Toxoplasmoza Toxoplasmosis Toxoplasma gondii tachyzoites Giemsa stain Tachyzoites

.")










 Posterior-anterior and (B) lateral views of the")



,")
. Infant girl with congenital toxoplasmosis with hepatosplenomegaly.")














- Slides: 38
Toxoplasmoza
Toxoplasmosis. Toxoplasma gondii tachyzoites (Giemsa stain).
Tachyzoites of T gondii.
§ Tissue cysts of T gondii. A. Tissue cyst freed from mouse brain. B. B. Two tissue cysts (arrows) in section of brain. C. Transmission electron micrograph of a small tissue cyst in cell culture.
Toxoplasmosis. Toxoplasma gondii tachyzoites in cell line. Toxoplasma gondii in infected monolayers of He. La cells (Giemsa stain).
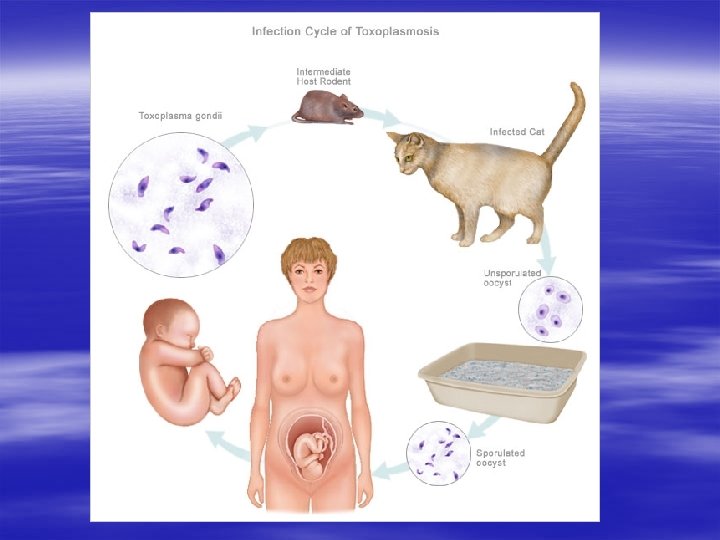
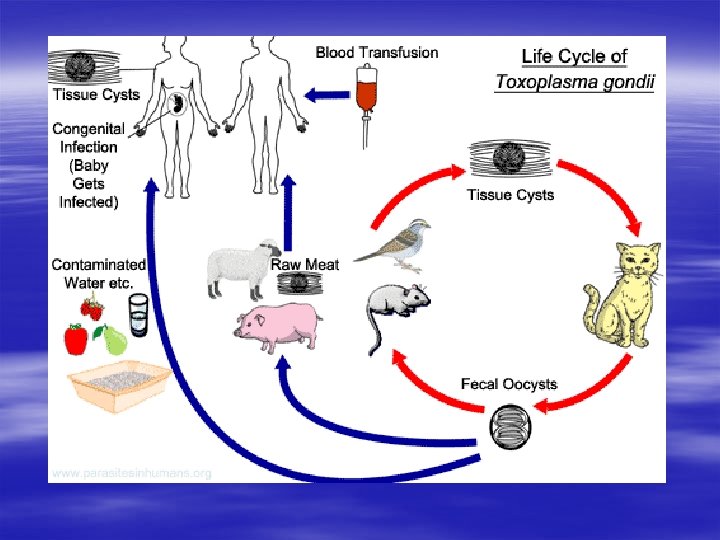
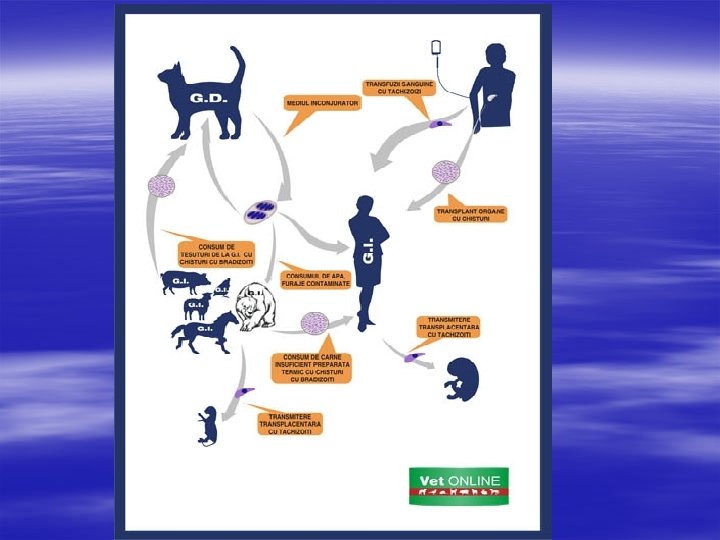
Life cycle of Toxoplasma gondii T gondii has 2 distinct life cycles. The sexual cycle occurs only in cats, the definitive host. The asexual cycle occurs in other mammals (including humans) and various strains of birds. It consists of 2 forms: tachyzoites (the rapidly dividing form observed in the acute phase of infection) and bradyzoites (the slowly growing form observed in tissue cysts).
