Toxicology for Medical Students Dr Kent Robinson Emergency

Toxicology for Medical Students Dr Kent Robinson Emergency Staff Specialist Liverpool and Campbelltown Hospital's

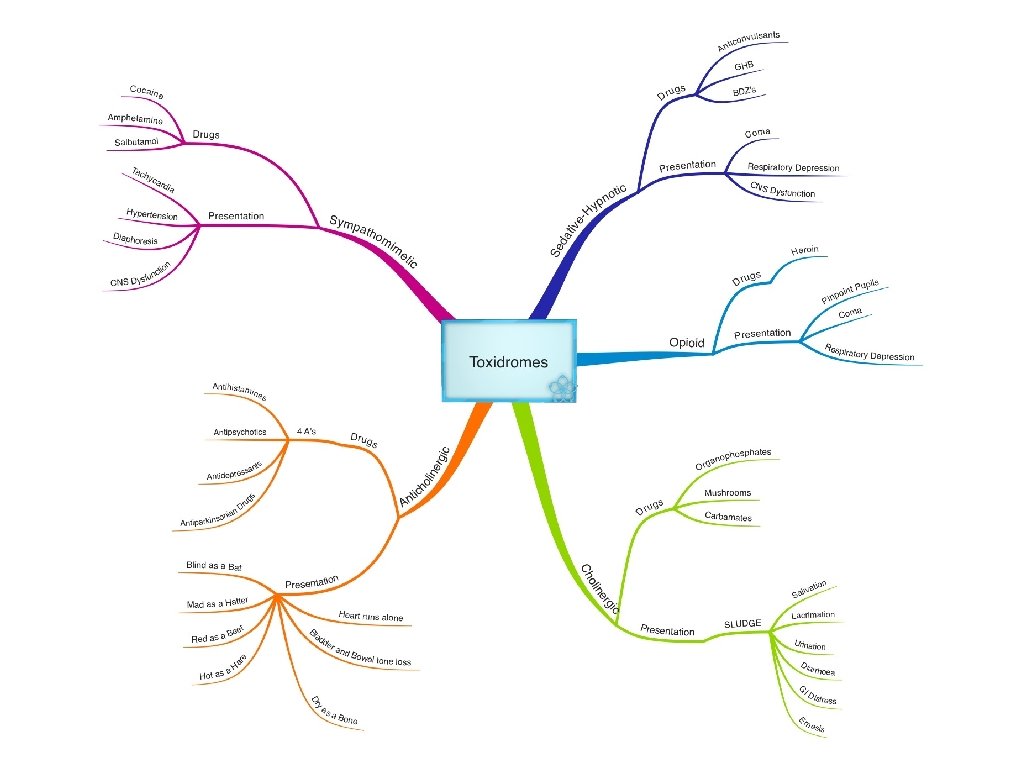
OBJECTIVES • Understand basic approach to the poisoned patient. • Recognose the major toxidromes. • Apply your knowledge to clinical cases.

Approach to Poisoned Patient • Supportive care is the mainstay of therapy. • Decontamination of the patient is now rarely indicated. • In specific situations, antidotes may used in the management of the poisoned patient.

Case 1 • 21 year old female - found down at home • Drug paraphenalia found next to patient • Pinpoint pupils, GCS 3, cyanotic

Case 1 • Naloxone 2 mg x 2 dose intravenous - no response • O 2 therapy, IPPV • How would you manage this patient?

Case 1 • Assess and manage ABC's • Disability - check BSL • Reading "low on glucometer" • Treated with dextrose 25 g iv, GCS to 15/15

Teaching Point In any patient with altered mental status, always check a BSL

Case 2 • 41 year old male brought in from police cells • Patient states he has taken overdose of diazepam • Ataxic and drowsy • Vital signs T 39, P 140 (ST), BP 90/60 • Pupils fixed and dilated • Dry, warm skin, urinary retention

Case 2 • Is this presentation consistent with the stated overdose? • What toxidrome is the patient exhibiting? • What drugs are likely to cause this problem? • How would you manage the patient?

Anticholinergic Toxidrome • Antihistamines • Antipsychotics • Anticonvulsants • Antidepressants • Antispasmodics • Antimuscarincs • Plants - Datura, Mushrooms

Case 2 - Management • Assess and manage ABC's • Sedation - benzodiazepines • One to one nursing care • Intravenous fluids for tachycardia and hypotension • Insertion of IDC • Consider physostigmine if pure anticholinergic overdose.

Teaching Point In patients who present with a drug overdose, always assume that they may have taken drugs other than what they have volunteered.

Teaching Point Patients who present with any overdose - make every attempt to get collateral information.

Case 3 • 18 year old female • Paracetamol overdose (50 x 500 mg tablets) • Observations; T 37, P 90, BP 120/60, GCS 15 • Management?

