THYROTOXICOSIS AND INFERTILITY An overview DR Abdul Wassay

THYROTOXICOSIS AND INFERTILITY An overview DR Abdul Wassay sultani MD
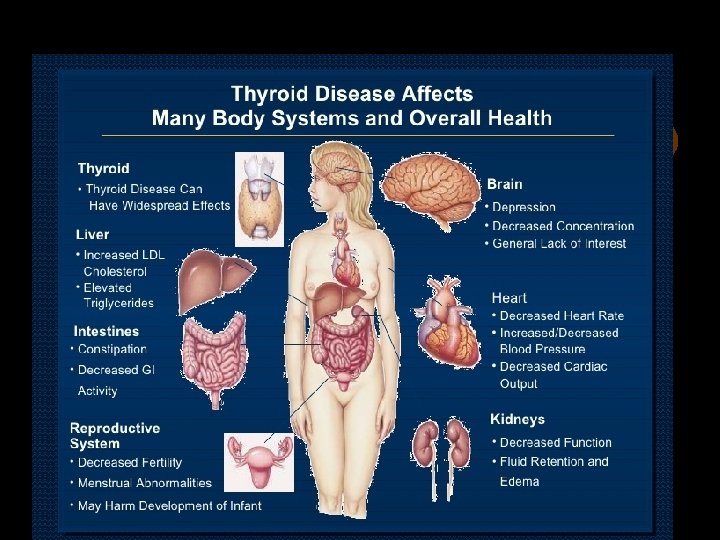

Thyrotoxicosis • Defined as the clinical, physiologic, and biochemical findings that result when the tissues are exposed to, and respond to, excess thyroid hormone. • Rather than being a specific disease, thyrotoxicosis can originate in a variety of ways. • RAIU is subnormal

Hyperthyroidism • Denotes only those conditions in which sustained hyperfunction of the thyroid gland leads to thyrotoxicosis. • Increased RAIU is the hallmark.

Varieties of Thyrotoxicosis • Associated with • Not associated with thyroid hyperfunction: • Excess production of • Disorders of hormone TSH(rare) storage-Eg: Subacute thyroiditis, chronic • Abnormal thyroiditis stimulator-Eg: Graves’ disease • Extrathyroid source of hormone- • Intrinsic thyroid Thyrotoxicosis autonomyfactitia, ectopic thyroid Eg: Hyperfunctioning tissue- struma ovarii, adenoma, Toxic functioning follicular multinodular goitre Ca.

Hyperthyroidism Graves’ disease • Also known as Parry’s or Basedow’s disease. • Graves’ disease is a disorder with three major manifestations: • 1)Hyperthyroidism with diffuse goitre • 2)Ophthalmopathy and • 3)Dermopathy. • These three manifestations may not appear together.

• In women with hyperthyroidism hormonal changes effecting reproductive system may occur. • androstenedione and testosterone production increase in hyperthyroidism and subsequently this leads to elevation of estron and estradiol. • Both this mechanism and decrease in metobolic clearance of estrogen lead to higher plasma estrogen levels in women with hyperthyroidism. Also some authors have stated that they detected elevation in serum LH, FSH and SHBG levels.

Incidence and prevalence • Relatively common disease that can occur at any age • More common in the 3 rd and 4 th decade • Disease is more frequent in women(7: 1) • Genetic factors play a important role • An overlap exsists with other autoimmune diseases suggesting Graves is also a autoimmune thyroid disease

• • Hyperthyroidism is ten times more common in women than in men and can cause a woman to have difficulties in not only getting pregnant, but also staying pregnant.

• Infertility incidence is about 5 -8% in women with hyperthyroidism. Even though in some studies endometrial biopsies proved that women were ovulating, it’s still emphasized that hyperthyroidism is related with reduced fertility. in a study performed in 2002 have reported that suppressed serum TSH levels are more frequent in positive infertile • Karaca N et al. Int J Res Med Sci. 2015 Jun; 3(6): 1299 -1304 International Journal of Research in Medical Sciences | June 2015 | Vol 3 | Issue 6 Page 1302

• • women compared to non-positive ones. Previously menstrual disorders including particularly oligomenorrhea was reported as 50% in people with Hyperthyroidism.

