TransCaribbean HIVAIDS Research Initiative A multicultural Caribbean united

Trans-Caribbean HIV/AIDS Research Initiative A multicultural Caribbean united against HIV/AIDS WELCOME Building Cross-Cultural, Trans-National Multidisciplinary Research Collaborations Skills-Building Workshop XVII International AIDS Conference 2008 Mexico City, Mexico August 2008

Workshop Objectives • • Start gathering an inventory of ongoing Caribbean AIDS research; Learn about current opportunities for collaboration; Identify and meet potential collaborators; Understand cultural competencies critical to the conduct of HIV/AIDS research in the region; • Help identify and develop approaches to addressing ethical and cultural issues relevant to the region; • Provide input into strategies for career development of junior Caribbean scientists; and • Return home with essential information on how to pursue collaborations.

MEMBERS OF THE PANEL • Prof. Jean Willian Pape, GHESKIO, Haiti • Prof. Courtenay Bartholomew, Professor Emeritus at the University of the West Indies (UWI), Trinidad and Tobago • Dr. Susan Buchbinder, University of California at San Francisco

MEMBERS OF THE PANEL • Dr. Carmen Zorrilla, Medical Sciences Campus, University of Puerto Rico • Dr. Lydia Santiago, Medical Sciences Campus, University of Puerto Rico • Dr. Patrice Joseph, GHESKIO, Haiti • Dr. Nanet López, Ponce School of Medicine, Puerto Rico

HIV/AIDS CARIBBEAN OVERVIEW • HIV/AIDS continue to be a public health problem affecting the Caribbean. • AIDS remains one of the leading causes of death among people aged 25 to 44 years in the Caribbean.

HIV/AIDS CARIBBEAN OVERVIEW • Sexual intercourse is the primary mode of HIV transmission in the region although injecting drug use is the key factor in HIV transmission in Bermuda and Puerto Rico’s epidemics. • National adult HIV prevalence has stabilized in several Caribbean countries, including the Dominican Republic and Haiti.

HIV/AIDS CARIBBEAN OVERVIEW • An estimated 28 000 people living with HIV started antiretroviral treatment in the region by end-2006. • The scaling up to prevention of mother-to-child transmission of HIV programmes in several countries, including Barbados, Guyana and Jamaica, has significantly reduced the rate of transmission to infants.

HIV/AIDS CARIBBEAN OVERVIEW • In Jamaica, 90% of pregnant women attending public antenatal clinics are now screened for HIV/a sevenfold increase since 2002. • The positive effects of expanded access to antiretroviral therapy in Barbados are evident, with the number of annual deaths attributable to AIDS having decreased by 85% between 2001 and 2006.

HIV/AIDS CARIBBEAN OVERVIEW • Guyana’s programme to prevent mother-to-child transmission of HIV is also expanding, and about 80% of pregnant women accepted prevention of mother-to-child transmission services when offered. • Cuba’s epidemic remains the smallest in the region.

The History of HIV/AIDS Research in Haiti Jean William Pape MD Professor of Medicine, Division of International Medicine and Infectious Diseases Weill Cornell Medical College, New York, NY Director, Centres GHESKIO, Port-au-Prince, Haiti TCHARI Skills Building Workshop Mexico city Centro Banamex, Palacio de Canal AIDS 2008 conference venue

HIV/AIDS Research in Haiti Linked to the creation in 1982 of the Haitian Study Group on Kaposi Sarcoma and Opportunistic Infections (GHESKIO) l GHESKIO and PIH created models of comprehensive research, services, and training programs that have been scaled-up nationwide with major public health impact l Highly successful despite the fact that Haiti has highest rate of HIV outside of Africa l GHESKIO

First Research Intervention in Haiti 1980: JW Pape established a treatment and research unit for infants at the State University Hospital in PAP, Haiti. The mortality decreased from 40% to less than 1% in one year with the introduction of oral rehydration therapy and careful monitoring of patients.

First AIDS cases and Creation of GHESKIO First AIDS Cases: l – – • 1981: KS and PCP in NY/California: MSM, heroin addicts, hemophiliacs MMWR, 1981, 30: 305 -308: 1982: OI and KS among Haitians in the US: 4 H Disease: Homosexuals, Heroin addicts, Hemophiliacs, Haitians MMWR, 1982, 31: 360 -364 Creation of the Haitian Study Group on Opportunistic Infections and Kaposi’s Sarcoma (GHESKIO) 5/2/1982 – – Mission: Services/Training/Research in HIV and ass. diseases Collaboration with: l l l – US universities: Cornell, Vanderbilt, Virginia, Hastings Center French Institutions: Institut Pasteur, Fondation Merieux Local institutions: Ministry of Health, Haitian Medical Assoc. and > 120 public and private institutions Research Support: l NIH: continuous since 1983; Fogarty; ANRS; Foundation Merieux

1983 and 2005: Two major publications
")
GHESKIO Founders (May 2 nd 1982)

AIDS in Haiti : Scientific challenges 1982 -2008 l 1982 -1990: Define the disease – Can the common OIs be treated? – What are the modes of transmission and cofactors? – What is the natural history of HIV? l 1991 -2002: Can the epidemic be controlled? – Can a model for prevention and care be developed? – Can HAART be introduced? l 2003 -present: Nationwide scale-up of the prevention and model Research has been the backbone of the interventions

The first GHESKIO Generation Marie Eu Beaulieu MT, Head of the lab 1979 -present. Dr Rose Irene Verdier Head Clinics 1984 -present Dr Reynold Grand Pierre Head Expansion, 1988 -present Yonie Cadot, Head Nurse 1979 -present 1983 -present

Major Collaborators Peter F Wright, Vanderbilt Warren D Johnson Jr, Cornell Alain Mérieux, Fondation Rodolphe Mérieux

Pressing Clinical Issues Coccidia associated chronic diarrhea l TB: Diagnosis, Prevention, Treatment l Dermatologic presentations l Kaposi Sarcoma: Liautaud B, Pape JW, Laroche AC, et al. Sarcome de Kaposi et SIDA en Haiti. Nouvelles Dermatologiques 5 suppl) 1986; 80 -6. Bernard Liautaud MD Prurigo: A common initial manifestations of AIDS in Haiti. Liautaud B et al Arch. Derm, 123: 625, 1989

GHESKIO Publications on Chronic Diarrhea l l l l l l De. Hovitz JA, Pape JW, Boncy M. and Johnson WD Jr. Clinical manifestations and therapy of Isospora belli infection in patients with the acquired immunodeficiency syndrome. N Engl J Med 1986; 315: 87 -90. Pape JW, Gerdes H, Oriol, Johnson WDJr. Typhoid fever: successful treatment with cefoperazone. J Inf Dis 1986; 153: 272 -6. Pape JW, Levine E, Beaulieu ME, Marshall F, Johnson WD Jr. Cryptosporidiosis in Haitian children. Am J Trop Med & Hyg 1987; 36: 333 -7. Pape JW, Balasubramanyan R, and Rohde JE: Intestinal Illness, IN Medical Care of Refuges. R. A. Sandler and T. C. Jones (eds), New York Oxford University Press, 1988, pp. 364 -3. Pape JW. Treatment of gastrointestinal infections. AIDS 1989; 2: 161 -7. Pape JW, Verdier R-I, and Johnson WD. : Therapy and prophylaxis of Isospora belli infection in patients with the acquired immunodeficiency syndrome. N Engl J Med 1989; 320: 1044 -7. Pape JW and Johnson WD Jr: Salmonella and Shigella, IN Internal Medicine: A Systemic Approach, Stein JH(ed) Little Brown and Co, 3 rd Ed, New York, 1990, pp. 1491 -6. Pape JW. Johnson, WD Jr. Isospora belli infection. Prog in Clin Parasit 1991; 2; 119 -27. Pape JW, Verdier R-I, Boncy M, et al. : Treatment and prophylaxis of Cyclospora species infections in AIDS patients. Ann Int Med 1994; 121: 9; 654 -7. Steiner TS, Pape JW, Guerrant RL: Intestinal Coccidial In Infections, IN Tropical Infectious Diseases, Principles, Pathogens, and Practice, R. L. Guerrant, D. W. Walker, P. Weller, (eds), Churchill Livingstone, Division of Harcourt Brace & Co. Philadelphia, Pennsylvania, 1999, pp. 721 -735. Verdier R-I, Johnson WD Jr, Pape JW. Treatment and prophylaxis of isosporiasis and cyclosporiasis with trimethoprim- sulafamethoxazole versus ciprofloxacin: a comparative study. Ann Int Med 2000; 132: 885 -8. Fitzgerald D, Pape JW: Cyclosporiasis in Current Treatment Options Infect Dis 2001, 3: 345 -349. Kirkpatrick BD , Daniels MM, Jean SS, Pape JW, Karp C, Littenberg B, Fitzgerald DW, Lederman H, Nataro JP. Cryptosporidiosis stimulates an inflammatory intestinal response in malnourished Haitian children. J Infect Dis 2002; 186; 94 -101. Champetier de Ribes G, Fline M, Desormeaux AM, Eyma E, Montagut P, Champage C, Pierre J, Pape JW, Raccurt CP. Intestinal helminthes in school children in Haiti. Bull Soc Patho Exot 2005, 98. Raccurt CP, Stockman CP, Verdier RI, Eyma E, Totet A, Nevez G, Pape JW Parasites intestinaux et SIDA en Haiti: risques lies a l’entourage familial. Accepted fo publication. Bull Soc Path Ex 2006 Raccurt CP, Brasseur P, Verdier RI, Li L, Eyma E, Stockman P, Agnamey P, Guyot K, Totet A, Liautaud B, Nevez G, Dei-Cas E , Pape JW Cryptosporidiose humaine et espèces en cause en Haïti. Trop Med Int Health 11: 6; 929 -934, 2006 Kirkpatrick BD, Wallace AK, Waganer D Noel F, De. Matteis P, Bois G, Pape JW, Sears CL. Serum Mannose-binding lectin deficiency is associated with cryptosporidiosis. CID 43: 289 -94, 2006 Kirkpatrick BD, Noel F, Rouzier PD, Powell JL , Pape JW, Bois G, Alston WK, Larsson CJ, Tenney K, Ventrone C, Powden C, Sreenivasan M, Sears CL. Childhood cryptosporidiosis is associated with a persistent systemic inflammatory response. CID: 43: 604 -8, 2006 Bras A, Evans E, Obison L, Brasseur P, Pape JW, Raccurt C. Biological 6 ` Assessment of cryptosporidium oocysts in drinking water in Port-au-Prince , Haiti, Env, Risques et Santé, 6: 5, 2007 Raccurt CP, Fouche B, Aganmey P, Menotti J, Chouaki T, Totel A, Pape J W; Human intestinal co-infections with Enterocytozoon bieneusi and coccidian in Haiti. Accepted for publication AM J Trop Med Hyg 2008
 De. Hovitz")
Clinical Manifestations and Therapy of Isosporiasis and cyclosporiasis in HIV+ Patients 1) De. Hovitz et al. NEJM 315: 87, 1986 2) Pape et al. NEJM 320: 1044, 1989 1) Pape et al. Ann Int Med 121: 654, 1994; 2) Verdier et al Ann. Int. Med. : 132: 885 -888, 2000

