Time is Brain Tissue Ischaemic core brain tissue
 Penumbra (salvageable brain")
Time is Brain Tissue Ischaemic core (brain tissue destined to die) Penumbra (salvageable brain area) An untreated patient loses approximately 1. 9 million neurons every minute in the ischaemic area Reperfusion offers the potential to reduce the extent of ischaemic injury Saver. Stroke 2006; 37: 263 -266. González. Am J Neuroradiol 2006; 27: 728 -735. Donnan. Lancet Neurol 2002; 1: 417 -425.



Time is brain!
, with")
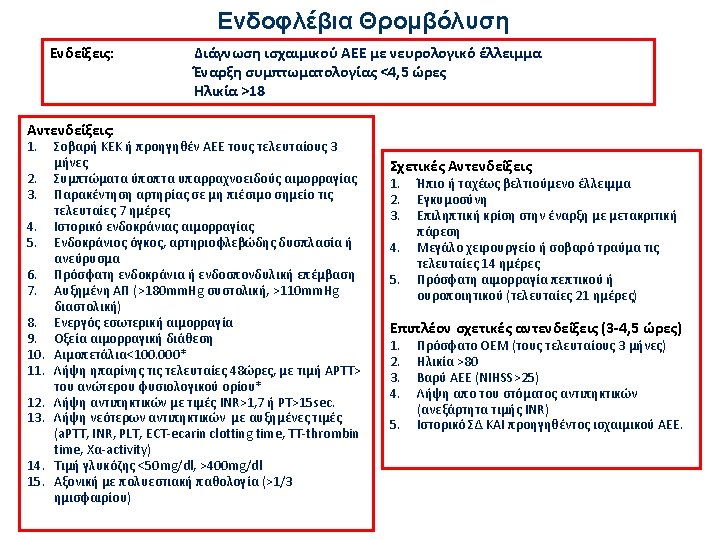
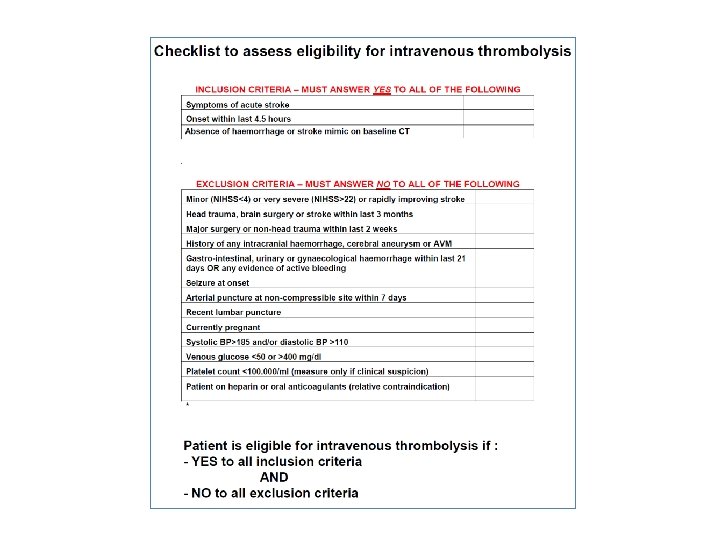
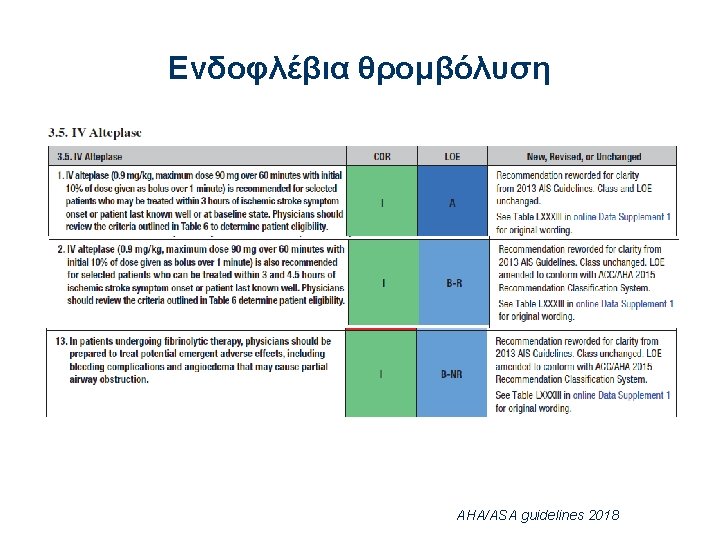
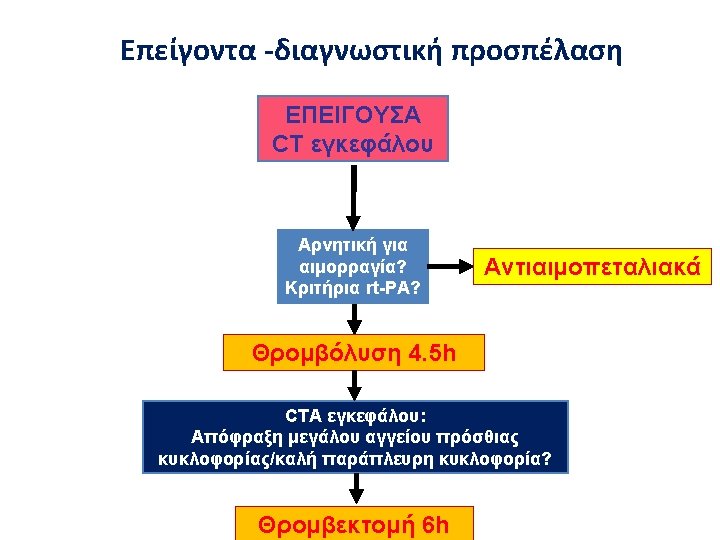
• Recommendations: thrombolysis Intravenous rt-PA (0. 9 mg/kg BW, maximum 90 mg), with 10% of the dose given as a bolus followed by a 60 -minute infusion, is recommended within 4. 5 hours of onset of ischemic stroke (Class I, Level A)