How thyroid hormones impact female fertility • Thyroid hormones interact with your reproductive hormones, estrogens and progesterone, to preserve normal function of the ovaries and maturation of the egg (oocyte). If your thyroid gland releases of too much (hyperthyroidism) or too little (hypothyroidism) thyroid hormones, the balance of reproductive hormones can be impaired with consecutive thyroid-related fertility problems such as ovulation disorders, irregular periods, and trouble getting pregnant or carrying a baby to term

Key symptoms of Thyrotoxicosis Irritability Fast heart rate Weight loss Trembling hands Prominent, staring eyes Increased sensitivity to heat Fast growing fingernails Hair loss Thin and smooth skin Frequent bowel movement Abnormal menstrual periods Complete absence of your monthly cycle

Clinical features • The clinical manifestations include those that reflect the associated thyrotoxicosis and those specifically related to Graves’ disease • One of the more common symptoms of hyperthyroidism is a disruption in female menstrual cycles. It may actually stop ovulation, either sporadically or completely

• • Hyperthyroidism Fertility Issues are Not for Women Only • Male fertility can be affected by a thyroid condition as well.

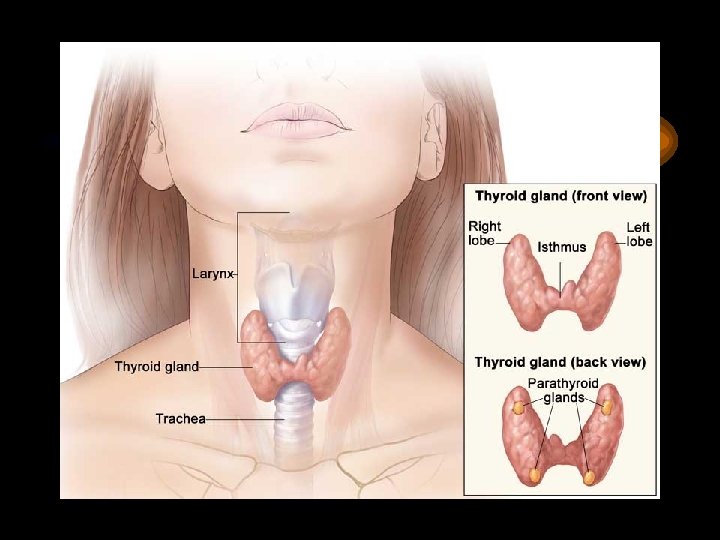
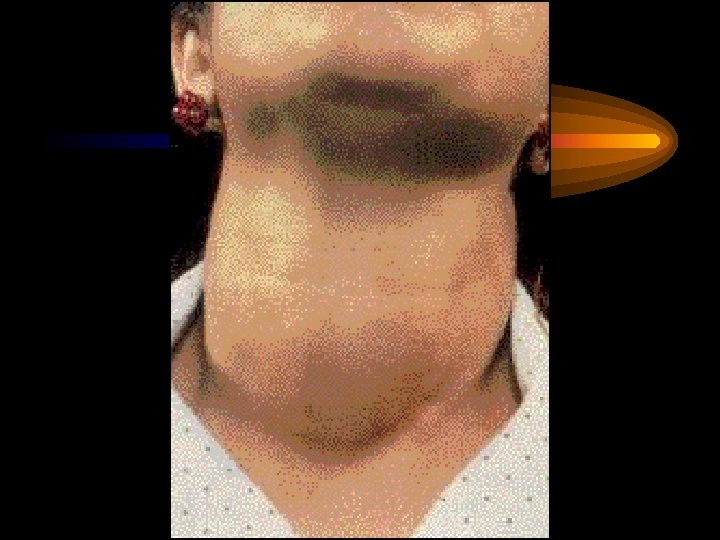
Goiter • Is diffuse and toxic and maybe asymetric and lobular. • There may be presence of bruit over the goiter


