Tips and Tricks of The Crossboss and Stingray

Tips and Tricks of The Crossboss and Stingray re-entry system William L. Lombardi MD FACC FSCAI Peacehealth St. Joseph Medical Center

William L. Lombardi, MD Stocks, Stock Options, other ownership interest: Bridge. Point Off-Label: Only products indicated for CTO is crossboss, stingray balloon and guidewire; all other interventional equipment is off-label.

New Devices for North American CTO

The Hybrid Algorithm for CTO PCI provisional approaches Dual Catheter Angiography yes no 1. Clear proximal cap 2. Good Distal Target Retrograde Antegrade yes Wire escalation no fail 3. Length < 20 mm Dissection Reentry (crossboss-stingray) fail Dissection Reentry (reverse CART) no yes Wire escalation fail Dissection Reentry (reverse CART) fail Dissection Reentry (crossboss-stingray))

Refractory RETROGRADE ANTEGRADE

Antegrade Wiring Algorithm Game changing event

Antegrade Dissection and Reentry Algorithm n n Predictable Controllable Teachable Reproducible

Challenges to overcome Wire Subintimal n Failure to get the Crossboss started n Cross. Boss gets stuck at, or goes into side branch n Failure to re-enter with Stingray guidewire n Questions of whether re-entry with stingray wire is correct n Hematoma formation n

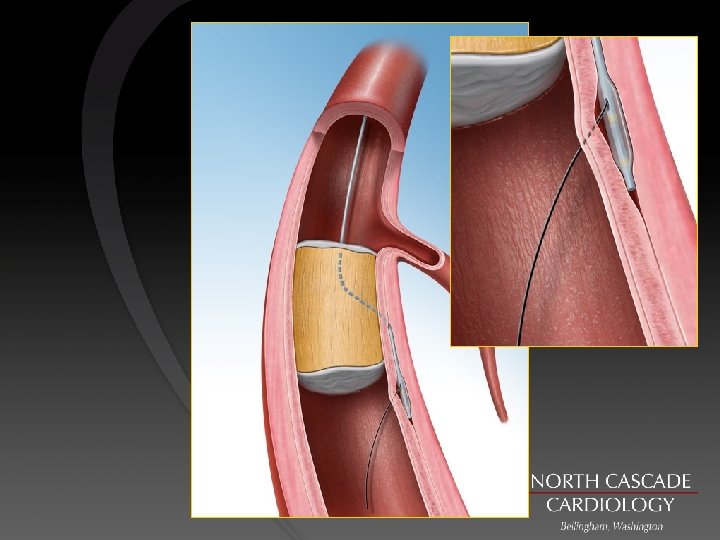
Stingray Balloon

Wire Subintimal the new approach

Bridgpoint techniques n Crossboss won’t get through proximal cap • Knuckle boss • Dilate proximal cap then place boss

Bridgepoint techniques • Show Cross Boss in Sidebranch no dance

Bridgepoint tips n n Show wire redirect Show Knuckle redirect
 n After")
Failure to obtain re-entry Either reposition stingray balloon to new location (bobsled) n After puncture use soft wire to exit into true lumen as stingray wire may have gone subintimal/true lumen/sub intimal • Pilot 200 n

Managing the reentry zone n n Minimize antegrade flow into tha antegrade dissection Do not allow knuckled wire into the re-entry zone Finish with boss If wire subintimal dilate with small 1. 5 or less or with corsair to allow delivery of stingray balloon without compressing the distal true lumen

Re entry techniques: Problem solving Compressive hematoma n n Hematoma compression can result in failure or bailout to retrograde Stenting hematoma can result in propagation


Re entry techniques: Problem solving Compressive hematoma n Avoidance is preferred • Controlled dissection- crossboss • Knuckle control- XT, trapping, MB 12 • Avoid antegrade injections

