Thyroid disorders Dr Enas Abusalim Thyroid physiology The

Thyroid disorders Dr Enas Abusalim

Thyroid physiology • The hypothalamic –pituitary –thyroid axis • And peripheral conversion of T 4 to T 3 , WHERE , AND BY WHAT ENZYME ? ? • Only relatively small concentrations of T 4 and T 3 are biologically active , WHY ? • WHAT IS THE DAILY REQIUREMENT OF IODIDE IN ORDER TO MAINTAIN NORMAL THYROID FUNCTION ?
,")
Common presentations in thyroid diseases • Enlargement of the thyroid gland ( goiter ), • Incidental finding of abnormal thyroid function test , • Symptomatic hypothyroidism or hyperthyroidism.

Who should be tested for abnormal thyroid function ?

Who should be tested for abnormal thyroid function ? • Patients with signs and symptoms of either hypothyroidism or hyperthyroidism , WHICH ARE ? • All pregnant patients as a routine screen during booking visit , • Goiterous enlargement of thyroid gland , • In the presence of other autoimmune diseases ( INCLUDING …………. ? ? ? ) • As follow up post thyroid resection , or thyroid cancer treatment.


Hyperthyroidism • What is THYROTOXICOSIS ? ? • How does it differ from the term hyperthyroidism ? • What are the causes of hyperthyroidism ? Most common ? Graves disease Toxic multinodular goiter Toxic adenoma
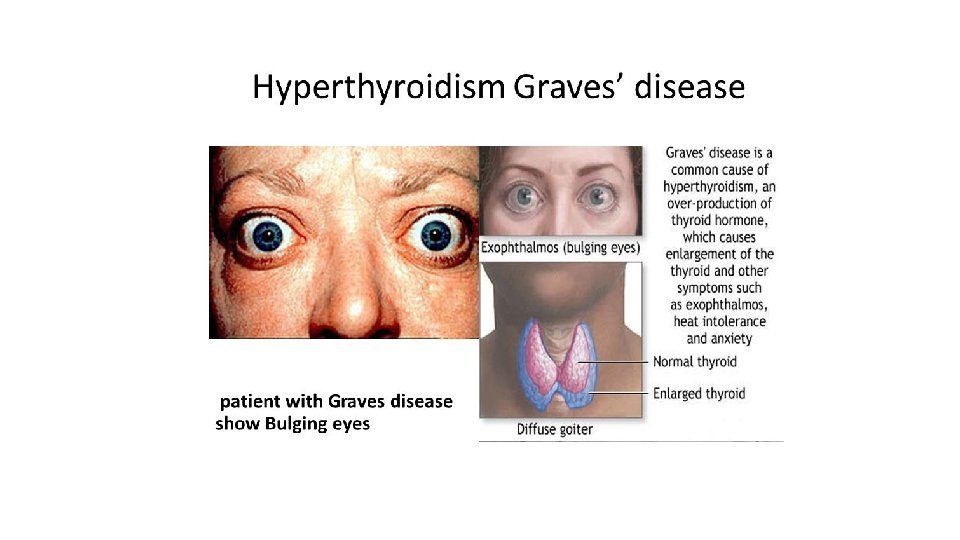


Graves disease • An autoimmune disorder • Affecting the thyroid gland ( hypersecreting and goiterous enlargement ) , periorbital fat , ocular muscles ( proptosis , diplopia , chemosis ophthalmoplegia ) , and skin ( pretibial myxedema ). • Caused by antibodies against which receptor ? ? ? • Can Graves ophthalmopathy occur in a euthyroid individual ? • Family history of autoimmune thyroid disease often present , and is a risk factor for the development of Graves.

What does physical examination of the thyroid gland reveal in Graves Disease ?

Diagnosis • TSH level is the first step in a patient who presents with signs and symptoms of abnormal thyroid function. • Normal range is variable according to age , pregnancy , but is usually between 0. 4 -4 milli-international units /L in young non-pregnant patients. • If abnormal this should be followed by measurement of T 4 levels ( not T 3 , WHY ? ? ) • Normal range of T 4 is 4. 6 -12 ug/dl • Anti –TSH receptor antibodies ( TSI , TBII ) • WHAT IS NEXT ?