Mama poate fi asimptomatică. Infectarea precoce, în jurul a 2 -3 luni de sarcină, practic când are loc organogeneza, este foarte gravă, putând apărea avort spontan, moartea fătului la naştere sau leziuni importante neurologice şi oftalmologice, hidrocefalie sau microcefalie, calcificări intracraniene şi corioretinita cronică.
§ Dacă infecţia cu Toxoplasma se produce în cel de-al treilea trimestru de sarcină, copilul se poate naşte viu, dar poate manifesta icter, hepatosplenomegalie, retard psihomotor sau manifestări oculare (strabism, orbire, cataractă) şi hepatice.
Congenital toxoplasmosis § The classic clinical triad of retinochoroiditis, cerebral calcifications, and convulsions defines congenital toxoplasmosis. Other findings include the following: § Hydrocephalus § Microcephaly § Organomegaly § Jaundice § Rash § Fever § Psychomotor retardation
§ Girl with hydrocephalus due to congenital toxoplasmosis
Hydrozephalus Intracranial calcification
§ Intracranial calcifications in congenital toxoplasmosis. (A) Posterior-anterior and (B) lateral views of the skull showing scattered bilateral calcific flecks, nodules and linear streaks in frontal and parietal lobes of an infected infant.
§ Congenital toxoplasmosis with intracranial hyrocephalus. The grossly dilated lateral ventricles are outlined with air on (A) AP and (B) lateral radiographs after pneumoencephalography. There is spreading of the cranial sutures due to increased intracranial pressure.
Acute toxoplasmosis in immunocompetent persons § Approximately 80 -90% of patients are asymptomatic. Symptomatic disease may be characterized as follows: § Patients may have cervical lymphadenopathy with discrete, usually nontender, nodes smaller than 3 cm in diameter § Fever, malaise, night sweats, and myalgias have been reported § Patients may have a sore throat § Retroperitoneal and mesenteric lymphadenopathy with abdominal pain may occur § Retinochoroiditis is reported
Acute toxoplasmosis in hosts who do not have AIDS but are immunodeficient § The disease in these patients may be newly acquired or a reactivation. It may be characterized as follows: § CNS toxoplasmosis occurs in 50% of patients - Seizure, dysequilibrium, cranial nerve deficits, altered mental status, focal neurologic deficits, headache § Patients may have encephalitis, meningoencephalitis, or mass lesions § Hemiparesis and seizures have been reported § Patients may report visual changes § They may have signs and symptoms similar to those observed in immunocompetent hosts. § Patients may have flulike symptoms and lymphadenopathy § Myocarditis and pneumonitis are reported. § Toxoplasmic pneumonitis can occur - Typical symptoms of a pulmonary infection, mirroring in particular P (carinii) jiroveci, including nonproductive cough, dyspnea, chest discomfort, and fever
Clinical manifestations of toxoplasmosis in patients with AIDS § Brain involvement (ie, toxoplasmic encephalitis), with or without focal CNS lesions, is the most common manifestation of toxoplasmosis in individuals with AIDS. § Clinical findings include the following: § Altered mental state § Seizures § Weakness § Cranial nerve disturbances § Sensory abnormalities § Cerebellar signs § Meningismus § Movement disorders § Neuropsychiatric manifestations § The characteristic presentation is usually a subacute onset, with focal neurologic abnormalities in 58 -89% of cases. However, in 1525% of cases, the clinical presentation is more abrupt, with seizures or cerebral hemorrhage.
§ Toxoplasma gondii Infections (Toxoplasmosis). Infant girl with congenital toxoplasmosis with hepatosplenomegaly.
Skin changes are uncommon and non-specific. Macular, maculopapular, papular and haemorrhagic eruptions may occur.
They may be followed by scarlatiniform desquamation. Other lesions have also been described including nodules, urticaria and bullae.