Tuberculosis and HIV Research Questions • • • Can primary TB prophylaxis prevent the development of active TB in those co-infected with HIV and TB? Pape JW et al: The Lancet 342: 1993 Can TB be effectively treated in patients co-infected with HIV? Desvarieux M et al: AMJPH 1997 Do HIV+ patients have recurrence of TB after successful treatment for TB? If so can post treatment TB prophylaxis prevent these recurrences in patients co-infected with HIV? • Fitzgerald D et al; The Lancet 2001; 375 Can persons seeking HIV testing be effectively screened for TB Burgess A et al, AIDS: 15: 1875 -1879 2001

GHESKIO Publications on TB l l l l Pape JW, Jean S, Ho J, Hafner A, Johnson WD Jr. Effect of isoniazid prophylaxis on incidence of active tuberculosis and progression of HIV infection. Lancet 1993; 342: 268 -72. Hyppolite PR and Pape JW: Human immunodeficiency virus and tuberculosis in Haiti. Boletin de la Oficina Sanitaria Panamericana 1995; vol 118, No. 2. Fitzgerald DW, Pape JW, Desvarieux M, Johnson W D Jr. The need for post-treatment tuberculosis prophylaxis in HIV- infected patients successfully treated for tuberculosis. Lancet 2000; 356: 1470 -74. Fitzgerald DW, Morse MM, Pape JW, Johnson WD Jr: Active tuberculosis in HIV-infected individuals who have completed isoniazid prophylaxis: evidence for a dose-dependent post-prophylaxis Effect. Clin Infect Dis 2000; 31: 1495 -7. Fitzgerald DW, Severe P, Joseph P, Noel E, Mellon LR, Johnson WD Jr, Pape JW. No effect of INH prophylaxis for PPD negative HIV infected adults living in a country with endemic tuberculosis. JAIDS 2001; 28: 305 -7. Desvarieux M, Pape JW, Hyppolite PR, Johnson WD Jr. : Efficacy of short-course tuberculosis therapy in HIV-infected patients. Am J PH 2001; 91: 1: 1 -4. Fitzgerald D, Johnson WD Jr, Pape JW. HIV-infection and risk of tuberculosis after rifampicin treatment. Lancet 2001; 357: 9280. Burgess AL, Fitzgerald DW, Severe P, Joseph P, Noel E, Rastogi N, Johnson, WD Jr. , Pape J. Integration of tuberculosis screening at an HIV voluntary counseling and testing center in Haiti. AIDS. 2001; 15: 1875 -9. Fitzgerald DW, Severe P, Joseph P, Noel E, Mellon LR, Johnson WD Jr, Pape JW. No effect of INH prophylaxis for PPD negative HIV infected adults living in a country with endemic TB. JAIDS 2001. 28: 305 -7. Filliol I, Driscoll JR, van Soolingen D, et al, Pape JW, Rasolofo-Razanamparany V, Ridell M, ROssetti ML, Stauffer F, Suffys PN, Takiff H, Texier-Maugein J, Vincent V, de Waard JH, Sola C, Rastogi N. Global distribution of Mycobacterium tuberculosis spoligotypes. Emerg Infect Dis 2002; 8: 1347 -9. Ferdinand S, Sola C, Verdol B, Legrand E, Goh KS, Berchel M, Aubery A, Timothee M, Joseph P, Pape JW, Rastogi N. Molecular characterization and drug-resistance of Mycobacterium tuberculosis isolated patients in an AIDS counseling center in Port-au-Prince, Haiti: A one-year study. J Clin Microbiol 2003; 41: 694 -702. Filliol I, Driscoll JR, van Soolingen D, Pape JW, Rasolofo-Razanamparany V, Ridell M, Rossetti ML, Stauffer F, Suffys PN, Takiff H, Texier-Maugein J, Vincent V, de Waard JH, Sola C, Rastogi N. Snapshot of moving and expanding clones of Mycobacterium tuberculosis and their global distribution assessed by spoligotyping in an international study. J Clin Microbiol 2003; 41: 1963 -70. Pape JW. Tuberculosis and HIV in the Caribbean: Approaches to diagnosis, treatment and prophylaxis. Topics in HIV Medicine 2005 ; 12 : 5 144 -9. Joseph, P, Severe P, Ferdinand S, Goh KS, Sola C, Haas, D. Johnson WD, Rastogi N, Pape JW, Fitzgerald DW. Multi-drug resistant tuberculosis at an HIV testing Center in Haiti, AIDS 2 006, 20: 415 -418
 - HIV- 5/166 (3%)")
MDR-TB and HIV Primary TB Recurrent TB HIV+ 11/115 (10%) - HIV- 5/166 (3%) - RR=3. 2, p=0. 03 TOTAL 16/281 (6%) 10/49 (20%) 330 isolates of mycobacterium tuberculosis over a 2 year period Joseph, P et al, AIDS 2006, 20: 415 -418

Epidemiology of HIV/AIDS in Haiti l Risk factors for AIDS ? l Cofactors for HIV transmission? l Natural history of HIV infections? – Adults – Children
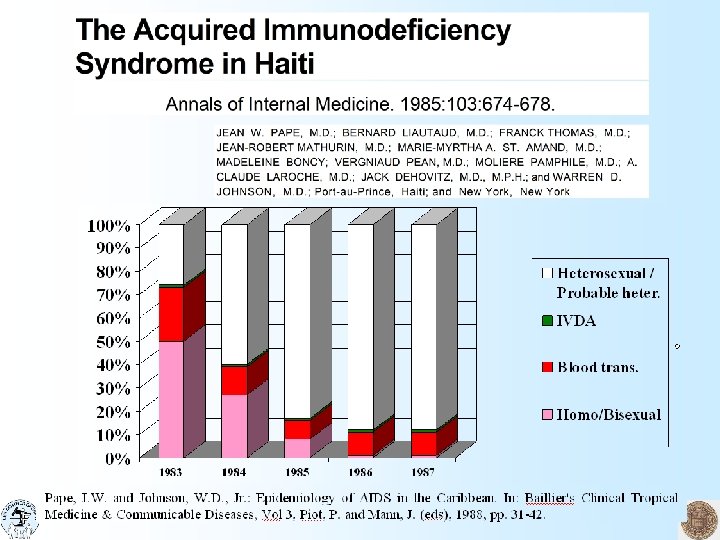