Οδηγίες θρομβόλυσης AHA/ASA guidelines 2018

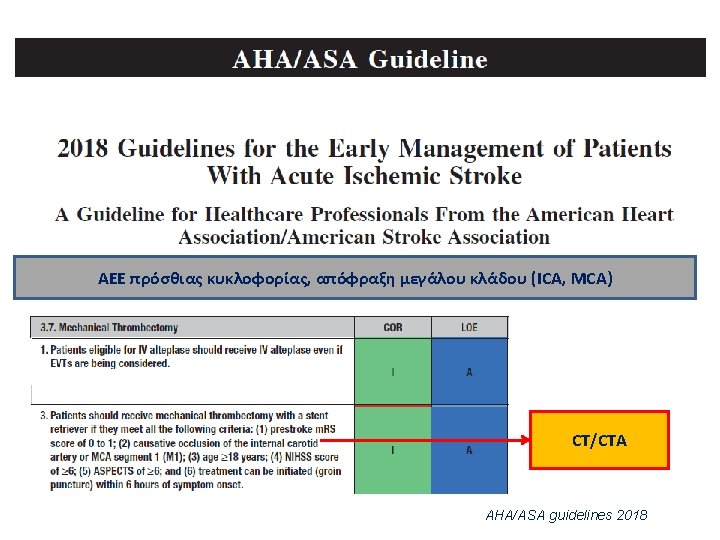
Mechanical thrombectomy with a stent retriever criteria 1. prestroke m. RS score of 0 to 1 2. causative occlusion of the internal carotid artery or MCA segment 1 (M 1) 3. age ≥ 18 years 4. NIHSS score of ≥ 6 5. ASPECTS of ≥ 6 6. treatment can be initiated (groin puncture) within 6 hours of symptom onset. AHA / ASA Guidelines 2018

ΝΝΤ = 2. 8 Stent retriever technique Aspiration technique

Thrombectomy: CTA

Panagiotis Papanagiotou, Interventional Cardiology Clinics, 2014

DVT prevention Low dose heparin Recommendations § Low-dose s. c. heparin or low molecular weight heparins should be considered for patients at high risk of DVT or pulmonary embolism (Class I, Level A) ESO 2008 Subcutaneous administration of anticoagulants is recommended for treatment of immobilized patients to prevent DVT (Class I; Level of Evidence A). AHA / ASA 2014 Συσκευές περιοδικής συμπίεσης (Class OR I, LOE B-R) LMWH “not well established” (Class OR IIb, LOE A) ΑΗΑ/ASA Guidelines, Stroke. 2018; 49: e 46–e 99


