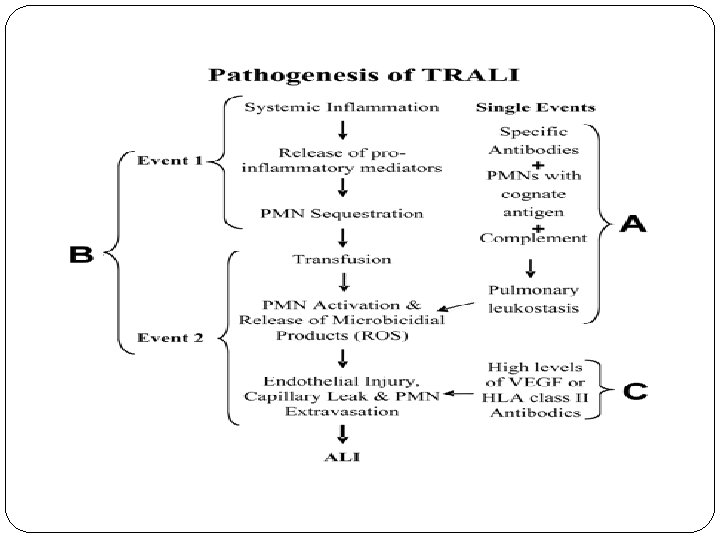
Pathogenesis of TRALI The exact pathogenesis of TRALI is not known thus several theories have been proposed for the pathogenesis of TRALI for immune competent hosts. � It is hypothesized that TRALI may be precipitated by the infusion of donor antibodies directed against recipient leukocytes. The infusion of donor anti-HLA (human leukocyte antigens) or anti-HNA (human neutrophil antigens) antibodies is thought to directly cause complement activation, resulting in the influx of neutrophils into the lung, followed by neutrophil activation and release of cytotoxic agents, with subsequent endothelial damage and capillary leak

WBC Antibody Hypothesis �Antigen-Antibody reaction triggers TRALI Activation Donor -Anti-HNA -Anti-HLA II Release of substances causing pulmonary endothelial damage and capillary leak Lodged in pulmonary capillaries Recipient WBC - Neutrophils - Lymphocytes - Monocytes Courtesy of Y. Lin

�An alternate hypothesis argues that TRALI is the result of at least two independent clinical events: the first is related to the clinical condition of the patient (infection, cytokine administration, recent surgery, or massive transfusion) that causes activation of the pulmonary endothelium. �This then leads to the sequestration of primed neutrophils to the activated pulmonary endothelium.

�The second event is the infusion of donor derived anti-HLA or anti-HNA antibodies directed against antigens on the neutrophil surface and/or biological response modifiers (e. g. , lipids) in the stored blood component that activate these adherent, functionally hyperactive neutrophils, causing neutrophil-mediated endothelial damage and capillary leak. �Third hypothesis suggests that high levels of donor derived vascular endothelial growth factor (VEGF) or antibodies to class II HLA antigens residing on pulmonary vascular endothelium may directly cause endothelial shape change and fenestration.
")
Two event hypothesis 1 st event: Underlying clinical condition of patient (inflammation, infection, surgery) 2 nd event: Transfusion of biologically active lipids or antibodies Activation Release of substances causing pulmonary endothelial damage and capillary leak Activation of pulmonary endothelium with increased adhesion molecules Silliman et al. Blood 2003; 101: 454 -62 Kleinman et al. Transfusion 2004; 44: 1774 -89

Criteria For TRALI �Acute onset hypoxemia. �Ratio of Pao 2/Fi. O 2 <300 or Sp. O 2 <90% at room temperature. �Occur during or within 6 hours before transfusion. �B/L diffuse pulmonary infiltrates �No evidence of left atrial hypertension(i. e. circulatory overload).

Clinical feature �Dyspnoea / respiratory distress requiring o 2 support. �Requiring mechanical ventilation-70% �Hypoxemia. �Cyanosis-very common. �Hypotension- majority. �Fever-very common �Clinical exam reveals respiratory distress and pulmonary crackles may be present with no signs of congestive heart failure or volume overload.
,")
�CXR shows evidence of bilateral pulmonary edema unassociated with heart failure (non-cardiogenic pulmonary edema), with bilateral patchy infiltrates, which may rapidly progress to complete "white out" indistinguishable from Acute Respiratory Distress Syndrome (ARDS).

Normal CXR Patient’s CXR

Diagnostic feature of TRALI �Onset within 1 -6 hrs of transfusion. �Acute respiratory distress. �Acute b/l pulmonary oedema (non-cardiogenic). �Severe hypoxemia. �Hypotension. �Fever. �No evidence of circulatory overload
 - develops within minutes to hours of transfusion")
Differential Diagnosis �Transfusion-associated circulatory overload (TACO) - develops within minutes to hours of transfusion as respiratory distress with tachypnea, tachycardia, hypertension, and cyanosis. It rapidly responds to aggressive diuresis and ventilatory support. �Acute Hemolytic transfusion reaction (AHTR)- may overlap with TRALI, they are easily distinguished by the presence of hemolysis. �Transfusion-related bacterial sepsis-after transfusion of contaminated peripheral red blood cells (PRBCs) or platelet concentrates manifests as fever, hypotension, and vascular collapse, which may include respiratory distress, and must be considered in patients with

�Anaphylactic transfusion reactions- involve respiratory distress related to bronchospasm manifested by tachypnea, wheezing, cyanosis, and severe hypotension. Facial and truncal erythema and edema are common. The respiratory distress from anaphylactic transfusion reactions is related to laryngeal and bronchial edema rather than to pulmonary edema, as in TRALI. These reactions occur rapidly during the transfusion of any type of protein-containing blood component and may occur after the transfusion of small volumes of blood.

TRALI Vs TACO TRALI � Fever � Hypotension � JVP unchanged � EF- normal � Pulmonary edema fluidexudate � Response to diureticminimal � WBC - Transient leukopenia. � BNP <200 pg/ml TACO � No fever � Hypertension � JVP can be changed � EF- Decreased � Pulmonary edema fluid- Transduate � Response to diuretic. Significant improvement � WBC- Unchanged � BNP- >1200 pg/ml

Immediate Management of TRALI 1. 2. 3. 4. 5. 6. Stop the transfusion immediately. For mild cases Supplemental O 2 and supportive care may be sufficient. For the most severe case- mechanical or non invasive ventilation and invasive monitoring may be required. Others less well documented and unproven therapies (eg. Diuretics, corticosteroids, etc) have also been used. Antibiotics – prevention of infection. Extracorporeal membrane oxygenation has been used successfully in a severe case of TRALI.

6. The majority of patients recover within 72 to 96 hours and subsequently recover to their baseline pulmonary function. 7. However, some patients are slower to recover and may remain hypoxic with persistent pulmonary infiltrates up to seven days. 8. Approximately 5 to 10% of cases are fatal in spite of aggressive supportive care.

Prevention of TRALI �Avoiding blood from multiparous women- these women are at risk of producing anti-leucocyte antibodies during previous pregnancy. �Donors whose blood has resulted in TRALI previously or donors known to be leukocyte-alloimmunized (i. e. donors with antibodies to leukocytes) or who are at increased risk of leukocyte alloimmunization”. �Blood which has been stored for long duration- long storage results in production of anti-leucocyte antibodies. �Not to use whole blood. �Leukoreduction - It can be done by ɤ - irradiation of the blood component, or by using micro filters in the transfusion sets, or by using centrifuged blood

Thank you
- Slides: 21