For any patient with signs and symptoms of hyperthyroidism, and abnormal thyroid function test , the next step is a RAIU scan. How is it beneficial? ?

Treatment of hyperthyroidism • For Graves disease treatment options are : üAntithyroid drugs , üRadioactive iodine ablation of the thyroid gland , ( any contra-indications ? ? ). üAnd thyroid surgery. In addition to symptomatic relief by beta-blocker therapy to suppress excess adrenergic tone ( propranolol for example , which has the additional benefit OF ? ? ? ) • How should treatment be monitored after initiation of management ? ? • What is the expected outcome of radioactive iodine ablation of the thyroid gland in graves disease ? ?

Treatment of multinodular goiter and solitary thyroid nodule • What is the gold standard treatment option , and how does it differ from treatment of graves disease post treatment ? ? ? • What is Jod-Basedow phenomenon ? • What are the indications of thyroidectomy in a hyperthyroid patient ? ? • If a cold thyroid nodule was found in a RAIU done for multinodular goiter what would be your next best investigation ?

Hypothyroidism • The most common cause is ? ? ? Other causes ? ? • Name possible medications known to cause hypothyroidism ? ? • How does an associated coeliac disease effect the management of a hypothyroid patient ?

Hashimotos thyroiditis • An autoimmune disorder caused by antibodies against TPO , and thyroglobulin. • Signs and symptoms ? ? • How does it affect blood pressure and lipid profile ? • Tendon reflexes ? ? • Is RAIU scan required ? • Is an Ultrasound required ?

Treatment of hypothyroidism • Levothyroxine therapy is the mainstay of thyroid hormone replacement , • What are the precautions you must inform your patient about while taking thyroid replacement therapy ? ?

Destructive thyroiditis • Definition : • Types : 1 - Subacute thyroiditis 2 -Silent thyroiditis 3 -post partum thyroiditis • Diagnosis : • Treatment :

Thyroid EMERGENCIES !!! Thyroid Storm And myxedema Coma

Thyroid Strom • This is a life threatening condition presenting as 1 - severe thyrotoxicosis 2 - coupled by secondary systemic decompensation Clinical presentation : • Hyperthermia • Tachycardia ( sinus or arrhythmias ) • Heart failure • Jaundice , Elevation in liver function test and fulminant hepatic failure • Diarrhea , nausea , vomiting , abdominal discomfort , • Agitation , disorientation.

• What precipitated this condition ? ? ?

• What precipitates this condition ? ? ? Surgery , Infection , Parturition , Acute iodine exposure , Radioactive iodine , Medications including salicylates and pseudoephedrine

How is it treated ? ? 1 - supportive measures , including ABCs……etc. . 2 - decreasing thyroxin production by thyroid gland , HOW ? ? 3 - decreasing peripheral conversion of T 4 to T 3 , HOW ? ? 4 - address associated adrenergic and thermoregulatory changes 5 - treat all precipitating factors 6 - aggressively reverse any systemic decompensation and organ dysfunction.

Myxedema coma • Systemic decompensation caused by severe hypothyroidism , • Caused by ? ? ?

Myxedema coma • Systemic decompensation caused by severe hypothyroidism , • Caused by ? ? ? üNon-adherence üMI , stroke üHeart failure üCold exposure üHypoglycemia üAcidosis üGI-bleeding …………. etc.

manifestations • Mental state changes ( including lethargy , stupor , psychosis m and coma ) • Hypothermia ( temp less that 34. 4 C ) • Bradycardia • Hypoventilation and type 2 respiratory failure • Hypotension • Hyponatremia ( by which mechanism ? ? ? ) • Hypoglycemia

Management 1 - supportive , including warming , ABCs…. , and management of organ dysfunction. 2 - TSH and free T 4 , and CORTISOL should be check promptly, DON’T WAITE FOR TEST RESULTS , TREAT ASAP , 3 -REPLACE CORTISOL IF DEFICIENCY IS SUSPECTED PRIOR TO REPLACEMENT OF THYROXIN , WHY? ? ? 4 -IV LEVOTHYROXINE

THANK YOU FOR LISTENING
- Slides: 29