MMWR May 10, 1985 Current Trends Update: Acquired Immunodeficiency Syndrome United States Haitian-born AIDS patients have now been placed into the "other/unknown" group. The previous separate listing for Haitian-born patients has been discontinued in light of current epidemiologic information that suggests both heterosexual contact and exposure to contaminated needles (not associated with intravenous (IV) drug abuse) play a role in disease transmission (5 -7). Similar risk factors have been described for AIDS patients in some central African countries (8 -10). Evidence from surveillance case report forms is insufficient to establish the specific modes of transmission in particular cases reported among Haitian immigrants. References 1) CDC. Update: acquired immunodeficiency syndrome (AIDS)--United States. MMWR 1984; 32: 688 -91. 2) Selik RM, Haverkos HW, Curran JW. Acquired immune deficiency syndrome (AIDS) trends in the United States, 1978 -1982. Am J Med 1984; 76: 493 -500. 3) CDC. Pneumocystis pneumonia--Los Angeles. MMWR 1981; 30: 250 -2. 4) CDC. Kaposi's sarcoma and Pneumocystis pneumonia among homosexual men--New York City and California. MMWR 1981; 30: 305 -8. 5) Pape J, Liautaud B, Thomas F, et al. Characteristics of the acquired immunodeficiency syndrome (AIDS) in Haiti. N Engl J * Med 1983; 309: 945 -50. 6) Pape J, Liautaud B, Thomas F, et al. AIDS: risk factors in Haiti. Washington, D. C. : Twenty-fourth Interscience Conference on Antimicrobial Agents and Chemotherapy, 1984: 99 (abstract #60). 7) Castro KG, Fischl MA, Landesman SH, et al. Risk factors for AIDS among Haitians in the United States. Atlanta, Georgia: International Conference on AIDS, April 16, 1985. 8) Piot P, Quinn TC, Taelman H, et al. Acquired immunodeficiency syndrome in a heterosexual population in Zaire. Lancet 1984; 11: 65 -9. 9) Van de Perre P, Rouvroy D, Lepage P, et al. Acquired immunodeficiency syndrome in Rwanda. Lancet 1984; 11: 62 -5. 10)Kapita BM, Mann JM, Francis H, Ruti K, Quinn T, Curran JW. HTLV-III seroprevalence among hospital workers in Kinshasha, Zaire. Atlanta, Georgia: International Conference on AIDS. April 17, 1985. 11)CDC. Prevention of acquired immune deficiency syndrome (AIDS): report of inter-agency recommendations. MMWR 1983; 32: 101 -3. 12)CDC. Update: acquired immunodeficiency syndrome (AIDS)--United States. MMWR 1983; 32: 389 -91.
 Heterosexual Transmission of HIV infection in 475")
Incidence of HIV Infection (#/100 p. yrs) Heterosexual Transmission of HIV infection in 475 Discordant Couples Condoms STI in HIV - Spouse Deschamps MM et al. Ann Intern Med; 125: 324 -330, 1996.

Timeline of HIV Disease in Haiti Before ART: Most important OIs Pulmonary TB : most common pre-AIDS manifestation occurring in 40% of the cohort by 6 years Most common AIDS illness: wasting syndrome, candida esophagitis, coccidia diarrhea Leading causes of death : wasting syndrome, TB, crytococcal meningitis, toxoplasmosis Deschamps MM et al. AIDS. 2000, 14: 25152521

GHESKIO ART Outcomes at 1 year Of 1, 000 patients: l 90% survived despite: - Advanced HIV disease High rates of TB Severe malnutrition l 95% adherent - Severe P et al New Eng. J. Med 2005 353: 22 -2325 -2334

Clinical Trials Team Patrice Severe MD, Coordinator Clinical Trials Francine Noel, MD, Head Pediatrics Cynthia Riviere , MD Study Coordinator Paul Leger, MD, Liaison Clinical-Data Management Alexandra Apollon, MT Laboratory Mac. Arthur Charles MD, Ph. D, Laboratory

Outcome of HIV-infected children on ART At 24 months: • 81% alive; 9% deaths; 10% lost Predictors of mortality 1) Age < 18 months HR 2. 26 (1. 34 -3. 82); p<0. 01 2) CD 4 % < 5% HR 1. 78 (1. 38 -2. 83); p< 0. 001) 3) WAZ < -3 HR 2. 07 (1. 39 -3. 10); p< 0. 001) George E et al JID 2007

Mortality in HIV-infected children < 12 months old of PMTCT mothers Bactrim, formula HAART for Mothers with AIDS PCR/p-24 for early diagnosis and HAART in babies

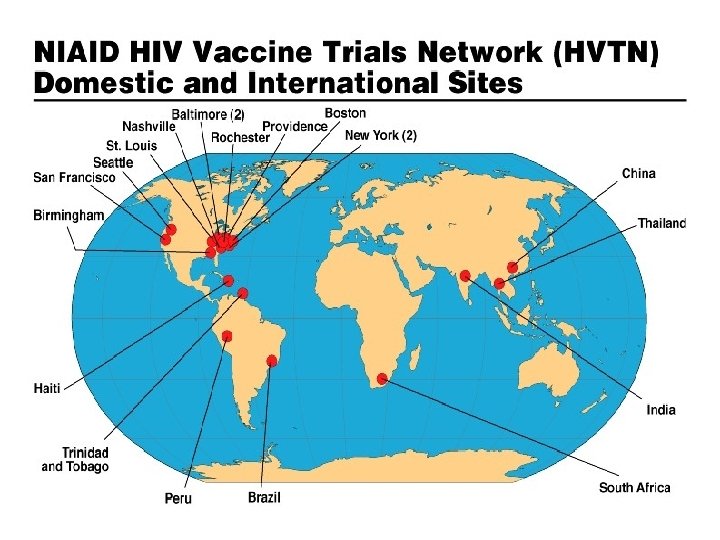
HIV Vaccine Trials in the Caribbean 903, 502 026, 050, 903, 502, 204 903, 050, 502 050, 903, 502 026

GHESKIO Ethics Publications l l l l l Pape JW. Ethics Review Committees: Consideration in Developing Countries. Emerging Infect Dis 2001; 7: 3. Fitzgerald DW, Marotte C, Verdier RI, Johnson WD Jr, Pape JW. Comprehension during informed consent in a less-developed country. Lancet 2002; 360: 1301 -2. Fitzgerald DW, Wasunna A, Crigger B, Pape JE. Building Ethics Capacity in Haiti. Developing World Bioethics 2003; 3: 3 -9 Fitzgerald DW, Wasunna A, Pape JW. Ten questions institutional review boards should ask when reviewing international clinical research protocols. IRB 2003; 25: 14 -8. Fitzgerald DW, Pape JW, Wasserheit JN, Counts GW, Corey L. Provision of treatment in HIV-1 vaccine trials in developing countries. Lancet 2003; 20; 362: 993 -4. Fitzgerald DW, Maxi A, Marcelin A, Johnson WD, Pape JW. Notification of positive HIV test results in Haiti: can we better intervene at this critical crossroads in the life of HIV-infected patients in a resource-poor country? AIDS Patient Care STDs 2004; 18: 658 -64. Desvieux JG, Malow RM, Jean-Gilles MM, Samuels DM, Deschamps MM, Ascencio M, Jean-Baptiste L, Pape JW. Reducing health disparities through culturally sensitive treatment for HIV+ adults in Haiti. The ABNF Journal 2004; 15(6)109 -15. Joseph, P, Schackman B, Horowitz R, Nerette S, Verdier RI, Henrys K, Wright P, Johnson WD, Pape JW, Fitzgerald DW, The use of an educational video during informed consent in an HIV clinical trial in Haiti. JAIDS 2006; 42; 5 -588 -591 Desvieux GD, Deschamps MM, Malow RM, Pape JW, Rosenberg R, Jean-Gilles MM, Saint Jean G, Metsch L. Barriers to care among HIV-positive Haitians : An examination of sociocultural factors; in HIV/AIDS Global Frontiers in Prevention Intervention (Pope C, White R, Malow R (eds) in press. Rose Irene Verdier, GHESKIO Daniel W Fitzgerald, Cornell

HIV Vaccine Trials Team Patrice Joseph, MD Coordinator Sandy Nerette, MD 502 Coordinator Conceptia Paul, RN 502 Nurse Marc Germain Ph. D Lab C Anne Beauharnais MD Biologist Maryse Thimolthee Msc, Micorbiology
 l HIVNET 026: March 2001 -April 2003")
HIV Vaccine Trials in Haiti (2001 -2008) l HIVNET 026: March 2001 -April 2003 – – – l 3 sites involved: Brazil, Haiti, Trinidad. Total Haiti: 40; Study status: completed Outcome: 100% retention rate; HVTN 050: April 2004 -2009 – – Total volunteers 435; Total Haiti: 35 low-risk participants Total Haiti: 35 enrolled; Study status: completed enrolment 100% retention rate; l HVTN 502: August 2005 -2010 – – – l Phase II-B MRK Ad-5/gag/pol/nef from MERCK & Co Total volunteers : 3, 000; Total Haiti: 440 high-risk participants Total Haiti : 326 enrolled; Study status: enrolment completed ; 100% retention; HVTN 204: Phase I/II VRC ADN clade B gag/pol/nef + clade A, B, C env and VRC r. Ad 5 clade B gag/pol fusion + clade A, B, C env from Vaccine Research Center & Co: Phase I/II – Total Haiti: 12 low-risk participants; Study status: enrolment completed –
 – 5175 : phase III,")
GHESKIO Clinical Trials l Adult Clinical trial Group (ACTG) – 5175 : phase III, randomized, open-label, three-arm study of ART efficacy comparing once daily PI vs. NNRTI-containing regimen vs. standard twicedaily ARV for the initial RX of HIV-1 infection; status: 100/100 enrolled – 5207: Randomized Comparison of Effects of Single-Dose NVP vs. Single- Dose NVP + ZDV/3 TC vs. Single Dose NVP + ZDV/ Tenofovir on the Emergence and Transmission of Drug Resistant Viruses in HIV+ mothers and their babies: status: 4/40 enrolled – 5190: Safety and toxicity among infants born to HIV+ women enrolled in HAART: not activated l Comprehensive International Program of Research on AIDS (CIPRA): Open-label clinical trial to determine whether “early” initiation of ART in HIV+ adults (actual US vs. UNAIDS guidelines) in HIV+ adults will improve survival at 36 months; status : 816/816 enrolled l PK study: effect of tropical AIDS diarrhea on absorption of ARV; status: 50/50 enrolled

