Thyroid Cytology Atypia of Undetermined Significance Dr Mohammadnia

")







 Focal cytologic atypia (b) Extensive but mild")













 § Population of follicular cells with nuclear enlargement and")

")



 In the first edition 5– 15% In the second edition")




- Slides: 39
Thyroid Cytology Atypia of Undetermined Significance Dr. Mohammadnia Cytopathology Fellowship Shiraz University of Medical Sciences
The Bethesda System for Reporting Thyroid Cytopathology: Category III Atypia of undetermined significance (AUS) OR Follicular lesion of undetermined significance (FLUS)
Use only one term: AUS or FLUS
AUS/FLUS Specimens that contain cells with architectural and/or nuclear atypia that is not sufficient to be classified as suspicious for a follicular neoplasm, suspicious for malignancy, or malignant and the atypia is more marked than can be ascribed confidently to benign changes.
§ AUS has only fair reproducibility. § Percentage of AUS cases: Maximum 10% of all thyroid FNAs. § AUS: malignant ratio: Less than 3. 0.
Ø Specimens with cytologic atypia always are adequate. Ø Air-drying artifact, obscuring blood, and excessive clotting artifact do not warrant an AUS diagnosis. Ø Rare cases with uncertainty that the cytologic changes artifactual in origin or truly atypical should result in an AUS diagnosis.
Air-drying artifact: Follicular cells with enlarged nuclei Pale but slightly smudgy chromatin Irregular nuclear outlines Excessive blood clotting: Architectural crowding due to the entrapment of cells in the clot False impression of nuclear grooves due to fibrin strands
Atypical follicular cells with blood and air drying
Criteria of AUS 1. Cytologic atypia (a) Focal cytologic atypia (b) Extensive but mild cytologic atypia (c) Atypical cyst-lining cells (d) “Histiocytoid” cells 2. Architectural atypia 3. Cytologic and architectural atypia 4. Hürthle cell aspirates 5. Atypia, not otherwise specified (NOS) 6. Atypical lymphoid cells, rule out lymphoma