Χορήγηση Ασπιρίνης • Administration of aspirin is recommended in patients with AIS within 24 to 48 hours after onset. For those treated with IV alteplase, aspirin administration is generally delayed until 24 hours later but might be considered in the presence of concomitant conditions for which such treatment given in the absence of IV alteplase is known to provide substantial benefit or withholding such treatment is known to cause substantial risk. (Class I, Lo. E A) AHA/ASA guidelines 2018

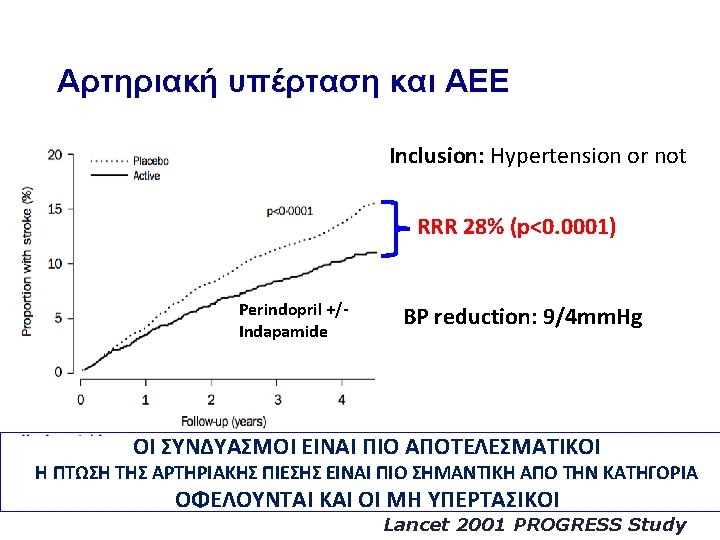
Acute IS and SAP on admission The Athens Stroke Outcome Project >140 mm. Hg: 75% >180 mm. Hg: 21% N=2160 Up to 80% of acute ischemic stroke patients have elevated BP on admission

Spontaneous decrease of blood pressure in patients with acute stroke Wallace et al. JAMA 1981

Krishman K et al. Stroke. 2015.