Cornell-GHESKIO VCT model with integrated services STI Management Post-HIV exposure Counseling and HAART Pre-test Counseling HIV, Syphilis, Tuberculosis Post-Test Counseling Reproductive Health Services (family planning and prenatal care) HIV+ women Prevention HIV MTCT with HAART Rx = Treatment Px = Prophylaxis Peck R, Fitzgerald D, Liautaud B et al: JAIDS: 33; 470 -475, 2003 Same day TB screening / Rx / Px Care to HIV infected individual / affected family · OI Rx/Px · HAART for AIDS or CD 4 count 200 · Nutritional support · Psychosocial support

GHESKIO Training Daphnee Benoit MD Training Director Claudia Riche RN MPH
 l 1986: First case of HIV in Central")
Partners in Health (Zanmi La Santé) l 1986: First case of HIV in Central Plateau l 1988: Free serologic testing to diagnose HIV l 1990: Intensified prevention efforts hampered by l 1995: development of comprehensive care program political violence and resulting migration, gender inequality, and poverty – AZT to pregnant women in order to block mother-to-child transmission l 2001: First to offer ART

“I was a walking skeleton before I began therapy. I was afraid to go out of my house and no one would buy things from my shop. But now I am fine again… My wife has returned to me and now my children are not ashamed to be seen with me. I can work again. ”

PIH Publications on HIV/AIDS in Haiti Patient Care Community Health workers Farmer et al. Community-based approaches to HIV treatment in resource-poor settings. Lancet. 2001; 358(9279): 404 -409. Louis C et al Late presentation for HIV care in central Haiti: factors limiting access to care. AIDS Care. 2007; 19(4): 487 -491. Walton DA, et al Integrated HIV prevention and care strengthens primary health care: lessons from rural Haiti. JPub. Health. Pol 2004; 25(2): 137 -158. Behforouz HL, et al From directly observed therapy to accompagnateurs: enhancing AIDS treatment outcomes in Haiti and in Boston. CID 2004; 38(Suppl 5): S 429 -436. Mukherjee JS et al Community health workers as a cornerstone for integrating HIV and primary healthcare. AIDS Care. 2007; 19 Suppl 1: 73 -82. Partners In Health; Program in Infectious Disease and Social Change, Harvard Medical School; Division of Social Medicine and Health Inequalities, Brigham and Women's Hospital; Francois-Xavier Bagnoud Center for Health and Human Rights, Havard School of Public Health. The PIH Guide to the Community-Based Treatment of HIV in Resource-Poor Settings. Revised second edition. Boston: Partners In Health; 2008. Mukherjee JS. HIV-1 care in resource-poor settings: a view from Haiti. Lancet. 2003; 362: 994 -995. Koenig SP et al Monitoring HIV treatment in developing countries. BMJ 2006; 332(7541): 602 -604. Mukherjee JS, et al Antiretroviral therapy in resource-poor settings: decreasing barriers to access and promoting adherence. JAIDS 2006; 43 Suppl 1: S 123 -S 126. Koenig SPet al Scaling-up HIV treatment programmes in resource-limited settings: the rural Haiti experience. AIDS. 2004; (18 Suppl 3): S 21 -25. Fraser HSFet al An information system and medical record to support HIV treatment in rural Haiti. BMJ 2004; 329(7454): 1142 -1146. Farmer P et al Community-based treatment of advanced HIV disease: Introducing DOT-HAART (directly observed therapy with highly active antiretroviral therapy). Bull. WHO. 2001; 79(12): 1145 -1151. Socio economic factors, stigma Farmer PE. Haiti's lost years: Lessons for the Americas. Current Issues in Public Health. 1996; 2(3): 143 -151. Farmer PE. AIDS-talk and the constitution of cultural models. Social Science and Medicine. 1994; 38(6): 801 -809. Farmer PE. Sending sickness: Sorcery, politics, and changing concepts of AIDS in rural Haiti. Medical Anthropology Quarterly. 1990; 4(1): 6 -27. Farmer PE. The exotic and the mundane: Human Immunodeficiency Virus in Haiti. Human Nature. 1990; 1(4): 415 -446. Mukherjee JS. Structural violence, poverty and the AIDS pandemic. Development. 2007: 15(1): 115 -121. Smith Fawzi MC, et al Factors associated with forced sex among women in rural Haiti: implications for the prevention of HIV and other STDs. Social Science and Medicine. 2005; 60(4): 679 -689. Castro A, Farmer P. The impact of comprehensive HIV/AIDS care on stigma and testing: learnings and experiences from Haiti. Exchange on HIV/AIDS, Sexuality and Gender. 2005; 1(1): 30 -31. Castro A, Farmer P. Understanding and addressing AIDS-related stigma: from anthropological theory to clinical practice in Haiti. AJPH 2005; 95(1): 53 -59. Kim JY, Farmer P. AIDS in 2006 -Moving toward one world, one hope? NEJM. 2006; 355(7): 645 -647. Farmer P. Political violence and public health in Haiti. NEJM 2004; 350(15): 1483 -1486. Farmer PE, Kleinman A. AIDS as human suffering. Dædalus. 1989; 118(2): 353 -378. Farmer PE. Bad blood, spoiled milk: Body fluids as moral barometers in rural Haiti. American Ethnologist. 1988; 15(1): 62 -83. Farmer PE. Blood, sweat, and baseballs: Haiti in the West Atlantic system. Dialectical Anthropology. 1988; 13(1): 83 -99. STIs Smith Fawzi MC, Lambert W, Singler J, Léandre F, Nevil P, Bertrand D, Claude MS, Bertrand J, Louissaint M, Jeannis L, Cook EF, Salazar JJ, Farmer P, Mukherjee JS. Identification of chlamydia and gonorrhea among women in rural Haiti: maximizing access to treatment in a resource-poor setting. STI. 2006; 82(2): 175 -181. Smith Fawzi MC, Lambert W, Singler JM, Koenig SP, Léandre F, Nevil P, Bertrand D, Claude MS, Bertrand J, Salazar JJ, Louissaint M, Joanis L, Farmer PE. Prevalence and risk factors of STDs in rural Haiti: implications for policy and programming in resource-poor settings. Int. J STD&AIDS. 2003; 14(12): 848 -853.

Haiti: 2008 Training l MPH program created with Quisqueya Uni. l CHART training centers (PIH, GHESKIO) Services: l. VCT sites: l. Persons tested for HIV : l. Patients receiving AIDS therapy: 140 332, 840 15, 492 HIV Counseling, Testing and Treatment Sites DR Research: l. National AIDS surveys – prevalence decreased from 6. 2% (1993) to 2. 2% (2005) l Collaborative nutrition research with College of Human Ecology l. National survey for drug resistant tuberculosis and treatment plan for MDRTB patients l. TCHARI

Remaining Challenges for Haiti and the Caribbean Continue to participate in defining the international vaccine and microbicides research agenda l Therapy: – Timing of HAART: Enrolment of 816 patients in GHESKIO study completed – Interventions to decrease the high early mortality l l TB – Co treatment of HIV and TB – MDRTB, XDRTB Implementation science: How to scale-up from models to implementation with limited capacity in lab and human resources? Ø How to share the research agenda with the entire Caribbean? TCHARI is the conduit l

25 years of research on HIV/AIDS in Haiti l 1982: First recognition of AIDS in developing world with creation of comprehensive research, service, and training program l 1983: NIH/Fogarty supported research/ training with capacity building for creation of integrated model of prevention/care l 2003: large scale training and extension of services nationwide with GFATM and PEPFAR. l National HIV seroprevalence decreased by 50% in last decade l Research projects can have national impact even under difficult conditions: These accomplishments were the result of: – synergisms between research, training and clinical care. – Strong public private collaboration l Share the research capacity with the Caribbean through TCHARI