Ophthalmic toxoplasmosis. Macular scar secondary to congenital toxoplasmosis. Visual acuity of the patient is 20/400
Papillitis secondary to toxoplasmosis, necessitating immediate systemic therapy. Acute macular retinitis associated with primary acquired toxoplasmosis, requiring immediate systemic therapy
Peripapillary scars secondary to toxoplasmosis Perimacular scars secondary to toxoplasmosis
§ Inactive retinochoroidal scar secondary to toxoplasmosis
§ Ring enhancing mass with extensive perilesional edema in the left parietal region , with mass effect. A case of toxoplasmosis.
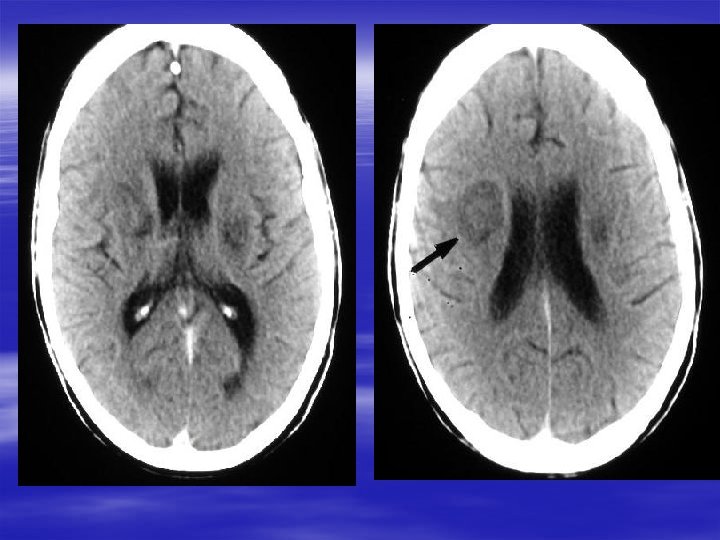
§ Bilateral basal ganglia toxoplasmosis
MULTIPLE TOXOPLASMOSIS- image shows an extensive area of vasogenic edema in the left pariteal cortex. Contrast enhanced scans show multiple ring enhancing toxoplasma.
§ Ventriculitis and hydrocephalus: an unusual presentation of toxoplasmosis in an adult with human immunodeficiency virus
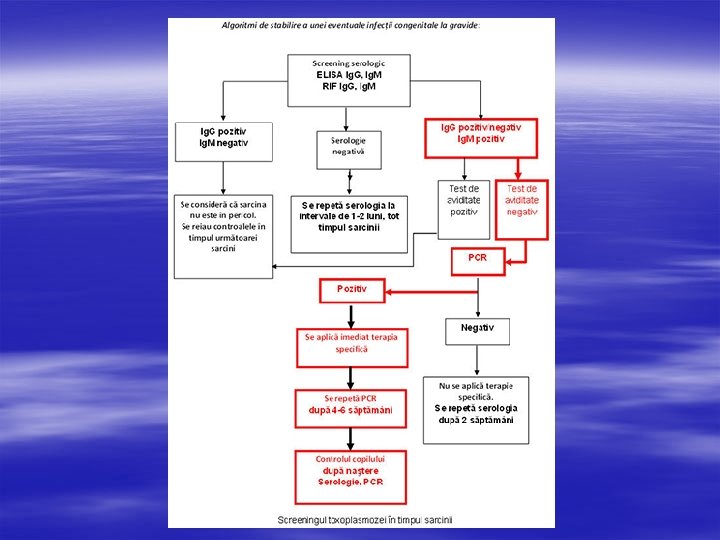
LABORATOR - hemograma - imunologic – teste de tip ELISA pentru determinarea Ig. A, Ig. M, Ig. E, Ig. G specific, index aviditate Ig. G, teste ISAGA pentru determinarea Ig. A+Ig. M anti Toxoplasma IMAGISTIC - ecografie, RMN, CT, Radiografie pulmonara, OCT DIAGNOSTIC GOLDEN STANDARD -teste PCR, teste de tip Western blot (Ig. A, Ig. M, Ig. E, Ig. G specifice), -Examen parazitologic: - examenul unui frotiu de sange, LCR, secretii vaginale, triturat placentar, tesut ganglionar, piese de autopsie colorate Giemsa, Culturi celulare
Tratamentul toxoplasmozei § Pirimetamina/sulfadiazina, Pirimetamina/sulfadoxina, § Spiramicina, Clindamicina, Azitomicina, Claritromicina § - Atovaquona § - Trimetoprim-Sulfametoxazol