Tips and Tricks in Overcoming Difficult Radial Access















































- Slides: 48
Tips and Tricks in Overcoming Difficult Radial Access Anatomic Problems Masters Sessions in Transradial Intervention II February 24, 2020 Michael A. Kutcher, MD, FACC, FSCAI
Michael A. Kutcher, MD I have no relevant financial relationships
Michael A. Kutcher, MD, FACC, FSCAI Interventional Cardiology Wake Forest Baptist Medical Center Winston-Salem, North Carolina
Objectives • Review standard procedures to assure effective radial access • Discuss various scenarios of radial vascular access misadventures and strategies to overcome
IT STARTS AT THE BEGINNING
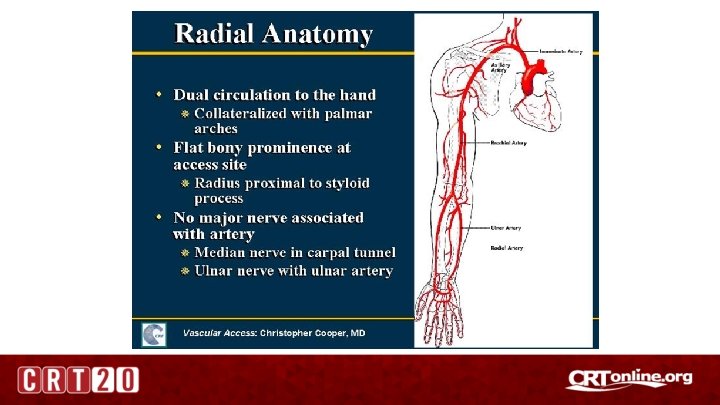
Safety of Procedure: Dual Blood Supply + Patent Palmar Arch
Radial Access Equipment Tam M, Medscape
Radial Access Technique Gentle hyperextension of hand to better expose radial bed Palpate for the radial artery. Aim for 2 cm proximal to the radial styloid process Tam M, Medscape Ultrasound guided entry should a standard of practice !!!
Radial Access Technique Ultrasound guided entry should a standard of practice !!! Puncture at 45 degree angle. Advance slowly until pulsatile backflow. Then go a bit beyond. Slowly bring needle back until pulsatile flow. Gently feed guide wire through needle. Bring needle back slightly if resistance. Change angle of entry if resistance. Advance wire carefully. Tam M, Medscape
Radial Access Technique Once radial sheath verified intraluminal • IA verapamil • Sheath wires: – Versacore 0. 035 x 145 in preloaded Tiger – 0. 035 Tight J 260 cm – 0. 035 Angled Terumo 300 cm – 0. 014 BMW wire • Verify long wire position with fluoroscopy
Radial Access Technique • Once sheath in place - never force wires – if resistance reassess location. • Arm pain is a sign of vascular problems. • Radial angiography with 50: 50 contrast saline solution via an A 2 MP catheter if radial/brachial issues.
ABERRANT RADIAL ARTERY
Aberrant Radial Artery • Suspect if patient has shoulder pain or there is difficulty in exchanging for a larger size guiding catheter. • Try smaller caliber catheters. • If you cannot resolve the issue – may have to pull back and do angiogram with A 2 MP catheter to see where you may be.
Aberrant Radial Artery • Once done you may have to re-enter the true radial-brachial branch. • If unable – you may have to switch to another vascular access site.
POOR RADIAL ACCESS ULNAR ALTERNATIVE
Access Strategy • Since right palmar arch intact – and right radial etreitic – decided on right ulnar approach • Standard access with 5 F sheath and diagnostic catheters – no technical issues.
Coronary Angiography and Left ventriculogram
Brachial/Radial Angiography with 5 F A 2 MP
Radialist Learning Points • Ulnar artery access is an alternative if radial pulses are poor • Make sure palmar arch reasonably intact • It would be wise to take an angiogram at the end of the case to assure no major issues.