Re entry techniques: Problem solving STRAW 2 Prior failures No retrograde option

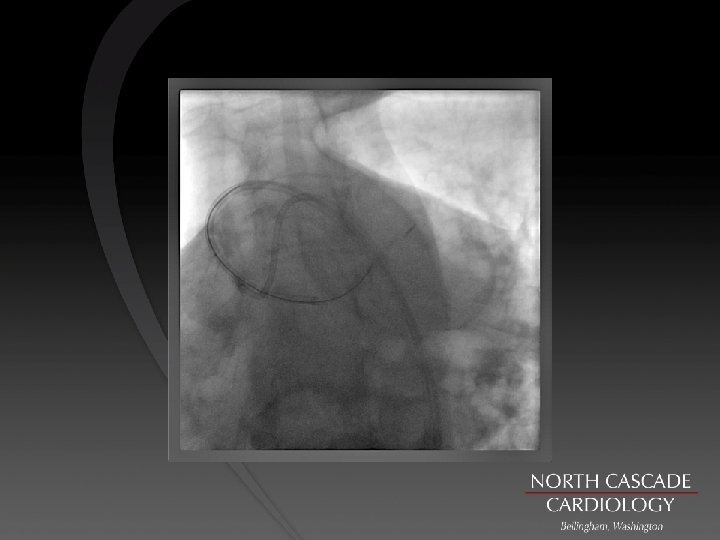
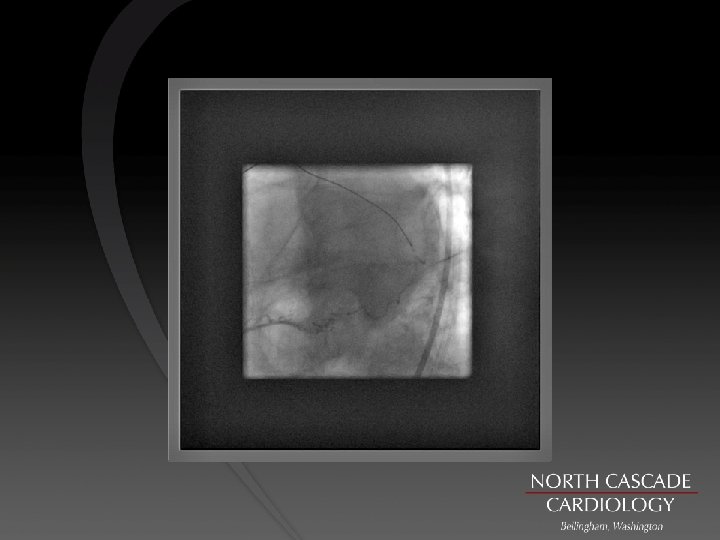
STRAW Technique

STRAW Technique Enhanced support with anchor , dilated proximally then knuckle boss technique