The Medical Research Foundation and Treatment Centre

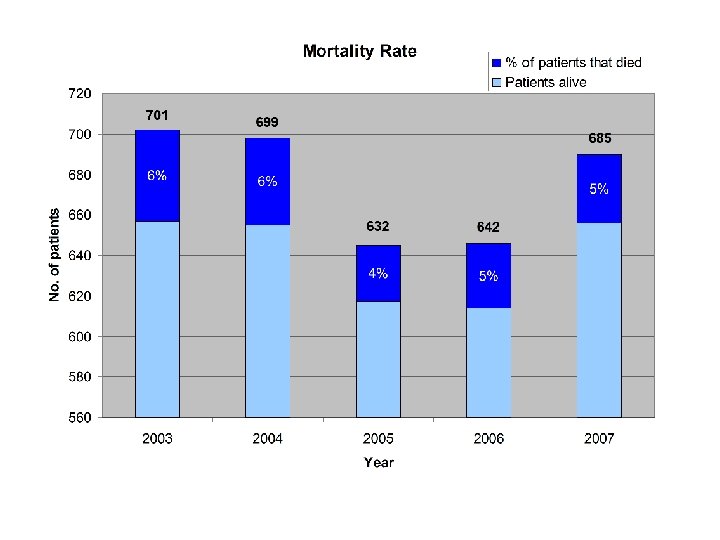
 TOTAL")
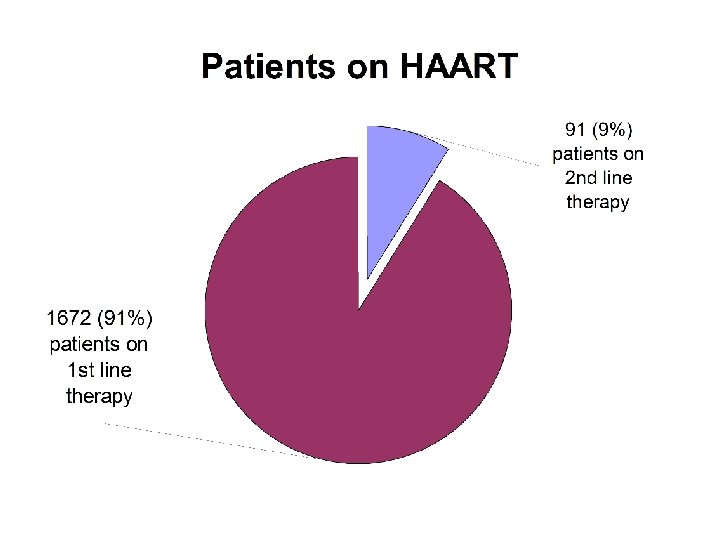
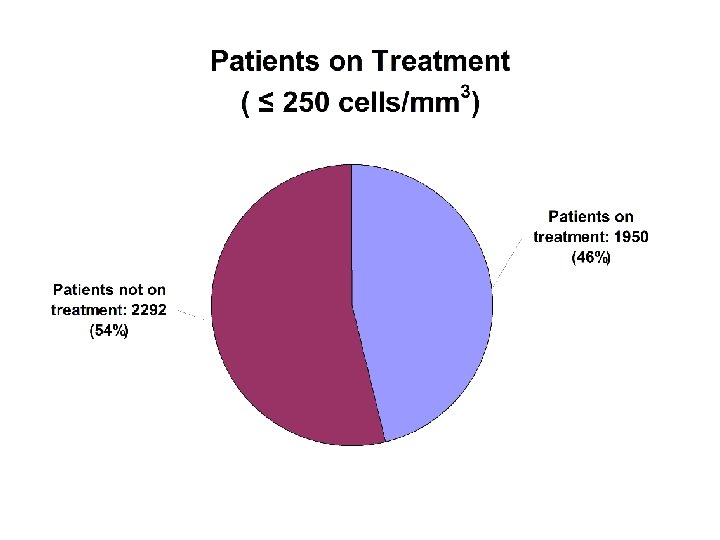
Medical Research Centre HIV/AIDS TREATMENT PROGRAMME (22 APRIL 2002 – 25 JULY 2008) TOTAL PATIENTS 4328 TREATMENT (CD 4 CELLS <250/cmm³) NO. PATIENTS ON TREATMENT 2206
 Cryptococcus neoformans Histoplasmosis capsulatum")
Most Common Ols Candida spp Toxoplasma gondii (gp. 54%. 1954) Cryptococcus neoformans Histoplasmosis capsulatum (gp. 61%. 1962) (Lancet, 1, 103, 1984 Pneumocystis carinii Mycobacterium tuberculosis Rare Ols Kaposi’s sarcoma Lymphoma M. Avium complex (MAC) infections
 Number of HIV/AIDS patients Number of HIV/TB patients 3843 265")
HIV/TB Coinfections (2002 -2007) Number of HIV/AIDS patients Number of HIV/TB patients 3843 265 (7. 7 %)
 in General population (Trinidad & Tobago) Total No.")
Hepatitis B surface antigenemia (HBs. Ag) in General population (Trinidad & Tobago) Total No. Tested (4454) HBs. Ag positive — 34 (0. 7%) Males 28 (82%) Hepatitis B surface antigenemia (HBs. Ag) in HIV-1 patients Total No. Tested (2293) HBs. Ag positive — 164 (7. 2%) Male/Female 106/58 HBe. Ag positive — 45 (27. 4%)
 <")
HTLV-1 seropositivity in 2042 HIV/AIDS patients Total # Coinfected = 128 (6. 2%) < 40 years > 40 years Total Male 10 ( 7. 8%) 45 (35. 2%) 55 (43%) Female 30 (23. 4%) 43 (33. 6%) 73 (57%) Total 40 (31%) 88 (69%) 128 (100%)

A subset of long-term non-progressors have recently been described. These patients are characterized by stable CD 4+ T-cell count, HIV-1 positivity confirmed by Western blot and < 50 copies of viral RNA/ml in the absence of antiretroviral therapy. These have been called “elite suppressors” (Migueles et al, 2003).

Between 1993 and 2007, of 794 HIVinfected individuals in Trinidad tested for HLA alleles, 58 (7%) were HLA B*57 positive. In a study of 11 elite suppressors, 9 (82%) were HLA B*57 positive. The intervals between the first diagnosis of HIV-1 and the discovery of their “elite suppressor” status ranged from 3 -10 years in 7 patients and < 3 years in four.

STAFF OF THE MRC 4 DOCTORS 3 LABORATORY TECHNICIANS 3 NURSES 2 SECRETARIES 1 NURSE COUNSELOR 1 DATA ENTRY CLERK 1 ADHERENCE NURSE 1 RECEPTIONIST 1 NURSE SOCIAL WORKER 1 DRIVER/CONTACT TRACER 2 PHARMACISTS 1 USHER/SECURITY GUARD 1 PHLEBOTOMIST




Developing collaborative relationships: perspective of a non-Caribbean investigator Susan Buchbinder, MD Director, HIV Research Section San Francisco Department of Public Health University of California, San Francisco

Overview • Collaborations: a personal story • How to form collaborations • Benefits in working collaboratively • Challenges and pitfalls with collaborations
… • The HVTN planned to conduct an efficacy trial of")
My beginnings (around 2000)… • The HVTN planned to conduct an efficacy trial of two experimental HIV vaccines – Canarypox vaccine with or without – Gp 120 subunit vaccine • Needed > 11, 000 study volunteers in areas where clade B virus common – Separate estimates of efficacy for men (MSM) and women

Capacity estimates to enroll HVTN 501 2000 MSM Heterosexuals US sites 56% 12% International sites 29% 9% Total 85% 21%

Next steps • The trial we had planned did not go forward, but data on other vaccines suggested they might generate stronger immune responses • Still needed to build additional capacity to test vaccines; possibility of 2 smaller efficacy trials, same total capacity need • How to build new partnerships?

Epidemiology of clade B epidemic • Severe epidemic in MSM throughout the Americas – Infection rates 2 -5% per year despite “best” risk-reduction counseling at sites in US, Canada, Peru, Brazil – “Generalized” epidemic in subpopulation of MSM in Americas similar to rates in heterosexuals in Africa • AIDS cases slowly increasing in women – Best investigators have been unable to find populations with seroincidence > 1. 2/100 py in US – Exceptions: Caribbean, Central America

Partnerships • Began by researching epidemiology to determine geography • Followed by looking for potential colleagues to work with • Lots of requirements, infrastructure building, but 3 essential components: – True partnership with strong investigators – Connections with local, at-risk communities – Political support for research

HVTN 2008

Choosing collaborators • Communication, communication • Reaching out through networks of contacts • Finding expertise that matches your needs • Listening for what is said (not what you want to hear)

What do non-Caribbean investigators bring to the collaboration? • Experience that should complement yours • Additional connections – Network of researchers – Funding, resources – Exchange of ideas, training in areas of expertise • Insight into new locations, new epidemics, new approaches

What should be avoided in collaborations? • Non-collaboration – One-way relationships – Scientific, ethical, regulatory imperialism – Unwillingness to engage with all 3 elements (investigators, community, political/regulatory leaders) • Mis-match between expectations – – Time Goals Money Duration • Lack of personal connection

Skills-Building Workshop XVII International AIDS Conference Carmen D. Zorrilla, MD Professor OB-GYN UPR School of Medicine carmen. zorrilla@upr. edu

Only one thing defines an impossible dream: the fear of failure. Paulo Coelho The Alchemist

WHO ARE WE? • The Trans-Caribbean HIV/AIDS Research Initiative is an independent, inclusive, diverse, trans-disciplinary, multicultural group of Caribbean-based HIV/AIDS researchers. • Through partnering, networking, and collaborative activities, TCHARI strives to become a catalyst for social change in support of the enhanced public health of the Caribbean.

