Tools for Measuring and Monitoring Equity in Quality






 developed in 2006 •")









 at UNM Hospitals: Tools for Measuring & Monitoring Equity")






 Sex")
 • Outpatient •")

 Race Ethnicity Age Language (primary oral and")
 Readmission rates Hg.")






- Slides: 36
Tools for Measuring and Monitoring Equity in Quality: The Hospital Perspective Thursday, January 27, 2010 3: 00 -4: 30 pm EST 2: 00 -3: 30 pm CST 1: 00 -2: 30 pm MST 12: 00 -1: 30 pm PST This web seminar will begin momentarily.
Tools for Measuring and Monitoring Equity in Quality: The Hospital Perspective James Walton, DO, MBA Vice President and Chief Health Equity Officer, Baylor Health Care System, Dallas, TX Sarah Rafton, MSW Director, Center for Diversity and Health Equity, Seattle Children’s Hospital, Seattle, WA Susana Rinderle, MA Manager, Diversity, Equity & Inclusion (DEI) at University of New Mexico Hospitals, Albuquerque, NM Joseph R. Betancourt, MD, MPH Director, The Disparities Solutions Center at MGH Moderator
Health Equity Improvement: The Baylor Health Care System Vision and Experience Jim Walton, DO, MBA Vice President & Chief Health Equity Officer Baylor Health Care System Dallas, Texas “Tools for Measuring and Monitoring Equity in Quality: The Hospital Perspective” January 27, 2 -3: 30 pm CST
Baylor Health Care System • North Texas integrated health care system: – 24 owned, leased, affiliated and short-stay hospitals – 120+ primary care, specialty care, and senior health centers – 17 ambulatory surgery centers – 450+ employed physicians in the BHCS affiliated physician network, Health. Texas • 20, 000+ employees • ~127, 000 inpatient admissions annually • >$3. 8 B net operating revenue (FY 09) 3/4/05 This is a test footer. 4 © 2009 Baylor Health Care System
Founding Statement “Is it now time to build a great humanitarian hospital, one to which men of all creeds and those of none may come with equal confidence? ” Dr. George W. Truett, 1903 Co-founder of Texas Baptist Memorial Sanitarium, predecessor of Baylor Health Care System 3/4/05 This is a test footer. 5 © 2009 Baylor Health Care System
Milestones in Baylor Health Care System’s Journey to Equitable Care § Board of Trustees passed Quality Resolution (2000) § System-level Best Care Committee created to develop, implement, and lead quality improvement projects related to achieving STEEEP objectives § Executive compensation aligned with process-of-care measures through the Performance Award Program 3/4/05 This is a test footer. 6 © 2009 Baylor Health Care System
Office of Health Equity • Office of Health Equity (OHE) developed in 2006 • To reduce variation in health care access, care delivery and health outcomes due to: • Race and ethnicity • Income and education (i. e. , socioeconomic status) • Age • Gender • Other personal characteristics (e. g. , primary language skills) 3/4/05 This is a test footer. 7 © 2009 Baylor Health Care System
Office of Health Equity: Goals • • Design and implement an annual “BHCS Health Equity Performance Analysis” (HEPA) & Report: § Quality of Care measures (Core Measures) § Experience of Care measures (Satisfaction) § Outcome measures (Mortality & Readmission) Utilize Health Equity Performance Report as a tool to focus resources and efforts to reduce inequalities and improve quality 3/4/05 This is a test footer. 8 8 © 2009 Baylor Health Care System
BHCS Health Equity Improvement Model 3/4/05 This is a test footer. © 2009 Baylor Health Care System
BHCS Analysis Methodology For each equity measure: § Patient population broken down into dichotomous variables • Race: White vs. Non-White • Ethnicity: Hispanic vs. Non-Hispanic • SES Proxy: Commercially Insured vs. Self-Pay/ Medicaid § Percentages of eligible patients calculated, and the differences between each dichotomous variable are calculated • Identify dichotomous variable differences that are statistically significant (p<=. 05) 3/4/05 This is a test footer. © 2009 Baylor Health Care System
