TonsilAdenoid Issues Hyponasality vs Hypernasality Differential Diagnosis and








")

 A Resonance Disorder The simultaneous occurrence of hypernasality and hyponasality in")

















 SPEECH Reduced articulation and sound clarity. IMPRECISION!")
 Eating Slow eaters Mouth breathers … BITE,")
 Sleep disturbance Signs of sleep apneasnoring, labored")

")



,")





. Childhood adenotonsillectomy study for children with OSAS (CHAT).")
- Slides: 45
Tonsil/Adenoid Issues: Hyponasality vs. Hypernasality. Differential Diagnosis and Treatment THERESA M. SNELLING MA, CCC-SLP Theresa M. Snelling and Assoc. , Inc. Lakewood, Colorado t. snell@hotmail. com Co-Author. SARAH SOGAN, MA, CCC-SLP
Disclosures- no financial disclosures related to this presentation: Non-Financial Speech Therapy Coordinator/Volunteer for the International Children’s Surgical Foundation (mission team) Advisory committee member on the Board of Face to Face Colorado/Cleft Family Support Group Member of ACPA and ASHA Sig 5 Brief BIO: Yearly Instructor for Cleft Palate portion of the Voice Class at University of Northern Colorado (Greeley, CO) Speech Pathologist and owner at Theresa M. Snelling and Associates in Lakewood CO Clinical Coordinator for the Rocky Mountain Cleft Palate and Craniofacial Center at P/SL 2002 -2019.
OVERVIEW 1. Resonance 2. Hyper vs. Hypo/Differential Diagnosis 3. Anatomy 4. Function 5. Characteristics of obstruction 6. Special Populations 7. Referral Considerations
Speech requires… Phonated sound which is altered by resonance: generated from vocal fold vibrations Modified by RESONANCE Important for vowels and voiced consonants Airflow which is stopped or constricted and alters pressure and volume: Up from lungs and altered by articulators Important for high pressure phonemes Required for voiceless consonants
From: Cleft Palate and Craniofacial Anomalies: Effects on Speech and Resonance, 3 rd Edition: Ann W. Kummer, Ph. D. , CCC-SLP Lungs VC Vibration Sound Open Glottis Airflow Air Pressure Resonance Vowels and Voiced Consonants Pressure Sounds, particularly Voiceless
Changes in Size and Shape of Cavities- alters speech/sound: Pharyngeal Oral Cavity Nasal Cavity
Velopharyngeal Valve Structures
RESONANCE BASED ON HOW AIRFLOW IS SHAPED THROUGH THE ORAL AND NASAL CAVITIES
HYPERNASALITY- A Resonance Disorder A Resonance disorder characterized by excessive nasal resonance (in nose) during production of primarily vowels and oral voiced consonants). Abnormal coupling of oral and nasal cavities during speech Associated with speech sounds that are phonated More perceptible in vowels (more noted on high vowels than low vowels) Hypernasality on vowels and nasalization on phonemes increases in connected speech
HYPONASALITY- A Resonance Disorder A resonance disorder A reduction in normal nasal resonance resulting from a partial or complete blockage (DENASALITY) of the nasal airway by any number of sources. Blockage can occur from level of soft palate through the nares and all points in between
MIXED NASALITY (HYPERHYPONASALITY) A Resonance Disorder The simultaneous occurrence of hypernasality and hyponasality in the same speaker usually as a result of VPI (velopharyngeal insufficiency) in the presence of high nasal resistance that is not sufficient to block nasal resonance completely. DENASALITY- when nasal resonance is completely blocked
Associated patterns related to RESONANCE DISORDERS NASAL SUBSTITUTIONS -incomplete VP closure causes oral consonants in the correct place of articulation to be produced as nasal consonants… **m/b, n/d, ng/g OFTEN SEEN WITH HYPERNASALITY NASAL EMISSIONnasal air escape associated with production of consonants requiring high oral pressure. May be audible or not (check with a mirror. )
HYPO vs. HYPER What does “NASAL” mean? Hypo-Nasality Candy… sounds like “cady” Me, me, … sounds closer to “be, be. ” Hyper-Nasality Vowels resonate in nose… Say “EEEEE” and pinch nose, air stops or sound changes… “baby” may sound more like “Mayme” YOU HAVE TO BE ABLE TO DIFFERENTIATE!