• Jean William Pape, M. D. - Chairman • Brendan Bain, M. D. - Founding Member • Courtenay Bartholomew, M. D. - Founding Member • Antonio De Moya, M. P. H. - Founding Member • Yasuhiro Yamamura, Ph. D - Founding Member • Carmen Zorrilla, M. D. - Founding Member

WHAT ARE OUR OBJECTIVES? • To contribute to defining a Caribbean HIV/AIDS research agenda • To facilitate, promote, and foster collaboration among Caribbean HIV/AIDS researchers, including the training and mentoring of new investigators • To disseminate research protocols and findings within the Caribbean region internationally • To develop a Caribbean HIV/AIDS Research Information Repository

WHAT ARE OUR ANTICIPATED OUTCOMES? • Development of culturally sensitive research training programs and research protocols • Development of molecular diagnosis programs in support of uniform clinical data collection • Development of programs for the clinical management of HIV/AIDS patients • Development of models of HIV/AIDS care across all Caribbean nations

Caribbean HIV Epidemic Research Needs • Better understanding of the nature of the epidemic in the Caribbean, particularly at the molecular level, and the pattern of HIV-associated infections such as human papillomavirus (HPV) and multi-drugresistant tuberculosis (MDR-TB); • Development of therapeutic approaches to effectively treat HIV and associated infections among HIV-infected people in the region; • Development and testing of vaccines to prevent infection with HIV; • Better understanding of the nature and context of risk behaviors and development of prevention interventions to address them; and • Development and implementation of strategies to prevent transmission of HIV from mother to child

This research agenda for the Caribbean represents the output of two technical meetings of the TCHARI Working Groups comprising approximately fifty (50) junior and senior Caribbean HIV/AIDS researchers and scientists. The 3 working groups and 2 sub-groups are: • • Therapeutic and Epidemiology Group Molecular Epidemiology Subgroup Vaccine Group Behavioral, Social Sciences, and Prevention Research Group • HIV Prevention Research—PMTCT Subgroup

The objectives of the Thematic Working Groups are: • To develop collaborative HIV/AIDS research methodology for the Caribbean • To develop a Caribbean HIV/AIDS research agenda • To discuss and agree on ongoing research protocols • To advance new ideas and research protocols of interest • To provide mentoring/training for early- to mid-career researchers/scientists

Therapeutics and Epidemiology Group • • • Jean William Pape, Chair Courtenay Bartholomew Gregory Boyce Juan Burgo-Soto Patrick Hochedez Serena Koenig Claudia Valdez Marie-Therese Sow Sharon Soyer-Labastide Gisselle Vasquez Molecular Epidemiology Subgroup • • • Yasuhiro Yamamura, Chair Georges Dos Santos George Hillyer Carole Anne Beauharnais Monica Smikle Marisol de Castro Jhoanne Munoz Angélica Lebreault Akinola Abayomi Frank Mejia

Vaccines Group • • Carmen D. Zorrilla, Chair Patrice Joseph Yeycy Donastorg Lydia E. Santiago Luis Rodríguez George Hillyer Peter Figueroa Behavioral, Social Sciences and Prevention Research Group • Brendan Bain, Chair • Antonio de Moya • Silkha Abreu • Althea Bailey • Frank Caceres • Judit de la Rosa • Lisa Norman • Julio Jimenez • Nanet Lopez • Marija Miric • Vanessa Suir • Peter Weller

HIV Prevention and Research–PMTCT Subgroup • Marie-Marcelle Deschamps, Chair • Celia Christie-Samuels • Eddy Perez-Then • Irma Febo • Avion Quava-Jones • Carmen D. Zorrilla

The search always starts with beginner’s luck and ends with the Conqueror’s test. Paulo Coelho The Alchemist

Vaccine Group Potential Collaborative Research Opportunities 1. Ethical issues, recruitment, consent, and retention challenges in the Caribbean Region as compared with U. S. sites recruiting Caribbean volunteers for clinical trials 2. Qualitative study to evaluate the impact of the negative results of the STEP trial on the volunteers, community and staff in the Caribbean Region 3. Laboratory abnormalities among volunteers for the HVTN 050/Merck 018 Phase 1 vaccine study in the Caribbean Region

Therapeutics and Epidemiology Group Potential Collaborative Research Opportunities Focusing on research related to antiretroviral therapy (ART) in the Caribbean region. ▪ ART treatment outcomes study at 1 year ▪ ART costing study ▪ ART cost analysis study

Therapeutics and Epidemiology Group Additional studies suggested • Early Mortality: Many patients still present late with advanced HIV/AIDS, resulting in high mortality during the first 3 to 6 months of care. Data from Haiti and Trinidad & Tobago demonstrate this phenomenon, even though care is free. • Adherence is a problem among all patients, but particularly among adolescents. Studies have shown that adherence is the strongest predictor of long-term clinical outcome. • HIV/TB and MDR-TB: TB remains the most common opportunistic infection, and a major cause of death.

Molecular Epidemiology Subgroup Potential Collaborative Research Opportunities ▪ Unexplainable weight loss during the initial 12 months of antiretroviral (ARV) treatment as a predictor of treatment failure and emergence of drug resistance. ▪ HPV genotype distribution and infection with multiple HPV genotypes among HIV sero-positive and sero-negative women. ▪ Multi-drug-resistant TB in HIV-infected patients. ▪ Genetic and immunologic shifting of HIV in the Caribbean, for possible submission to the National Institutes of Health (NIH) as an R-01 proposal.

Behavioral, Social Sciences, and Prevention Research Group Potential Collaborative Research Opportunities • A review of approaches to studies of knowledge, attitudes, perception, and behavior (KAPB) related to HIV/AIDS in the multicultural Caribbean. • A correlational study of stigma and discrimination related to HIV/AIDS and general social prejudices.

Behavioral, Social Sciences, and Prevention Research Group Additional Studies Suggested • Individual, social, and structural barriers and facilitators to acceptance of HIV testing in multiple Caribbean countries. Adherence to antiretroviral (ARV) treatment in Caribbean contexts, particularly in adolescents. Gender and power issues influencing the epidemic. Risk, vulnerability, and resilience in relation to the HIV epidemic, with specific individuals and groups to be determined. Innovative, culturally appropriate communication strategies to improve primary prevention. HIV service provider behavior: • • • ▪ Improving efficacy in delivery of services, ▪ Communication strategies that enhance prevention and care, and ▪ Psychosocial factors that intervene in the provision of HIV prevention, care, and treatment.

HIV Prevention Research–PMTCT Subgroup Potential Collaborative Research Opportunities • Strategies to decrease mother-to-child transmission of HIV. • Outcomes of infants born to HIV-positive mothers in the Caribbean.

TCHARI’s 2007 Achievements • Identification of 10 -proposed studies in the 5 -thematic program areas to inform the Caribbean HIV/AIDS research agenda; • Development of the Database Repository and Website; • Collective agreement to conduct collaborative studies; • Development of 2 -protocols for studies approved by collaborative sites; • Development of models of HIV care that are all strategically aligned with the core mandate of TCHARI.

Limitations of Research in the Caribbean • Ms. Caroline Allen, the Health Research Scientist at the Caribbean Health Research Council (CHRC) has just co – authored a literature review on the “Social and Cultural Factors driving the HIV epidemic in the Caribbean: a literature review. ” The document can be found on the CHRC website http: //www. chrc-caribbean. org • Only a few studies undertaken in the region are documented in peerreviewed journals. • Most of the unpublished studies can be found in the reports of the various development or funding agencies that work in the region. • Not many longitudinal research studies have been conducted in the region that can identify factors that lead to change in outcomes.

Limitations of Research in the Caribbean • Many countries do have functioning National Ethical Review Boards with standardized protocols for approval. Some feel that Regional Ethics Review process needs to be established to ensure equity. • Not many people in the field are qualified to be Principal Investigators. Young people therefore need to be mentored in the HIV research field. • More rigorous research methods need to be applied to some of the studies that are designed and implemented so the results can be used to provide evidence base policy decisions.

Limitations of Research in the Caribbean • Need for an information data base, for a repository of projects, investigators and findings • Need for a repository of publications with easy access to all interested in carrying out research projects in the Caribbean • Need to foster more collaborative multi-national studies in the region • Need to involve the Community as partners

• TCHARI can facilitate the development of an inventory of research projects and post the results in our website • We can facilitate the dissemination of published reports and abstracts presented at the diverse meetings • We need to start considering the idea of a Caribbean Ethics Committee • Mentoring junior investigators will assure the availability of a well-trained cadre of investigators for the region and for the world

Acknowledgements These individuals contributed to the preparation of the workshop and the information presented: • Stewart Smith • Linda Reck • Nicola Taylor • Prof. Karl Theodore TCHARI recognizes its supporter: The Office of AIDS Research, NIH (OAR) and its liaison Ms. Linda Jackson

Measure time, if you must, in lessons learned, not in minutes or hours or years. Brian Weiss Only Love is Real

Trans-Caribbean HIV/AIDS Research Initiative A multicultural Caribbean united against HIV/AIDS “The Trans-Caribbean HIV/AIDS Research Initiative: Building Cross. Cultural, Trans-National, Multidisciplinary Research Collaborations” The context for conducting HIV/AIDS research in the Caribbean: cultural competency Lydia E. Santiago, Ph. D. Medical Sciences Campus University of Puerto Rico

Introduction ▪ Identify cultural competency issues that must be considered when conducting regional research ▪ Highlight cross-cultural issues ▪ We will not offer solutions to as-yet unsolved issues

