Trabecular Bone Score Mozhdeh Zabihiyeganeh M D Associate

Trabecular Bone Score Mozhdeh Zabihiyeganeh, M. D. Associate Professor of Rheumatology Iran University of Medical Sciences valabmd@gmail. com 14 th Nov 2019

Introduction § Osteoporosis is a skeletal disorder characterized by both low bone density & micro architectural deterioration. § Prevention of osteoporotic fracture, needs paying attention to the both surrogates of bone strength.

Introduction § Until recently, a. BMD was the only method used in assessment of osteoporosis and fracture risk. • more than half of the fragility fractures occurred in people with a. BMD above the diagnostic threshold of osteoporosis. § TBS has recently been shown to independently predict fracture risk, to complement standard a. BMD imaging.

Introduction • TBS uses standard DXA spine images to measure texture inhomogeneity that is, how wellstructured or poorly structured the trabecular bone appears when assessed as individual voxels and local variations in gray level distribution.

TBS Monitoring § TBS is not directly dependent on BMD § TBS it’s directly linked to DXA image quality
 Natural position Lordosis reduced by elevating legs L 5 L")
Lumbar Positioning (leg cushion) Natural position Lordosis reduced by elevating legs L 5 L 4 L 3 L 2 L 1



DXA Units Compatible with TBS i. Nsight § Hologic: • • Horizon™ (A, C, W, Ci, Wi) Discovery™ (A, C, W, Ci, Wi) Delphi™ (A, C, W, SL) QDR 4500™ (A, C, W, SL) o Explorer not supported § GE Lunar: • Prodigy™ (all models) • i. DXA™ (all models) o DPX not supported

FRAX-TBS § Considering bone micro-architecture in combination with a. BMD and other risk factors, TBS adjusted FRAX provides its users a 10 -year percentage of the risk of hip fracture (HF) and major osteoporotic fracture (MOF). 12

Caucasian woman, 58 years, smoker 13

Caucasian woman, 58 years, smoker TBS Adjustment 14

Caucasian woman, 58 years Low TBS = 1. 16 Before TBS Adjustment 12% 4% After TBS Adjustment 15

Mirzaei A, et al. Taiwanese Journal of Obstetrics & Gynecology 2018; 57: 389 -93.

Normal BMD and degraded TBS • Two patients were found with normal BMD but fully degraded TBS. • Severe osteophytes were evident in their spines X-rays, which could explain their false positive normal BMD. • Although TBS may have clarified their real bone architecture, there is a debate on the importance of this finding in practice. • Still there is no answer to the important clinical question on how to manage a person with good BMD but poor TBS. Mirzaei A, et al. Taiwanese Journal of Obstetrics & Gynecology 2018; 57: 389 -93.

Role of TBS in fracture prediction ROC curve analysis of different models for prediction of vertebral fracture. All models have been adjusted for age and BMI. Model 1: spine a. BMD Model 2: TBS Model 3: combination of a. BMD and TBS Mirzaei A, et al. Taiwanese Journal of Obstetrics & Gynecology 2018; 57: 389 -93.

§ Aim was to evaluate the ability of lumbar spine TBS to predict future clinical osteoporotic fractures. § A total of 29, 407 women ≥ 50 years of age at the time of baseline hip and spine DXA were identified from a database containing all clinical results for the Province of Manitoba, Canada. § Health service records were assessed for the incidence of non-traumatic osteoporotic fracture codes subsequent to BMD testing (mean follow-up 4. 7 years). Hans D, at al. J Bone Miner Res. 2011; 26: 2762 -9.

Fracture incidence rates in the highest, middle, and lowest TBS tertiles according to lumbar spine BMD category § Spine TBS predicts osteoporotic fractures and provides information that is independent of spine and hip BMD. § Combining the TBS trabecular texture index with BMD incrementally improves fracture prediction in postmenopausal women. Hans D, at al. J Bone Miner Res. 2011; 26: 2762 -9.