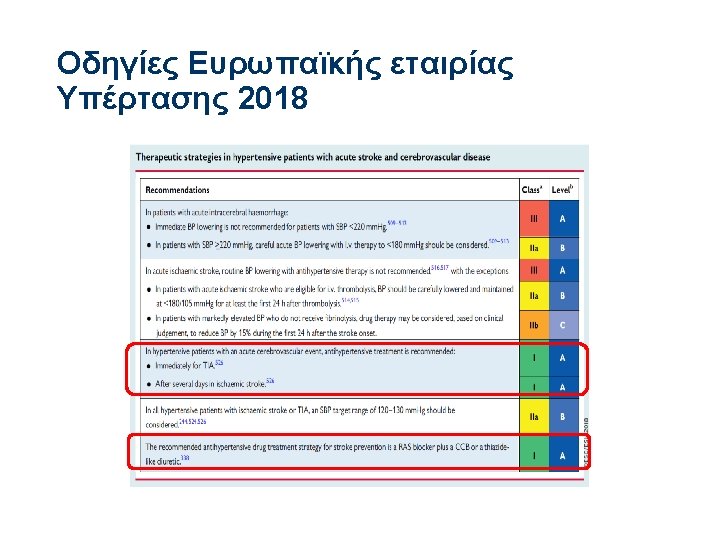
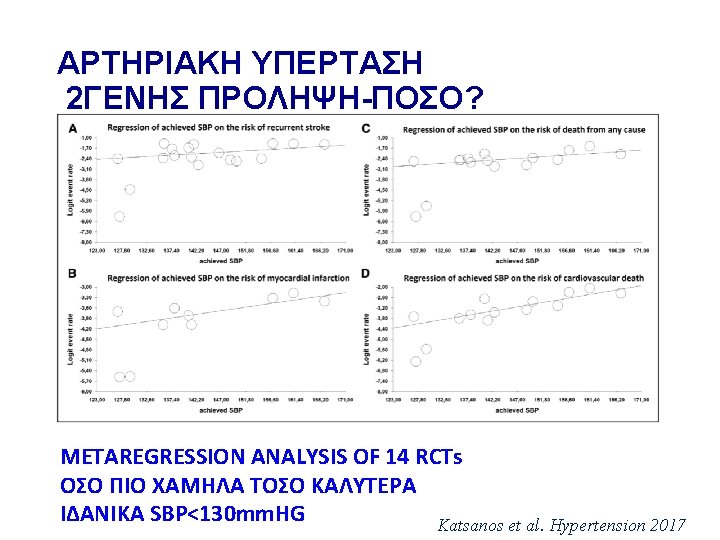
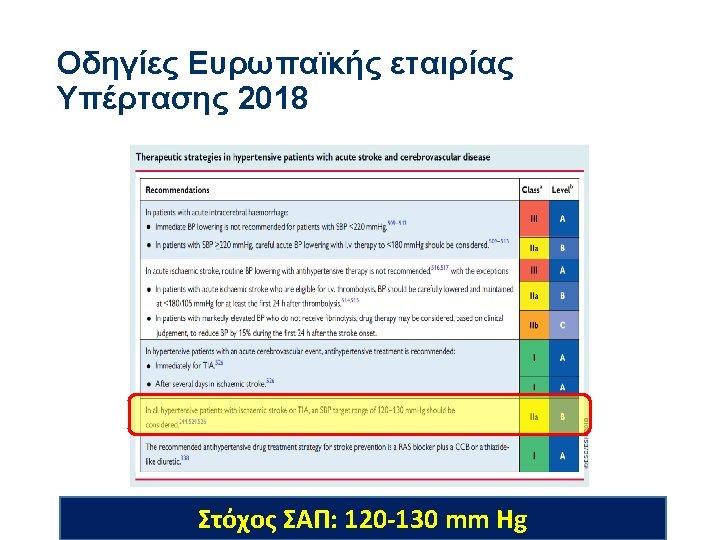
Management of HTN in acute IS Whelton et al. , Hypertension 2017; AHA/ASA guidelines 2018
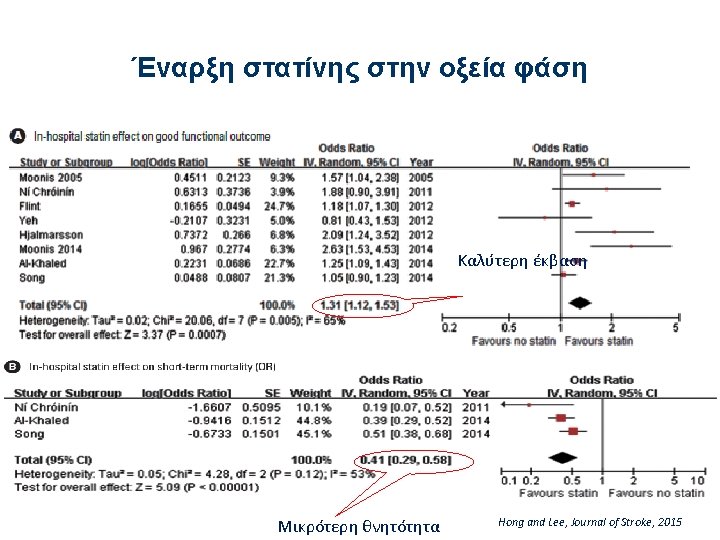