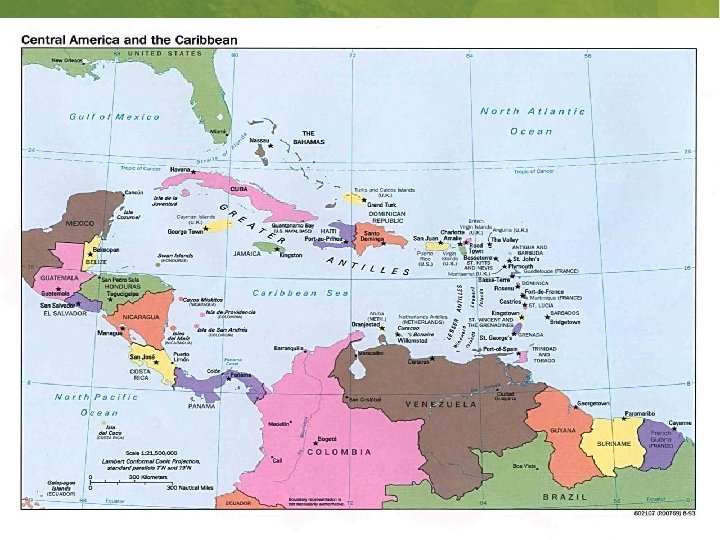
Caribbean Region

Heterogeneity of the Caribbean Region § National identity (Guyanese, Cuban, Haitian, Puerto Rican etc. ) § Religion (Catholicism, Hinduism, Santería, Espiritismo, etc. ) § Language (Patois, Creole, Papiementu, Hindi, French, Spanish, English, etc. ) § Ethnic origin (Chinese, Indian, African, Lebanese, Dutch, Hispanic etc. )

“How should we understand a commitment to equality in a world of multiple human differences, grim hierarchies of power, and cruel division of life circumstance? ” Okin, SM, 1999

Why is it important to develop cultural competent HIV researches for the Caribbean? § Our academic training has instilled in us an idea of a homogeneous and ethnocentric culture; which makes us think that our own culture or cultural group is inherently superior to other cultures or cultural groups. § This “superiority” frequently has been expressed through oppressive relationships between groups with more power and those most vulnerable in society. § Next generation of HIV researchers needs to understand value the richness of cultural diversity. Santiago & Rosa Soberal, 2007

Why is important to develop cultural competent HIV Researches for the Caribbean? § Uni-cultural perspective assumes that concepts, (and explanations of relationships between concepts), are universally applicable across different cultures. § Without cultural competent health researchers tend to impose their beliefs, values, and behavior patterns upon other cultures. § This perspective leads to invalid research data. Porter and Villaruel, 1993; Linenger, 1995; Papadopoulos, 2002

What is cultural competency? § The ability to appreciate and use the knowledge of a culture to understand a situation or try to find a solution to a problem. § It includes the recognition of personal attitudes, the acquisition of relevant knowledge and the development of skills, which facilitate working effectively among those who are different. Walters et al. 1994; Zambrana et al. 2004; Winkelman et al. 2005; Betancourt et al. 2006.

Cultural issues § Race and Ethnicity § Gender § Caribbean Sexuality § Poverty and Structural Violence

Cultural issue : race/ethnicity § In North America, discussions on cultural competence have primarily centralized around issues traditionally associated with race, gender, ethnicity and language. § In Latin America, there is a continuum of racial categories and often only people who look quite African in appearance will be identified as such. Wade, 1997; Smedly 1999; Leavitt, 2002; Winkelman, 2005;

Cultural issue : race/ethnicity § In North America, the category “black” includes anyone with a known “drop of black blood”; thus someone known to have a black grandmother will be assigned a black identity. § Other important issue related with race is the controversy about race as biology construct. Many biologists, geneticists and physical anthropologists have reach the conclusion that biologically speaking, races do not exist. § While the biological basis for races has never been scientifically established; legal, social, administrative and political concepts of races have been widely utilized

Cultural issue : race/ethnicity § The ideology of racism exists and has very serious consequences. § Kempadoo affirms that race has been constructed as real in the Caribbean life. Oppressions, discrimination and social inequities based on phenotype and cultural origins are still found within the region. Hierarchies marked by skin color, hair, body type and facial features remain in place, with terms such as indio, mulato, trigueño which are commonly used across several languages. Kempadoo K. (2004).

Cultural issue : race/ethnicity § Ethnicity has become an alternative conceptual framework for race § Ethnic identification is classified by common traits or customs; and it is based on a person’s self-identification as belonging to a particular group that shares a cultural heritage. Wade, 1997; Smely 1999; Leavitt, 2002; Winkelman 205;

Cultural issue : Sexuality § To many, the Caribbean continues to be an unruly and promiscuous place. Kamala Kempadoo asserts that the Caribbean has been portrayed in the global imagination as an exotic region of the world. § She also points out that the Western ideal of monogamous, patriarchal, heterosexual arrangement is been questioned by the diversity of Caribbean sexuality, in which multiple partnering relationships by both men and women exist. § Kempadoo proposes that we need a different lens for thinking about Caribbean sexuality. Kamala Kempadoo (2004)

Cultural issue : Gender • In the Caribbean region, as in most part of the world, women are confronted with sexism (the ideology that situate women as inferior of men). During the last 20 years we have work hard to empower women as a preventive strategy for HIV protection. • Sex workers have been mentioned as one of the principle HIV “risk group” in the Caribbean region. In Surinam, Dominican Republic and Guyana female sex workers have established projects for their own empowerment. • Now, we have to do more research to learn how non sex worker women are dealing with the sexual negotiation in the Caribbean region.

Cultural issue : Poverty and Structural Violence § Paul Farmer has shown us that AIDS in the Caribbean region is deeply embedded in social and economic structure; and that violence, poverty, and inequality are the fault lines along which HIV spreads. § What do we know about the nature of the Caribbean pandemic? Farmer, 1993; Farmer, 1999; Farmer, 2003

Cultural issue : Poverty and Structural Violence § Farmer states that the Caribbean region needs programs designed to remedy the inequalities around access to services. § These can help people to live free and to have healthy lives § The challenge for the new Caribbean HIV researchers is: How to build a research agenda for action that moves beyond good scientific analysis? Farmer, 1993; Farmer, 1999; Farmer, 2003

Conclusions ▪ We not offer solutions to as-yet unsolved issues ▪ But we need to begin to talk about the development of an appropriate Cultural Competence Model for the Caribbean Region.

Gracias, Thanks, Merci, धनयव द ,
. Cultural Competency: Providing Quality Care to Diverse Populations. Consult")
References • Betancourt JR. (2006). Cultural Competency: Providing Quality Care to Diverse Populations. Consult Pharm 21(12): 998 -95. • Essed F. (1996). Diversity- gender, color & culture. Amherst: University of Massachusetts Press. • Farmer P (1992/2006). AIDS & Accusation- Haiti and the geography of blame. Berkely: University of California Press. • Farmer P. (1999). Infections and Inequalities-the modern plagues. Berkeley: University of California Press. • Farmer P. (2003). Pathologies of Power-health, human rights, and the new war on the poor. Berkely: University of California Press. • Goode TD, Sockalingam S. (2000). Home Health Care Manage Prac. (2000). 12(5): 49 -55. • Kempadoo K. (2004). Sexing the Caribbean- Gender, Race, and Sexual Labor. New York : Routledge. • Leavitt, RL. (2002). CEU: Developing cultural competence in a multicultural world. Alexandria. 10: 36 -48. • Louis C; Ivers LC; Smith Fawzi MC; Freedberg KA; Castro A (2007). Late presentation for HIV care in central Haiti: factors limiting access to care. AIDS Care 19(4): 487 -491.
 (1999). Is Multiculturalism Bad for Women? New Jersey: Princeton")
References • Okin SM (ed) (1999). Is Multiculturalism Bad for Women? New Jersey: Princeton University Press. • Leninger MM. (1995). Transcultural Nursing: Concepts, Theories, Research and Practices. New York: Mc. Grow-Hill. • Papadopoulos I. (2002). Journal of Advanced Nursing. 37(3): 258 -264. • Spector, RE. (2000). Cultural Diversity in Health & Illness. New Jersey: Prentice Hall Health. • Porter C & Villaruel A. (1993). Nursing research with African-American and Hispanic people: guidelines for action. Nursing Outlook. 42: 59 -67. • Priddy FH; Cheng AC; Salazar, LF; Frew PM. ((2006). Racial and ethnic differences in knowledge and willingness to participate in HIV vaccine trials in an urban population in th Southeastern US. International Journal of STD & AIDS. 17: 99 -102. • Santiago LE & Rosalie Soberal R (2007). Elementos de la diversidad. In Rosa Soberal R (ed). La diversidad cultural: Reflexión Crítica desde un acercamiento Interdisciplinario. • Smedly, A, (1999). Race in North America-origin and evolution of a Worldview. Boulder, Colorado: Westview.
 Cultural Competency: from Philosophy to Research and Practice. Journal")
References • Sue S. (2006) Cultural Competency: from Philosophy to Research and Practice. Journal of Community Psychology. 34(2), 237 -245. • Thompson, SJ. The social and cultural context of risk and prevention: food and physical activity in an Urban Aboriginal community. Health Education & Behavior. 27: 725 -743. • Wade P. (1997). Race and Ethnicity in Latin America. Sterling, Virginia: Pluto Press. • Walters, JL, Canaday, R. Stein, T. (1994). Evaluating Multicultural Approaches in HIV/AIDS Educational Material. AIDS Education and Prevention. 6(5): 446 -453. • Winkelman M. (2005). Cultural Awareness Sensitivity & Competence. Iowa: eddie bowers publishing. • Zambrana RE; Molnar C; Baras Muñoz H; Salas Lopez, D. (2004). Cultural Competency as It Intersects With Racial/Ethnic, Linguistic, and Class Disparities in Managed Healthcare Organizations. The American Journal of Managed Care. 10 sp 37 -sp 44.