BHCS HEPA Dashboard Baylor Health Care System - FY-10 Health Equity Performance Dashboard Metric WHITE NON-WHITE EQUITY OF CARE NON-HISPANIC EQUITY OF CARE AMI perfect care bundle (%) 97. 9 97. 4 = 97. 8 98. 1 = HF perfect care bundle (%) 96 94. 1 Favors White 95. 5 93. 9 = PNE perfect care bundle (%) 92. 1 91. 8 = 91. 9 92 = SCIP perfect care bundle (%) 94. 5 = 94. 6 94 = Inpatient overall satisfaction mean score 88. 1 87. 4 Favors White 87. 9 88. 9 Favors Hispanic Emergency Department overall satisfaction mean score 87. 5 84. 2 Favors White 87. 1 84. 3 Favors Non. Hispanic AMI=Acute Myocardial Infarction; HF=Heart Failure; PNE=Pneumonia; 3/4/05 This is a test footer. SCIP=Surgical Complication Infection Prevention © 2009 Baylor Health Care System
Office of Health Equity: Patient Experience Measures § Health Equity Performance Metric: § Utilize Press Ganey measurements of patient satisfaction to detect differences among patient variables. § Measurement offers standardized approach to data collection and national baselines for comparison. 3/4/05 This is a test footer. © 2009 Baylor Health Care System
Health Equity Performance: ED Patient Satisfaction-Race Persisting Racial Inequity Observed 3/4/05 This is a test footer. 13 © 2009 Baylor Health Care System
Health Equity Performance: ED Patient Satisfaction-Race First Qtr. Patient Responses Baylor Hospitals 3/4/05 This is a test footer. © 2009 Baylor Health Care System
BHCS Health Equity Improvement Strategy § Establish organizational disparity sensitivity § Push data out to operating unit (hospital) leaders, influencers and front line staff § Ready evidence-based literature supporting evaluation metrics and conclusions § Assemble workgroups evenly dispersed organizationally and by experience level § Analyze again…and again 3/4/05 This is a test footer. © 2009 Baylor Health Care System
Conclusions § Health Equity must be a shared value; § Disparities in health outcomes exist as do inequities in health care access and delivery: find Module 3: Health Equity Performance Improvement Exercise the evidence; § As health care professionals, we have a duty to lead with evidence and improve health inequities. § Improving health equity is consistent with the Baylor mission 3/4/05 This is a test footer. 16 © 2009 Baylor Health Care System
Diversity, Equity & Inclusion (DEI) at UNM Hospitals: Tools for Measuring & Monitoring Equity Susana Rinderle, M. A. Manager ~ Diversity, Equity & Inclusion University of New Mexico Hospitals DSC webinar January 27, 2011
UNM Hospitals • Only public and only teaching hospital of note in New Mexico – • • One of only 30 hospitals nationwide who are both public safety net and teaching/academic Only Level I Trauma Center in the region Only emergency adult psychiatric services 619 beds: 5 hospitals, 48 clinics (22 offsite) Employees: ~6, 000 Providers: 579 faculty, 116 midlevels Outpatient visits: 492, 000 Inpatient days: 180, 000 Budget: $705 million
New Mexico • • • Population: nearly 2 million State with fourth highest percentage of “frontier lands” One of only two states in the U. S. that have always been “majority-minority” The only majority Hispanic state in the U. S. at 45. 6% (California and Texas follow behind at 37%) State with second highest percentage of Native Americans (fifth highest total number) The state with the second highest percentage of residents that speak a language other than English at home, at 36. 5% Source: Census Bureau
Diversity, Equity & Inclusion • Interpretation – since 2003 • 18 full time interpreters (14 Spanish, 3 Vietnamese, 1 Navajo), 1 educator, 2 admin support staff • • • Only in-house interpreter dept. in state 130 dual role interpreters in 9 languages Video interpreting Pacific Interpreters 24 -hour phone line Participation in the Disparities Solutions Center Disparities Leadership Program, third cohort 2009 -2010 Office of DEI created October 2010
What is DEI? The UNMH Office of Diversity, Equity & Inclusion leads the effort to make sure that every UNMH patient receives the safest, most effective, most sensitive medical care possible, regardless of the patient’s race, ethnicity, or any other group identity. We do this through data collection and analysis; community collaboration; cultural “competence” training, education and consulting; and process improvement.