Avoid the term “NASAL”! ”They sound nasal…” “Sounds like s/he is talking through their nose” …does NOT differentiate hyponasality and hypernasality.
Quick screen… Use a small mirror under nose… Use a straw or listening tube per Anne Kummer’s book (in references). On “mmmm” does air flow equally through both nostrils? On “baby, baby…” there should be no nasal airflow on mirror (unless they stop and breathe… then try with one word. ) !
Adenoid
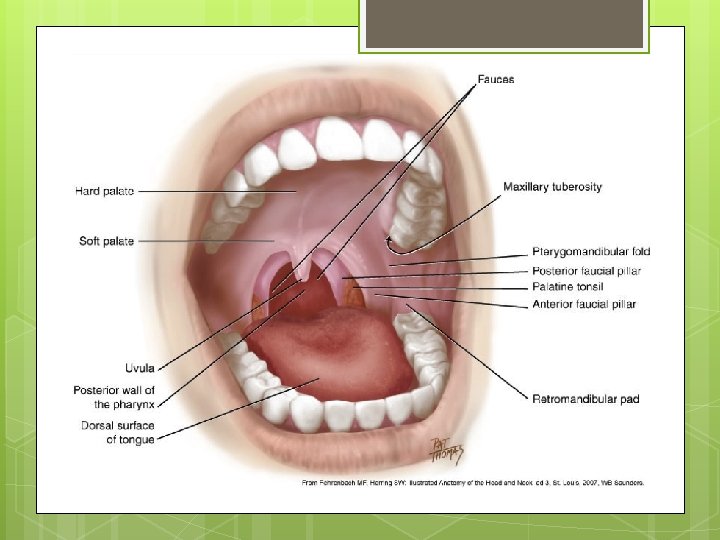
WHERE are tonsils and the adenoid located…? newenglandent. com
Velopharyngeal Valve Structures
Tonsil Classifications 0 -4
ANATOMY PALATE FUNCTION WHAT CAN OBSTRUCT?
Tonsils- 3 TYPES Palatine tonsil- tonsils you CAN SEE Collection of Lymph tissue Right and left of upper throat (oropharnyx)
TONSILS -3 TYPES THIRD TYPE PHARYNGEAL TONSIL- more commonly referred to ADENOID Located in the nasopharynx BEHIND the soft palate! Not easily visualized!
TONSILS -3 TYPES Lingual tonsilslocated at base of tongue Difficult to visualize Remember locationcan’t see- CAN impact speech and airway
ANATOMY test…. Where are the Palatine tonsils? Where are the Lingual tonsils? Where are the anterior faucial pillars? Posterior faucial pillars? Where is the Adenoid? Where are the remains of the Oreo Cookie his mother fed him? ? ?
Medical DEBATE re: TONSILS ENT Reseach ENT community does not focus as much on IMMUNE benefit No adverse effect reported by removal (usually do better) Reason for removal less for infection/more for obstruction Can become more “Dysfunctional” and more of a liability than an asset. Report tonsils play a role in immune system to fight infection Defense function greater in children By age 6 -7 limited immune function In current urban society, not effective in containing infection (prior society for worms or parasites. )
American Academy of Otolaryngology 2011 GUIDELINES ON TONSILLECTOMY DUE TO INFECTIOIN… 7 throat infections in one year 5 in each of 2 years 3 in each of 3 years THROAT INFECTIONS DEFINED AS HAVING ONE OF THE FOLLOWING: Fever of 101+ degrees Discharge on tonsils Swollen lymph nodes in neck Positive Strep culture
CASE STUDY 9 year old 6 Strep/throat infections in one year Missed 11 days of school Scheduled tonsillectomy/adenoidectomy Insurance called day before procedure scheduled to cancel- ONLY 6 Strep! Filed a greivance with Insurance Commission Insurance commission came back and mandated procedure be paid for by insurance Start of this school year to December- did not miss one day of school!