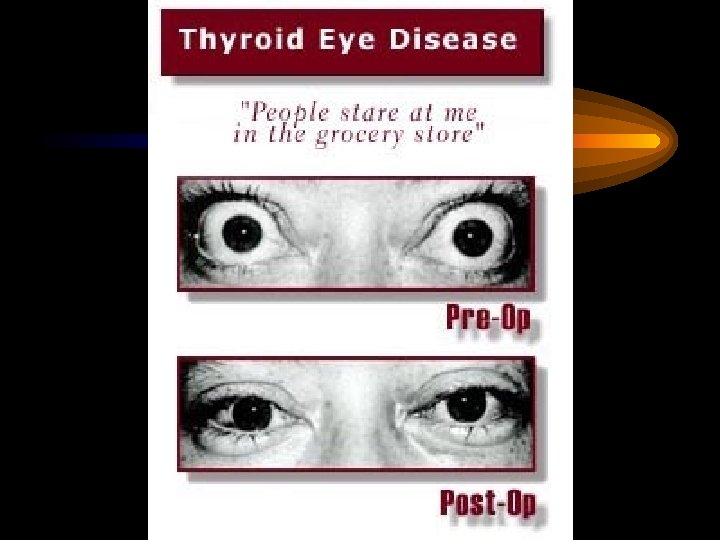
 Spastic:")
Ophthalmopathy • Signs of Graves’s ophthalmopathy are divided into two components: • 1) Spastic: Stare, lid lag and lid retraction which account for the “frightened” facies. • 2) Mechanical: Proptosis of varying degrees, ophthalmoplegia, and congestive occulopathy characterized by chemosis, conjunctivitis, periorbital swelling and the potential complications of corneal ulceration, optic neuritis and optic nerve atrophy.



Dermopathy • Usually occurs over the dorsum of the legs or feet and is termed localized or pretibial myxedema. • It is usually a late phenomenon • The affected area is usually demarcated from the normal skin by being raised andthickened and having a peau d’ orange appearance; it may be pruritic and hyperpigmented. • The most common presentation is non pitting oedema, but lesions maybe plaque like, nodular or polypoid. • Clubbing of the fingers and toes accompanies and is termed thyroid acropachy





Investigations • • • Thyroid function test: TSH- Undetectable T 4 - Raised T 3 - Raised RAIU- Raised TSH-receptor antibodies(TRAb)-elevated in Graves’s disease • Isotope scanning- Increased uptake

Treatment of Hyperthyroidism

• The best way to treat the infertility issues caused by hyperthyroidism is to get the disease under control so your metabolism works properly. In some cases additional help may also be required to restart ovulation.

Anti thyroid drugs • Chemically block hormone synthesis • Enhance evolution to remission • Best indicated for children, adolescents, young adults and pregnant women. • Propylthiouracil-100 -150 mg every 6 or 8 hrs • Carbimazole- 40 -60 mg daily initially for 3 weeks, then reduce to 20 -40 mg for another 8 weeks and maintain at 5 -20 mg daily for 18 -24 months. • Methimazole-active metabolite of Carbimazole

Duration of treatment • 18 -24 months • Side effects- Rash Leukopenia Agranulocytosis

Control of adrenergic symptoms • Adrenergic antagonists: • Propranolol-40 -120 mg/day
Cardiac- Heart failure Atrial fibrillation • 2)Thyrotoxic crises: or ‘storm’:")
Complications of thyrotoxicosis • 1)Cardiac- Heart failure Atrial fibrillation • 2)Thyrotoxic crises: or ‘storm’: • Fulminating increase in signs and symptoms of thyrotoxicosis. • Occurs in medically untreated or inadequately treated patients. May be precipitated by surgery or sepsis • The syndrome is characterized by extreme irritability, delirium or coma, fever 41°C or more, tachycardia, restlessness, hypotension, • vomiting and diarrhea.

Treatment of thyroid crisis • • • Provide supportive care; Treat dehydration Administer glucose and saline Vitamin B complex and glucocorticoids Digitalization is required in those with atrial fibrillation Immediate and large doses of anti thyroid agents(Eg-propylthiouracil 100 mg every 2 h) Iodine intravenously or by mouth Propranolol 40 -80 mg every 6 h Dexamethasone(2 mg every 6 h) and to be tapered later.

Thanks THANKS
- Slides: 38