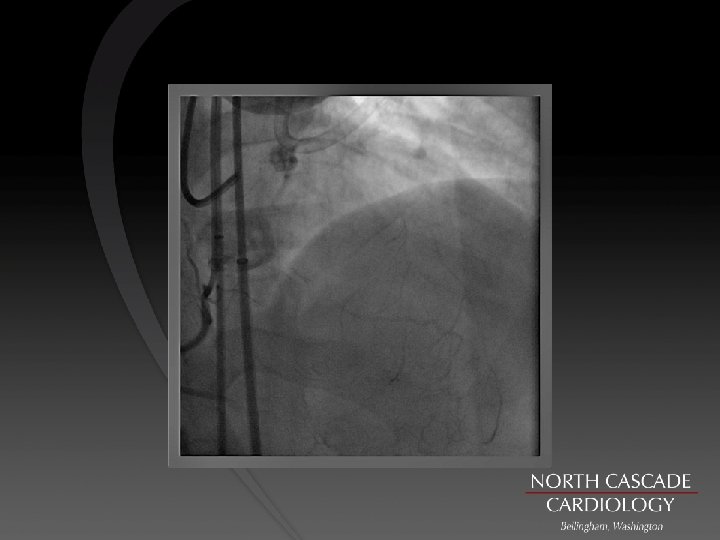
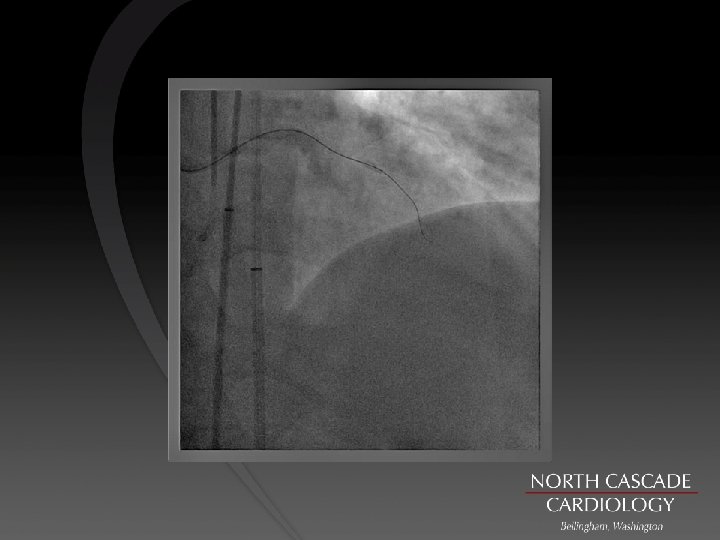
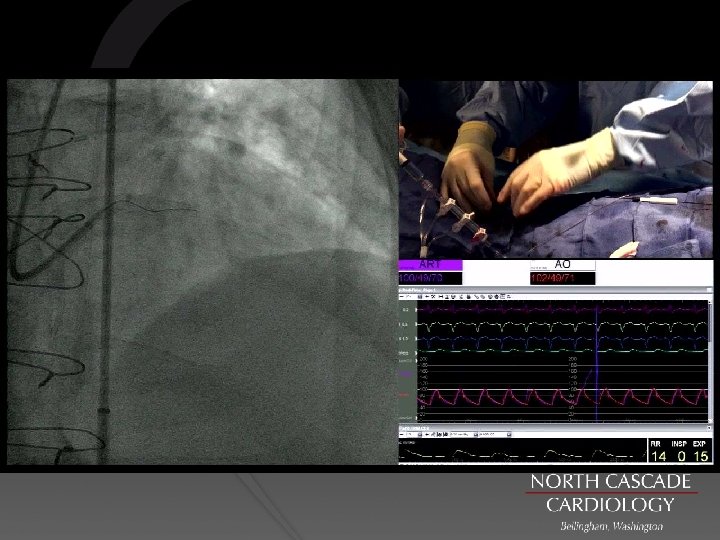
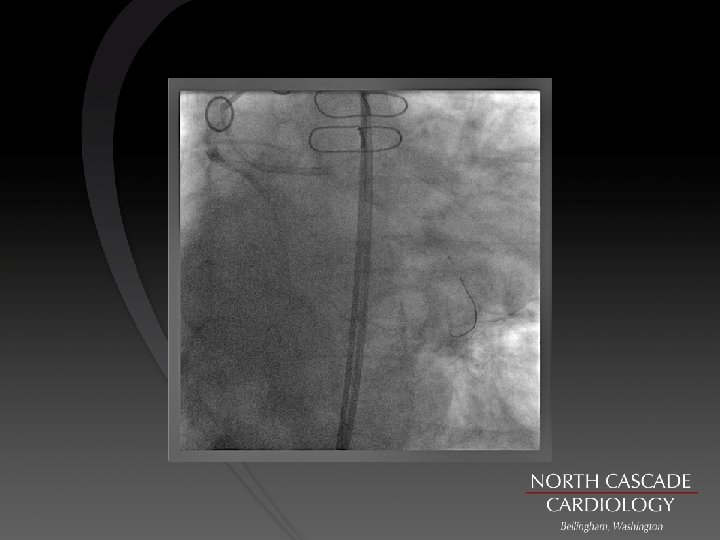
STRAW Technique Loss of retrograde filling