Cul-De-Sac resonance and glottal distortion SOUND IS BLOCKED FROM EXITING A CAVITY Pharyngeal cul-de-sac Oral Cul-de-sac Nasal Cul-de-sac What might create the blockage at these levels of these structures?
SYMPTOMS OF OBSTRUCTION OF THE ORO-NASAL-PHARYNX (handout) SPEECH Reduced articulation and sound clarity. IMPRECISION! Cul-de-sac resonance Glottal distortion Denasal voice quality Mixed nasality (seen with cleft palate and obstruction Oral Characteristics Pooling of saliva Drooling Sores on Margins of mouth Open mouth breathing Tongue thrust Orthodontic issues Open Bite High Arched Palate (Adenoid Faces)
SYMPTOMS OF OBSTRUCTION OF THE ORO-NASAL-PHARYNX (handout) Eating Slow eaters Mouth breathers … BITE, BREATH, CHEW, BREATH, BITE, BREATH… Failure to thrive/ slow growth “messy” eater Ears History of chronic otitis media Chronic middle ear fluid 2 nd set of PE tubes (warrants adenoid evaluation) Eustachian tube dysfunction
SYMPTOMS OF OBSTRUCTION OF THE ORO-NASAL-PHARYNX (handout) Sleep disturbance Signs of sleep apneasnoring, labored breathing, observed apnea (cessation of breathing), restlessness Excessive daytime sleepiness (teens) Hyperactivity Bed wetting Irritability Behavior and Learning Problems
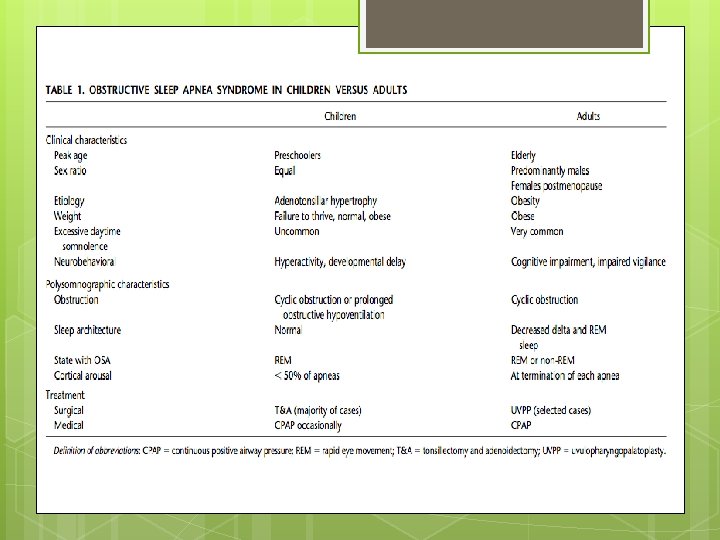
SDB-SLEEP DISORDERED BREATHING 3 - LEVELS Severity: Primary snoring Snoring with apnea, hypoventilation or sleep disturbances- no daytime symptoms. Upper Airway Resistance Syndrome Middle of the spectrumassociated with increased respiratory effort and daytime symptoms OBSTRUCTIVE SLEEP APNEA Most severe end of the spectrum characterized by Obstruction that disrupts normal ventilation and normal sleep pattens
ASHA Leader July 2013 A study of pt. with OME (otitis media with effusion) benefit from PE Tubes with removal of adenoid, either alone or in combination Decreases duration of OME by up to 2 years. Newer evidence showed no benefit from oral or nasal steroids. (Theresa and Sarah’s experience too!)