Case 3 • Assess and manage ABC's • Toxic dose considered to be 150 mg/kg. • Baseline bloods (FBC, EUC, LFT, Coag's, Paracetamol level) • Repeat paracetamol at 4 hours • Start NAC infusion.
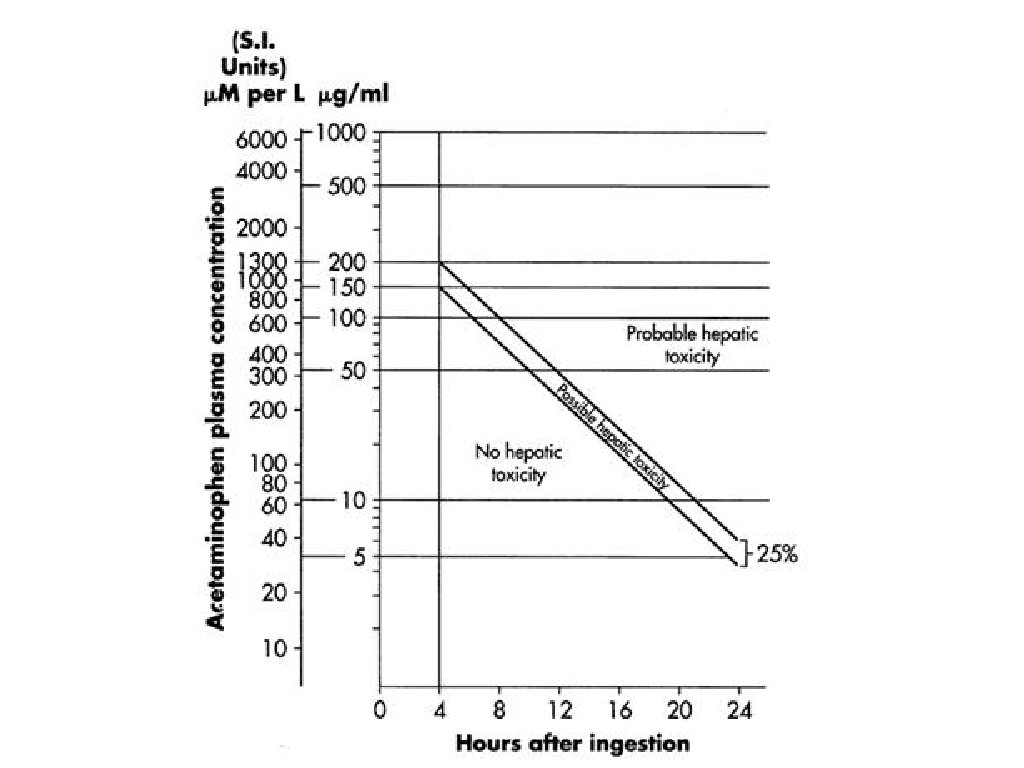
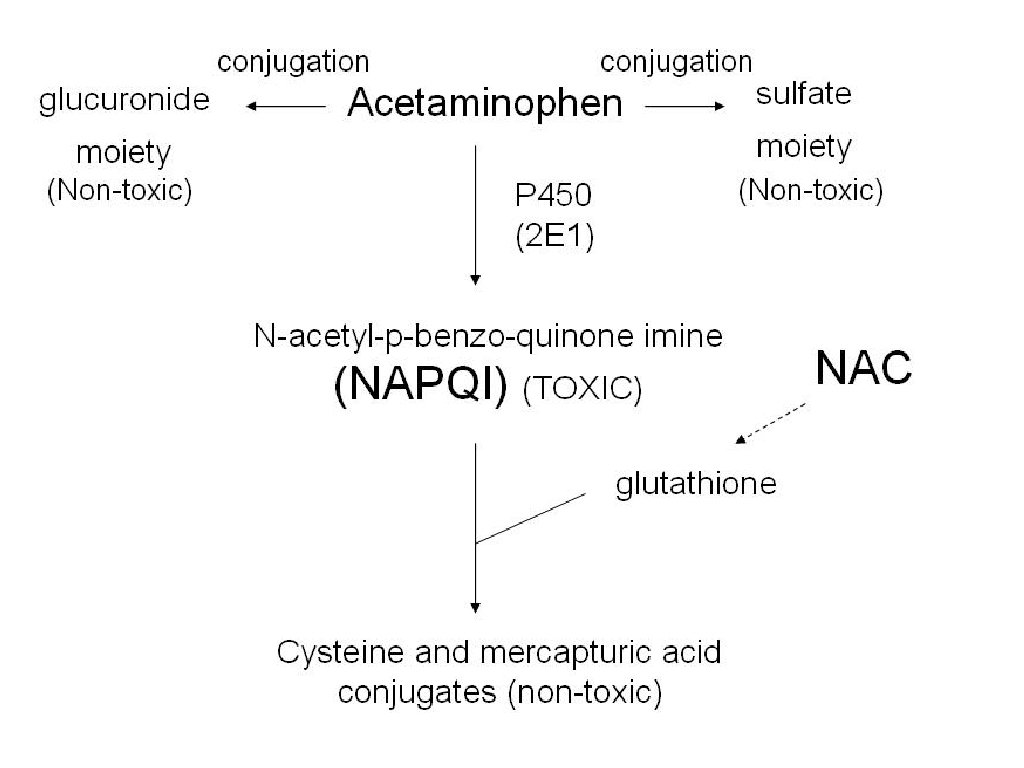

Teaching Point • NAC is the "antidote" for paracetmol toxicity • In the setting of potentially hepatotoxic ingestion, start NAC early. • Decision for ongoing therapy should be based on the 4 hour paracetamol level.

Case 4 • 45 year old male • Chronic alcohol dependence • Alcohol intoxication, presents aggressive and agitated. • Vital Signs; T 37, P 100, BP 110/60, RR 16, GCS 14/15 • Management?
 •")
Case 4 • Assess and manage ABC's (Intravenous fluids for HR and BP) • Check BSL • Give dextrose 25 g and thiamine 300 mg • If no response, will need chemical restraint what agent will you choose to sedate, and why?

Teaching Point • Alcohol and benzodiazepines are sedativehypnotic agents. • Giving a BDZ to an agitated alcoholic will make the problem worse - use an antipsychotic. • Always think of the possibility of intracranial pathology in an agitated alcoholic - low threshold for CT Brain.

Summary • Management of poisoned patient is largely supportive • Decontamination is rarely indicated (seek senior advice) • In specific situations, an antidote may be of benefit.
- Slides: 23