Trans-Caribbean HIV/AIDS Research Initiative A multicultural Caribbean united against HIV/AIDS The context of conducting HIV/AIDS Research in the Caribbean: Relevant ethical issues Patrice Joseph, MD, MSCI August 5, 2008

Outline • Ethical issues specific to the Caribbean region • How ethical issues relative to one study or country can impact the region • Informed consent process at GHESKIO: “A model for appropriate counseling and evaluation of volunteers knowledge and real desire to participate” • Futures directions

Existing Research Collaboration within the Caribbean countries • HIV Vaccine trials : – HIV vaccine Trials: • HIVNET 026: Haiti, Trinidad • HVTN 050: Haiti, DR, PR • High–risk Population for phase III: HVTN 903: Haiti, DR, PR • HVTN 502: Haiti, DR, PR, Jamaica • HVTN 204: Haiti, Jamaica • Therapy – (HAART): Haiti( GHESKIO, PIH), DR, Puerto Rico, Barbados, Jamaica, Martinique, Guadeloupe – AACTG: Haiti, PR (Non TCHARI site) – Surveillance of ART resistance: PR, Haiti, Martinique • Press Education (Fogarty): – Year 1 Haiti; Year 2: DR, T/T, and other Caribbean countries • Hepatitis C: Haiti, Martinique • TB: MDR-TB prevalence study: DR, Haiti

Potentials areas for Research Collaboration within the Caribbean countries • Therapy – ART outcome in the Caribbean – Cost of ART in the Caribbean • High risk cohort of CSWs: Haiti, DR, PR • IRB clearance

How do we protect subjects participating in research? • • • Nuremberg Code, 1949 ▪ Voluntary consent of the human subject is absolutely essential ▪ Subject well-being is more important than “Science ▪ Respect for Persons Declaration of Helsinki, 1964 Belmont Report, 1979 1. 2. 3. 4. • Adequate information provided Comprehension: understanding the information Voluntary choice to participate Privacy and confidentiality ▪ Beneficence ▪ Justice U. S. Code of Federal Regulations, 1981 ▪ Ethics committee approval required ▪ Added many protections for human subjects ▪ Additional requirements and safeguards

Ethical Concerns in the Caribbean l Inform Consent Process and Ethic Committee approval: l Are adequate information provided to subjects? l How to enhance understanding/comprehension of the information by study subjects? l How best ensure voluntary choice to participate l Are subjects involved in research studies Guinea-pigs? l How best to maintain privacy and confidentiality l Ethical clearance: l Existing IRB or Credible Local IRB/ethical committees l Communication between local IRB and foreign IRBs
 May 2,")
at the Haitian Study Group on Opportunistic Infections and Kaposi’s Sarcoma (GHESKIO) May 2, 1982 ETHICAL CONCERNS • Necessity to Improve Informed Consent Process ▪ Development of a model for appropriate counseling and evaluation of volunteers knowledge and real desire to participate Fitzgerald DW, Marotte C, Verdier RI, Johnson WD, Pape JW. Comprehension during informed consent in a less-developed country. Lancet 2002; 360: 130 -02. • Need for Credible Local IRB Pape JW. Ethics Review Committees: Consideration in Developing Countries. Emerging Infect Dis 2001; 7: 3 Fitzgerald DW, Wasunna A, Pape JW. Ten questions institutional review boards should ask when reviewing international clinical research protocols. IRB 2003; 25: 14 -8
")
ETHICAL CONCERNS at the Haitian Study Group on Opportunistic Infections and Kaposi’s Sarcoma (GHESKIO) May 2, 1982 • Provision of HAART to Seroconverters Fitzgerald DW, Pape JW, Wasserheit JN, Counts GW, Corey L Provision of treatment in HIV-1 vaccine trials in developing countries. Lancet 2003; 362: 993 -994. • Enhancing the understanding of the informed consent process in HIV Research Joseph P , Schackman BR, Horwitz R, Nerette S, Verdier RI, Wright P, Johnson W, Pape JW, Fitzgerald DW. The use of an educational video during informed consent in an HIV clinical trial in Haiti. J Acquir Immune Defic Syndr. 2006; 42: 588 -91. .

Strategies to Improve Informed Consent • Sensitization Posters, pamphlets, generic video • Willingness Questionnaire • Designing a standardized questionnaire aimed at evaluating the knowledge and motivation( PI, Co-PI, Psychologist, Regulatory Manager, Co-Investigators) • Educational sessions • Evaluation of the comprehension before signing the Consent Form • Evaluation of the level of motivation before enrollment

Education Sessions • The procedure used in informed consent is to inform volunteers about all aspects of the protocol: ▪ With easy simple terms that they can understand explain in creole ▪ For consistency and educational purpose, the consent form has been translated in creole • An illustrated booklet has been produced, dealing with key issues raised in the protocol • A generic and specific educational videos have been develop in order to standardize the educational message.
 educational sessions including a 15 minutes protocol")
Education Sessions • At least, three (3) educational sessions including a 15 minutes protocol specific video and two face to face sessions with a counselor. • The comprehension and the level of motivation was evaluated by a psychologist not involved in the educational sessions. • A grading system was established for consistency • Those who failed received additional informative sessions and be reevaluated

Educational Booklets

 Altruistic Reasons")
Volunteers Motivation to Participate in HIV Vaccine Trial 026 n= 123 1) Altruistic Reasons : 116/123 (94%) 1. Contribution to find an HIV vaccine (n=75) 2. Importance of the study for Haiti (n=15) 3. Other good reasons to participate (n=26) 2) Non Altruistic Reasons : 7/123 (6%) 1. Received care at GHESKIO (n=4) 2. Member of family with AIDS (n=2) 3. Knowledge of health status (n=1)

Obtaining Informed Consent • For illiterate participants, a witness other than the staff person obtaining consent is present in the consent process • Study staff reads the consent documents to the participant in front of the witness, and have the illiterate person sign or “make their mark” on the consent form, in addition to the witness signature.

Future directions • Ethical principles should always guide decisions and behavior with regard to research • Continuing application of International code on harmonization (ICH) guidelines is essential for all research studies in the Caribbean region. • Ethical committees for research should be set up at sites where not available; consider a Caribbean IRB • Finally, it is possible to obtain proper inform consent even if dealing with vulnerable populations

Acknowledgement • GHESKIO Centers ▪ Marie Marcelle Deschamps ▪ Patrice Severe ▪ Sandy Nerette Fontain • Weill Medical College of Cornell University ▪ Daniel W Fitzgerald ▪ Warren Johnson Jr ▪ Jean William Pape ▪ Emmlyne Emmanuel ▪ Rose Irene Verdier ▪ Sonia Simone Jean ▪ Yvanne Philistin ▪ Danie Archange ▪ Hubert Abner Pierre • Vanderbilt University ▪ Peter F Wright

Trans-Caribbean HIV/AIDS Research Initiative A multicultural Caribbean united against HIV/AIDS “The Trans-Caribbean HIV/AIDS Research Initiative: Building Cross. Cultural, Trans-National, Multidisciplinary Research Collaborations” The context for conducting HIV/AIDS research in the Caribbean: Issues in career development for junior investigators in the Caribbean Nanet M. Lopez-Cordova, Psy. D. Ponce School of Medicine Puerto Rico

Introduction ▪ Description of current situation in the Caribbean with junior researchers ▪ Identification of obstacles in career development ▪ Plan of action

From the Perspective of a Junior Investigator § Sharing Experiences § New members & challenges § Differentiation of islands/countries § Achievements of junior investigators § “Graduation”/Transitions

From the Perspective of a Junior Investigator • “Independent/Why? • Obstacles/challenges • The CHALLENGE • Facing the CHALLENGE

Ways to Further the Career of Junior Researchers in the Caribbean § Know yourself. § Recognize your genuine interest as a researcher/clinician involved in issues related to HIV/AIDS in the Caribbean region.

Ways to Further the Career of Junior Researchers in the Caribbean • Recognize and clarify the conceptions and misconceptions about identity as members of the Caribbean toward our neighbors. • We must challenge and improve them. • This is relevant to become a culturally competent researcher/clinician.

Ways to Further the Careers of Junior Researchers in the Caribbean • Identify mentors in your region and in other islands/countries. • That can provide and assist you in the process of developing a research project, a mentor-mentee relationship that will encourage and help you develop a career as a culturally competent Caribbean researcher/clinician.

Ways to Further the Careers of Junior Investigators • Promote and research new-found information through readings, conferences, workshops and by asking continuously questions about your area of interest.

Ways to Further the careers of Junior Investigators • Demonstrate your commitment within the field of HIV/AIDS research and clinical work by working and/or conducting research and sharing your findings and mishaps with other colleagues from the region.

Ways To Further the Career of Junior Investigators • Finally and most significantly, become a Mentor yourself by sharing with others your experiences and always emphasizing the importance of understanding, cooperation, fraternity and growth in the Caribbean region.

Quote from John Donne • “No man is an Island, entire of itself; every man is a piece of the Continent, a part of the main. . . ” • “Ningún hombre es una isla, algo completo en si mismo; todo hombre es un fragmento del continente una parte de un conjunto” • "Aucun homme n'est une île, complet en soi-même; chaque humain est une partie du continent, une partie du tout. "

From the Perspective of a Junior Investigator GRACIAS MERCI THANK YOU

- Slides: 179