TBS and obesity § TBS was negatively correlated with BMI, weight, waist circumference, total body fat mass, trunk fat mass, and trunk lean mass. § TBS software have not recommended the use of TBS in individuals with BMI < 15 kg/m 2 or > 37 kg/m 2. Endocrinol Metab Clin N Am 2017; 46: 153– 180.
")
BMD and TBS in a real obese case (w=105 kg)










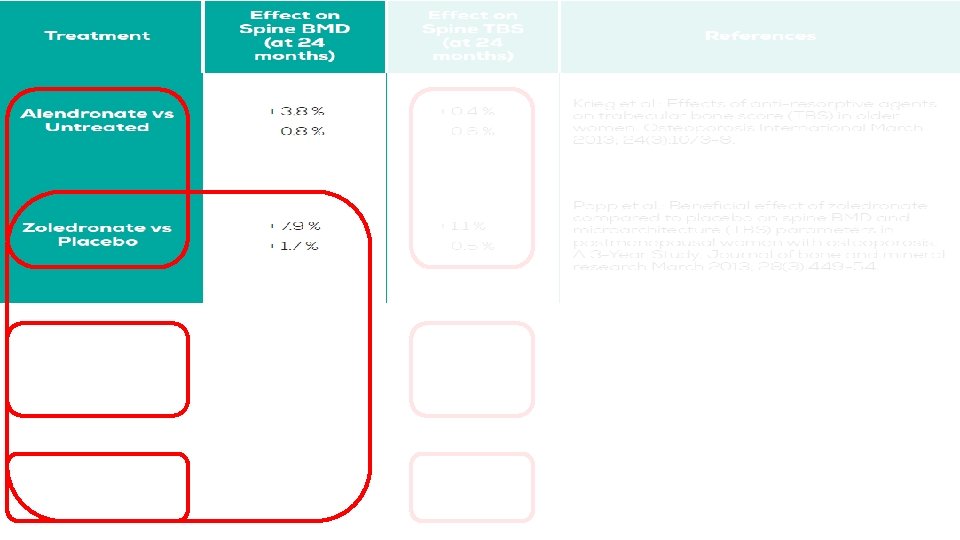
Use of TBS to Monitor Treatment: Review of Selected Studies Senn et al, OI 2014; [2] Del Rio et al, Bone 2015; [3] Krieg et al, OI 2013; [4] Popp et al, JBMR 2013

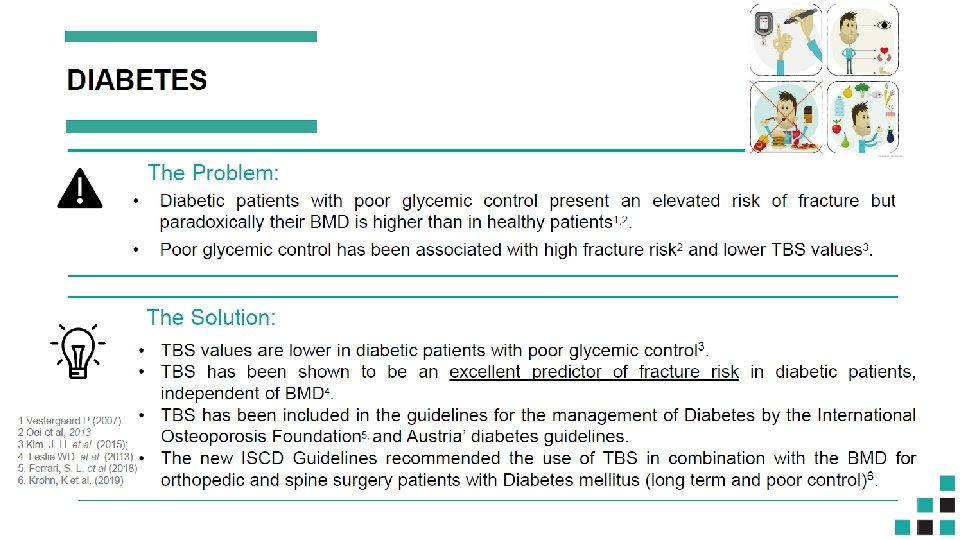
ISCD Official Position § TBS is associated with vertebral, hip, and MOF risk in postmenopausal women. § TBS should not be used alone to determine treatment recommendations in clinical practice. § TBS can be used in association with FRAX and BMD to adjust FRAX-probability of fracture in postmenopausal women and older men. § TBS is not useful for monitoring bisphonate treatment in postmenopausal women with osteoporosis. § TBS is associated with MOF risk in postmenopausal women with T 2 DM.

- Slides: 36