RADIAL LOOP
Procedural Issues • Successful right radial access and 5 F sheath inserted • However – there was resistance at mid forearm level with 0. 035 tight J wire • Radial angiogram performed via 5 F sheath
Radial Angiography with 5 F A 2 MP
Procedural Issues • No problemo !!!! • Plan to traverse radial loop with 0. 014 BMW wire.
0. 014 BMW across Radial Loop
Procedural Issues • Still no problem !!! • Advance traverse catheter over BMW wire and exchange for angled Turomo • Then advance 5 F A 2 multipurpose catheter over stiffer Turomo
Terumo and A 2 MP approaching Radial Loop
Procedural Issues • Problem: Cannot overcome angles • Concerned about damaging radial loop even if able to cross catheter • Abandoned right radial • TR band applied • Right femoral previously prepped and ready to go
Radialist Learning Points • If you encounter a severe radial loop – should you even go on to try to circumvent it? • Concerned about damaging radial loop with catheter maneuvers even if able to cross. • This could be exacerbated higher caliber PCI guide catheters. • Option - “take a knee” if faced with a radial loop – go on to the femoral or other radial.
ABERRANT RIGHT SUBCLAVIAN
Procedural Issues • • Access via right radial artery with 5 F sheath Difficult to access right subclavian Variety of wires: Tight J. 035 Versacore modified J. 035 Glide wire Contrast injection with 5 F A 2 multipurpose
Procedural Strategy • • Patient stable – no pain – hemodynamics OK Transitioned to right femoral artery access Aortic root injection Proceeded with diagnostic coronary angiography and LV gram
Ascending Aortogram • Arch vessels clearly outlined, with aberrant right subclavian artery insertion posterior and slightly distal to left subclavian artery • Flow noted into aberrant vessel • Patient with intact right arm pulses
Coronary Angiogram • Left dominant circulation • Normal coronary anatomy • Staining of vessel still noted
Left Ventriculogram
CTA Chest Day 1
Aberrant Right Subclavian Artery • Normal anatomic aortic arch: three supra-aortic trunks: brachiocephalic, left carotid, left subclavian • 0. 07 - 0. 2% incidence where right subclavian is distinct from the right carotid and originates in the descending aorta distal to the left subclavian artery. • Described by Hunald in 1935 – termed lusorian artery • Predominance in females
Aberrant Right Subclavian Artery
Aberrant Right Subclavian Artery • 80% incidence of path posterior to esophagus • 15% between esophagus and trachea • 5% anterior to trachea Term: dysphasia lusoria
Aberrant Right Subclavian Artery Kommerell Diverticulum • Incidence 20 -60% • Increasing incidence of type A dissection • Consider surgical repair if diameter > 3 cm above level of orifice and > 5 cm in depth
Radialist Learning Points • Recognize this as a possible entity whenever encountering difficulty in accessing ascending aorta via a right radial approach • Use variety of delivery wires including tight J, angled Versacore, or hydrophilic wires • Do not force the issue • Take angiogram if aortic waveform confirmed and use pigtail or angled A 2 multi-purpose catheter
Radialist Learning Points Catheter crossing the midline in AP view signals a possible aberrant right subclavian artery
Radialist Learning Points Do aortogram to confirm presence or absence of aberrant position of right subclavian
Radialist Learning Points • If aberrant right subclavian artery is confirmed and no Kommerell diverticulum is seen – may continue gentle wire access - but be very careful • If successful entry into ascending aorta – maintain wire position in aorta at all cost • Realize that any catheter manipulation will be difficult • Would be best to stop at diagnostic – reserve PCI for another day with another access.
Radialist Learning Points • If aberrant right subclavian artery is confirmed and if Kommerell diverticulum is seen – then transition to an alternative arterial access – either left radial or femoral. • If there is ANY doubt as to anatomy – then transition to an alternative access route. • Based on my experience transition to an alternative access route is the better option
Conclusions • Know your radial, brachial, and arch anatomy and the potential variations • Never force a guide wire or catheter • Always listen to the patient • Think spatially to resolve problems • Keep thinking ahead of options if your current strategy is not working
Thank You !!! Questions ? ?