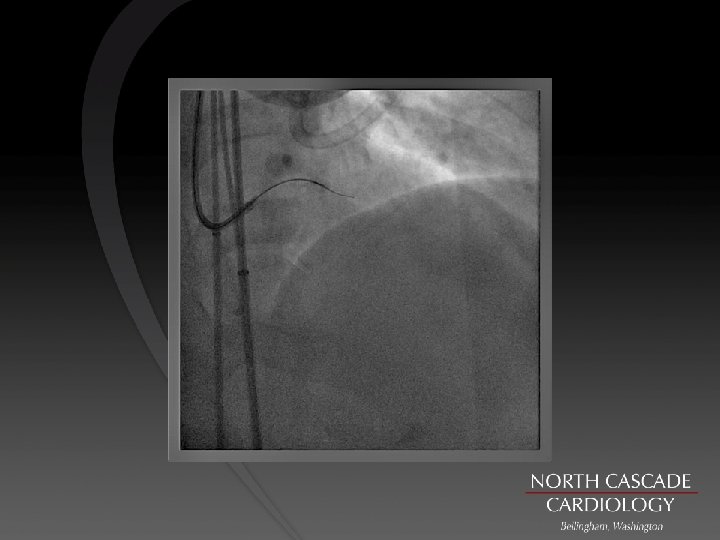
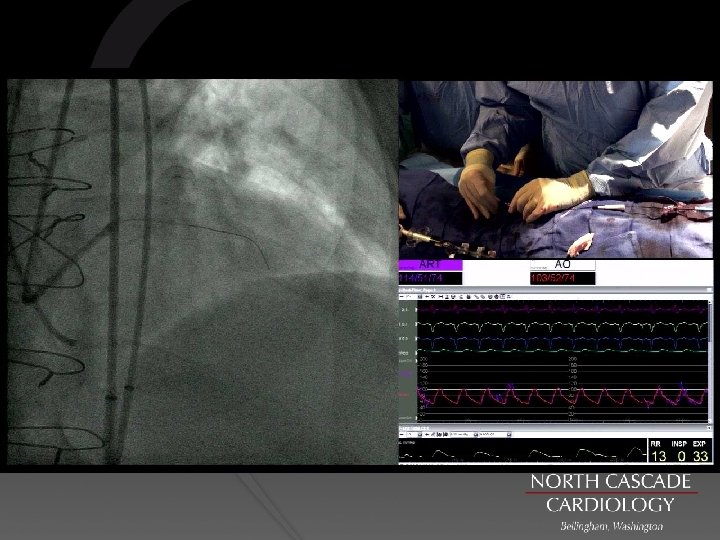
STRAW Technique Restored retrograde filling with antegrade aspiration