Handout Summary for obstructive sleep symptoms for screening and parent questionnaire. This information from parent, is suggestive of airway obstruction, is information parent needs to share with ENT or Pediatrician for evaluation.
CASE STUDY 3 1/2 year old female Referred by ENT for speech evaluation; reduced intelligibility; Per Mom ”Hard to understand” No history of recurrent strep or tonsil infections Obstructive sleep symptoms and daytime sleepiness beyond her age Imprecise articulation; LARGE 3+ tonsils bilaterally Denasal Drooling Pools Saliva “Messy” eater Articulation placement was accurate but connected speech was muffled with reduced speech intelligibility. RECOMMENDATION: Tonsillectomy/Adenoidectomy; *no speech therapy recommended. Follow-up with speech 4 -6 weeks after T&A. RESULTS: speech intelligibility improved to WNL; no need for speech therapy. Per mom, temperament improved, better eating, no snoring at night and no drooling.
A. B. C. D. Coronal Sagittal Circular with Passavant’s ridge http: //sig 5 perspectives. pubs. asha. org/article. aspx? articleid=1768695
Special populations-Cleft Palate In the presence of secondary surgical management (pharyngeal flap. Sphincterpharyngoplasty, Furlow-Zplasty), patients are more at risk for obstruction IF TONSILS AND ADENOID ARE PRESENT.
Special populations-Cleft Palate Recommendations: 1. Do adenoidectomy and/or tonsillectomy, if PRESENT, before secondary surgical management. 2. POST Pharyngeal Flap or Sphincter Pharyngoplasty- monitor airway for signs of obstruction
Special Populations. Cleft Palate 8 year old with repaired cleft palate with cul-de-sac resonance post severe tonsillar hypertrophy. Per parent report, likely obstructive sleep apnea. Child is a patient from medical mission in Philippines and tonsillectomy is not available.
Special Populations-Cleft Palate 4 year old female with cleft palate post pharyngeal flap (low flap) with tonsils sitting in lateral ports. Sleep study showed severe sleep apnea. P-Flap taken down, tonsillectomy and adenoidectomy and palatal revision (sphincter pharyngoplasty). Ongoing speech therapy.
Special Population DOWN SYNDROME 50 -100% incidence of Obstructive Sleep Apnea in people with Down Syndrome; 60% of children with D. S. have abnormal sleep studies by age 3. 4 -4 years old. Incidence of OSA increases with age. American Academy of Pediatrics recommend baseline polysomnogram by age 4 years.
Special Population DOWN SYNDROME Tonsillectomy and Adenoidectomy may not resolve all OSA issues in some patients with D. S. Lingual tonsils should still be explored. Other factors related to OSA in DS: *GERD *Chronic postnasal drip=edema of the pharynx. *Re-growth of adenoid tissue *Mid-face hypoplasia (narrow passages of midface and throat)
REFERENCES: Redline, S. et al. (2007). Childhood adenotonsillectomy study for children with OSAS (CHAT). Clinicaltrials. gov. Retrieved from: https: //clinicaltrials. gov/ct 2/show/study/NCT 00560859. Sterni, L. M. & Tunkel, D. E. (2003). Obstructive sleep apnea in children: An update. Pediatric Clinics of North America, 50(2), 42743. Maris, M. , Verhulst, S. , Wojciechowski, M. , Van de Heyning, P. , & Boudenwyns, A. (2016). Prevalence of obstructive sleep apnea in children with Down Syndrome. Sleep, 39(3), 699 -704. Mitchell, R. B. (2007). Adenotonsillectomy for obstructive sleep apnea in children: Outcome evaluated by pre- and postoperative polysomnography. Laryngoscope, 117(10), 1844 -54. Kummer, A. W. (2014) Cleft Palate and Craniofacial Anomalies: Effects on Speech and Resonance (3 rd ed. ) Englewood Cliffs, NJ: Thomson Delmar Learning