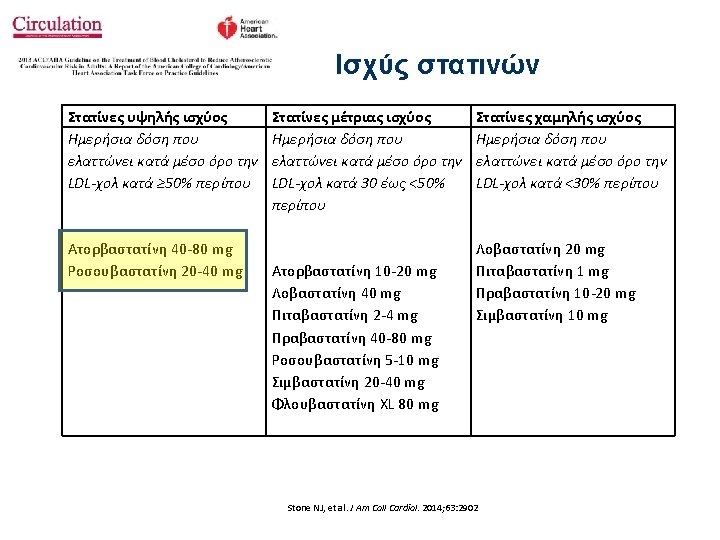
Χορήγηση στατίνης στην οξεία φάση του ισχαιμικού ΑΕΕ • Among patients already taking statins at the time of onset of ischemic stroke, continuation of statin therapy during the acute period is reasonable. (Class IIa, Lo. E B) • High-intensity statin therapy should be initiated or continued as first-line therapy in women and men ≤ 75 years of age who have clinical ASCVD*, unless contraindicated. (Class I, Lo. E A) • In individuals with clinical ASCVD* in whom high-intensity statin therapy would otherwise be used, when high-intensity statin therapy is contraindicated or when characteristics predisposing to statin-associated adverse effects are present, moderate-intensity statin should be used as the second option if tolerated. (Class I, Lo. E A) ΑΗΑ/ASA Guidelines, Stroke 2018

Anticoagulants in the acute phase of cardioembolic ischemic stroke Meta-analysis of 7 RCTs 4624 patients • Non significant reduction in IS recurrence • Similar rate of death or disability • Significant increase in ICr. H Intracranial bleeding Paciaroni, Stroke 2007

Secondary stroke prevention 2016 ESC Guidelines Recommendation Anticoagulation with heparin or LMWH immediately after an ischemic stroke is not recommended in AF patients. Class III (harm), Level A
 Clinical factors Repeat scan 1 -3 -6 -12 rule")
Stroke severity (NIHSS) Clinical factors Repeat scan 1 -3 -6 -12 rule

NOACs: Efficacy and safety Ruff et al. , Lancet 2014

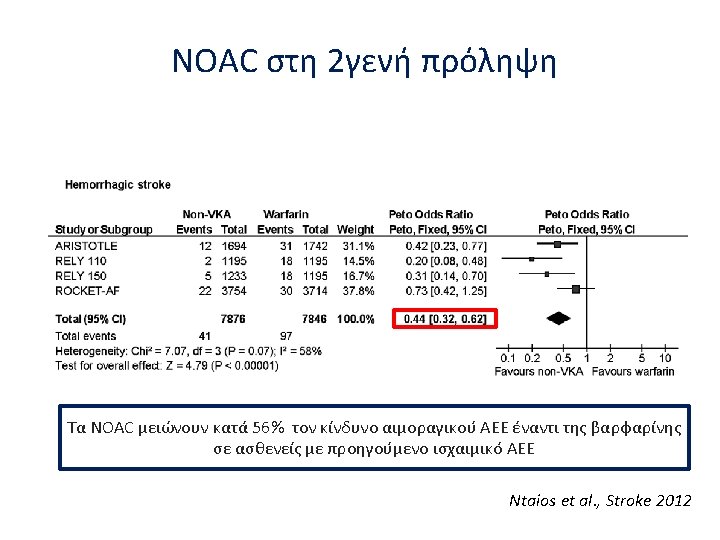
NOACs in secondary stroke prevention Ntaios et al. , Stroke 2012

Secondary stroke prevention- 2016 ESC Guidelines Recommendation NOACs are recommended in preference to VKAs or aspirin in AF patients with previous stroke Class I, Level B