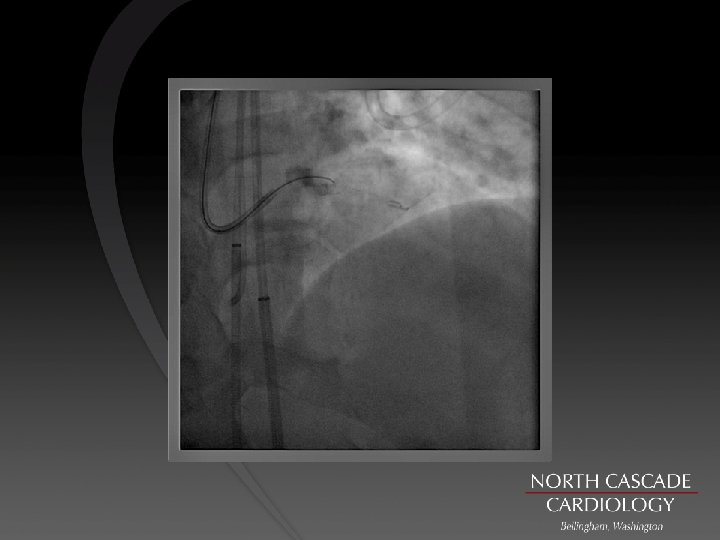
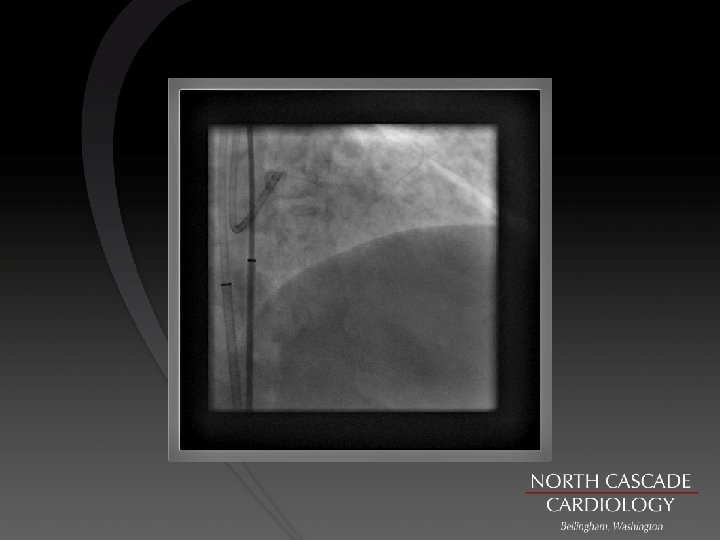
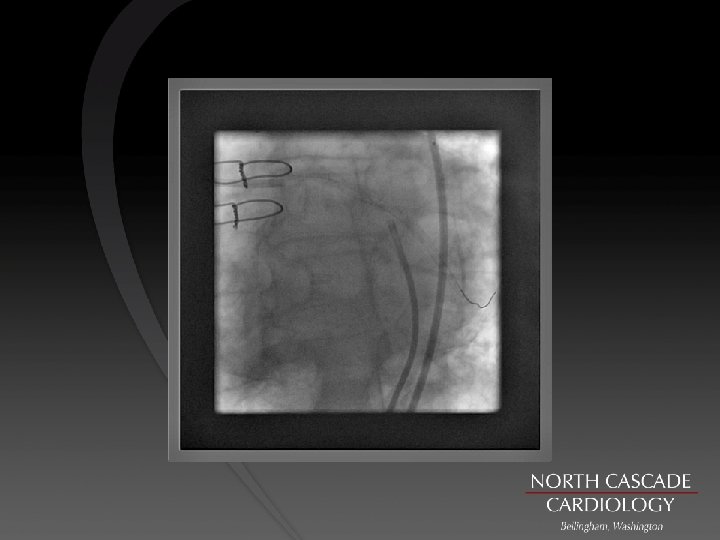
STRAW Technique Lost filling again while exchanging boss for ray

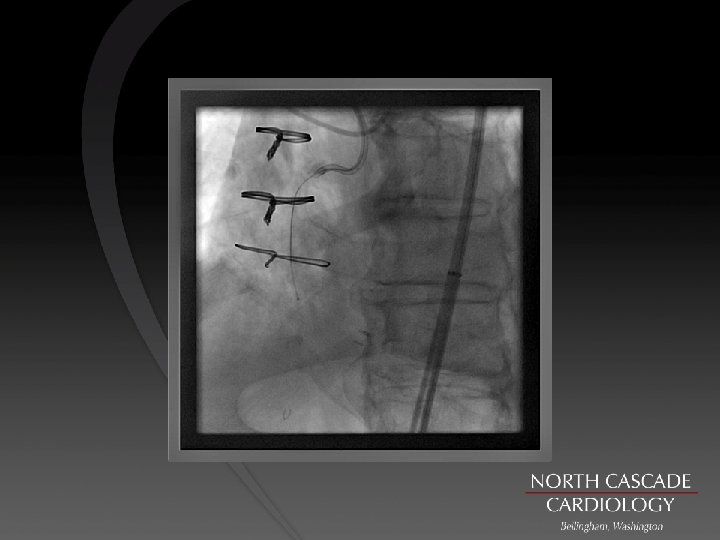
STRAW Technique RE restored filling and made stick with ray balloon deployed