How does DEI do these things?
QUALITY COMPLIANCE COMPETENCE COMMUNITY CARE DISPARITIES Diversity is a driver of quality
2010: “REALS” data Race Ethnicity Age Language (primary oral) Sex
Collection and use of REALS • 100% electronic medical record (EMR) • Outpatient • Self-reported on a form at registration and data entered into EMR by staff • Inpatient • Same self-reporting process at all points of entry (ED, admitting) • Included in unit/department “Operational Plans” effective July 2010
You have a right to an interpreter. UNM Hospitals will provide one free of charge – just ask us! Please place patient’s registration sticker here. UNM Hospitals is dedicated to providing the highest quality care regardless of a patient’s race/ethnicity. Your response to the questions below will help us to monitor care and ensure our patients receive the best care possible. Your information will remain private and access to this information will be highly restricted. 1. Please select the language you would like to receive services in. Other Languages: Most Common at UNM Hospitals: q Arabic q English q Chinese (Mandarin) q Spanish/Español q Dutch/Nederland q Vietnamese q Farsi q Sign Language/ASL q French/Français q Keresan q German/Deutsch q Navajo q Italian/Italiano q Tiwa, Tewa or Towa (circle) q q q q Japanese Portugese/Portugais Russian Swahili Turkish Zuni Other __________ 2. If you would like an interpreter, we can provide one free of charge, either in-person or by phone. Do you want UNM Hospitals to provide an interpreter for your visit today? (please circle) Yes No 3. Select from the following choices to provide us with your race/ethnicity information. If you are multiracial, please select the race/ethnicity with which you primarily identify yourself. q American Indian or Alaskan Native q Tribal Affiliation______________________________________ q Asian, Vietnamese, or ________________________________ q Native Hawaiian/Pacific Islander, or __________________________ q Black or African American or ____________________________ q Hispanic or Latino or ________________________________ q White or Anglo__________________________________ q Other ______________________________________ q Decline to answer. 4. Patient signature: ______________________________ Date: __________ Thank you for your assistance! If you have any questions, please ask one of our staff. Hospital staff: Please enter response into Cerner and then forward this info through campus mail to Interpreter Services, 1 -South
2011: “SOREAL” data! Sex Orientation (sexual orientation/transgender) Race Ethnicity Age Language (primary oral and written)
Initial data indicators Clinical: • • Mortality Length of stay (LOS) Readmission rates Hg. A 1 C levels Outpatient pneumovax vaccines Inpatient core measures for pneumonia Childhood immunizations or asthma Colorectal cancer screening Non-clinical: • Employee race, ethnicity, age, sex and (a) job position and (b) organizational level • Employee satisfaction • Patient satisfaction • Patient no-show rates • Patient/family complaints • Self-reported employee/provider awareness, attitudes, beliefs (pending)
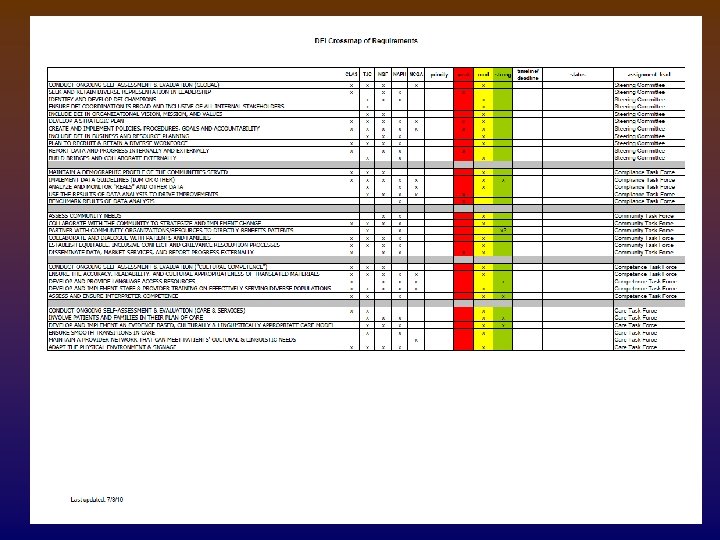
First equity dashboard
First equity dashboard
Next steps • Modifications to data fields and collection form • • • Separation of race & ethnicity Changes to tribal and religion categories Exploring options for multiracial category Addition of written language Adding LGBT information • Analysis of initial equity dashboard findings • Strategic plan and recommendations to Competence and Care task forces • Rollout of unit-specific and organization-wide training, system and process changes, and other interventions
What questions do you have? Susana Rinderle, M. A. Manager, Diversity, Equity & Inclusion (DEI) Chair, Health Literacy Task Force UNM Hospitals 933 Bradbury Drive SE, Suite 3057 Albuquerque, NM 87106 tel (505) 272 -1698 pager (505) 951 -3927 fax (505) 272 -5477 http: //hospitals. unm. edu/dei/index. shtml
Question and Answer Period
Thank you for your participation.