When should we start anticoagulants?
 32% stroke")
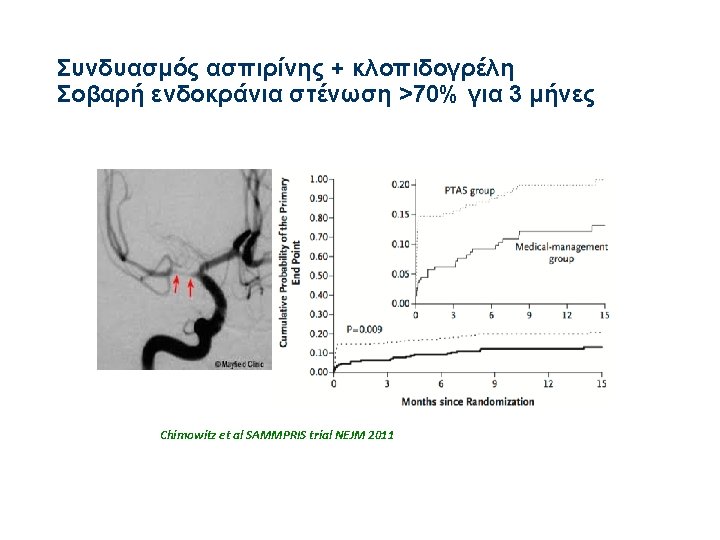
Clopidogrel+ Aspirin in High-Risk Patients with Acute non-disabling Ischemic Stroke (CHANCE study) 32% stroke recurrence reduction 31% Stroke, ΜΙ, Cardiovascular Death International Stroke Conference, Feb, 2013 N Engl J Med 2013; 369: 11 -9
 and high")
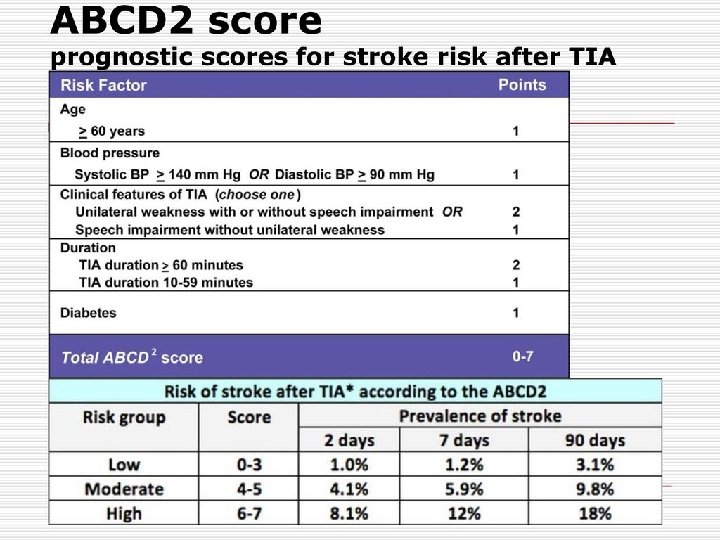
POINT trial: Results 4881 patients, 269 international sides Minor IS (NIHSS≤ 3) and high risk TIA (ABCD₂ score≥ 4) ASA+clopidogrel 75 (loading 600 mg) vs. ASA+placebo Primary efficacy outcome: Composite major ischemic events (IS, MI, vascular death) at 90 days Primary safety outcome: Major bleeding at 90 days

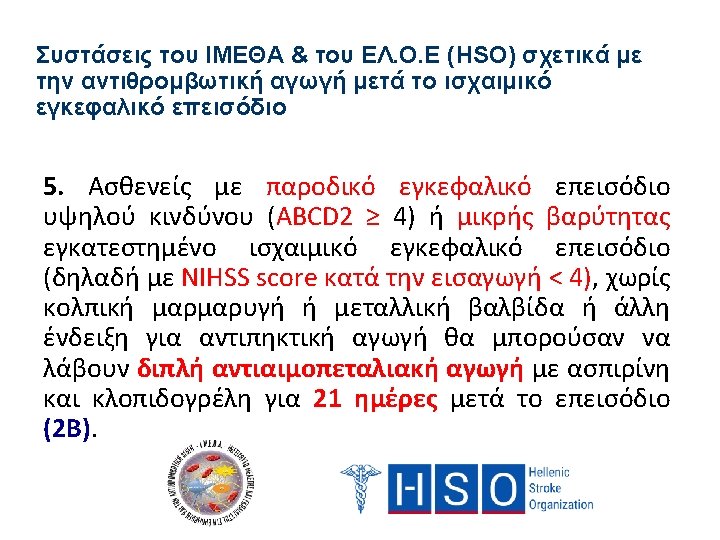
The combination of Aspirin and Clopidogrel might be considered for initiation within 24 hours of a minor ischemic stroke or TIA and for continuation for 21 days (Class IIb; Level of Evidence B). (New Recommendation) Stroke. 2014; 45: 2160 -2236; originally published online May 1, 2014;

Thank you and…. Keep safe!
- Slides: 74