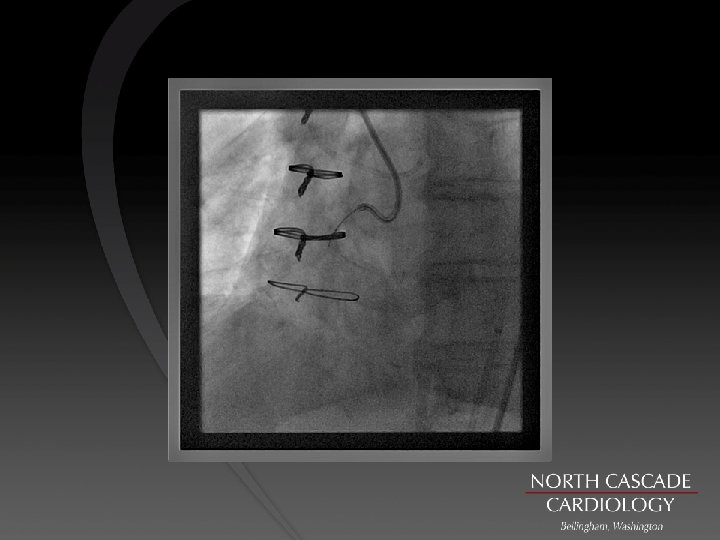
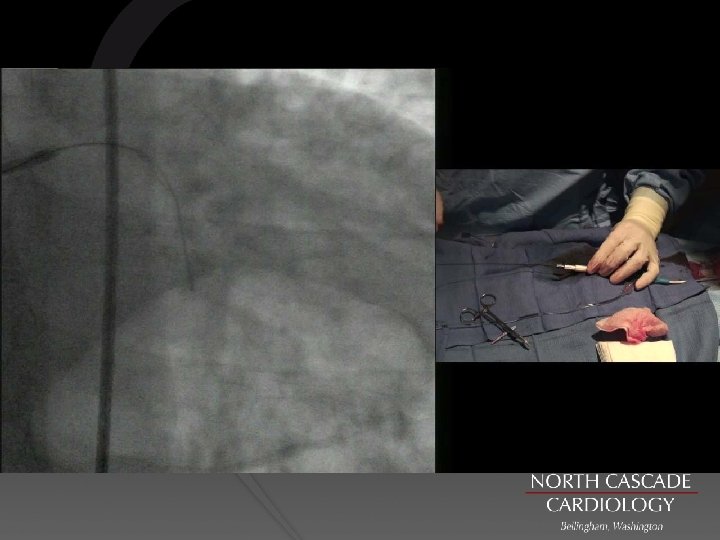
STRAW Technique Ballooning over workhorse wire

STRAW Technique Final result

Key points n Ensure you are in vessel architecture before bringing otw gear in. n How you cross CTO segment is irrelevant (wire, knuckles or crossboss) n Managing the landing/re-entry zone with very controlled small dissections. (Preferable crossboss or can use 1. 25/1. 5 balloons making just big enough channel to deliver the stingray balloon to re-entry site n In diffusely diseased vessels make re-entry with stingray wire but don’t hesitate to swap to polymer wire to wire the distal vessel as the design of stingray makes it very difficult to wire the native vessel. n www. ctofundamentals. org

- Slides: 48