Cytologic atypia
Focal cytologic atypia Rare cells with: nuclear enlargement and irregular nuclear contours In the paucicellular aspirate or benign aspirate
Extensive but mild cytologic atypia Many cells with mildly enlarged nuclei with slightly pale chromatin and only limited nuclear contour irregularity. Nuclear pseudoinclusions are absent.
Extensive but mild cytologic atypia
Atypical cyst-lining cells § Nuclear grooves § Prominent nucleoli § Elongated nuclei and cytoplasm § Rare intranuclear pseudoinclusions Histiocytoid cells Compared to histiocytes are larger and have rounder nuclei, higher N/C ratio, and harder cytoplasm with vacuole. Cystic papillary carcinoma?
Atypical cyst lining cells
Atypical cyst-lining cells
“Histiocytoid” cells
Architectural atypia § Scantly cellular specimen with rare microfollicles or crowded three-dimensional groups and scant colloid § Focally prominent microfollicles in a moderately or markedly cellular sample. Single slide or an area of the slide is different from the rest of the aspirate. This pattern is low risk
Architectural atypia
Cytologic and architectural atypia § Mild cytologic atypia and architectural atypia § More common with NIFTP
Cytologic and architectural atypia
Hürthle cell aspirates A sparsely cellular aspirate comprised almost exclusively of Hürthle cells with minimal colloid. § A moderately or markedly cellular sample composed almost exclusively of Hürthle cells in benign clinical setting (lymphocytic thyroiditis or MNG). §
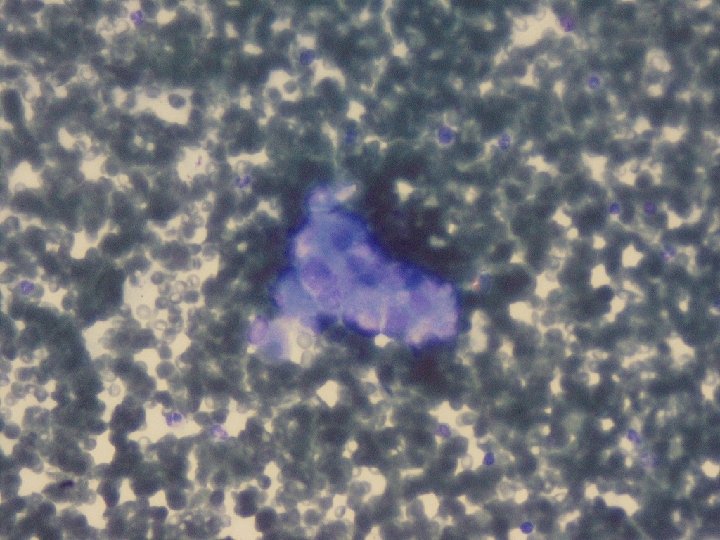
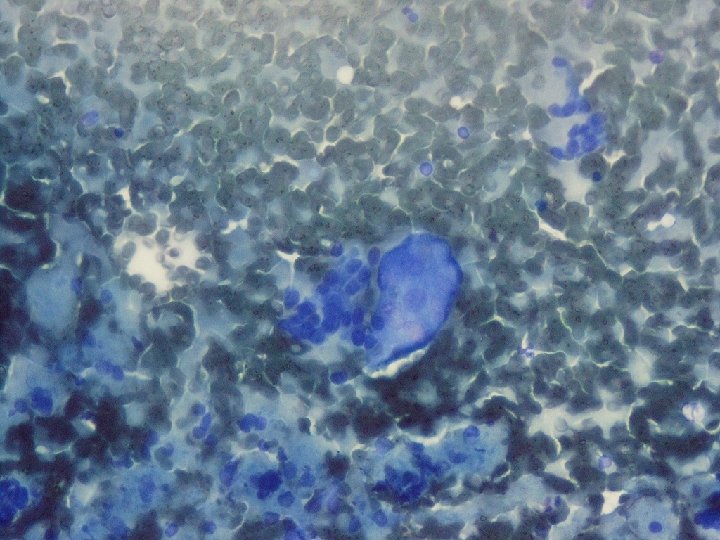
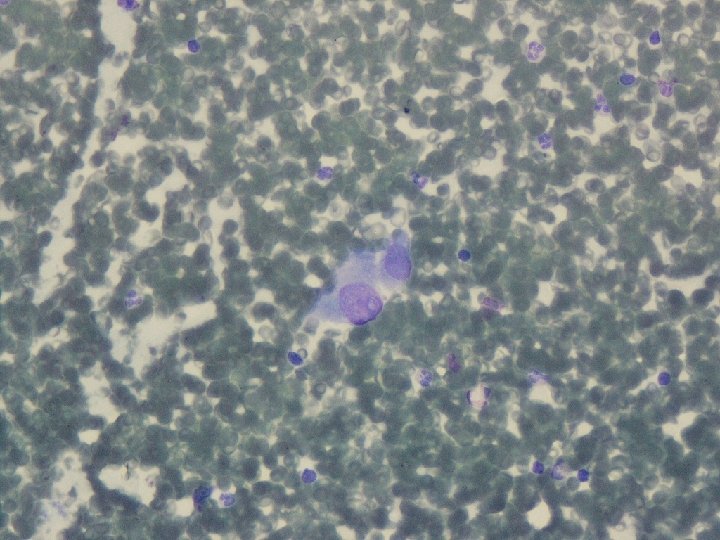
Atypia, not otherwise specified (NOS) § Population of follicular cells with nuclear enlargement and prominent nucleoli when there is uncertainty regarding the clinical history § Psammomatous calcifications in the absence of nuclear features of papillary carcinoma
Atypical cells post radioiodine therapy
Atypia, not otherwise specified (NOS)
Psammoma bodies
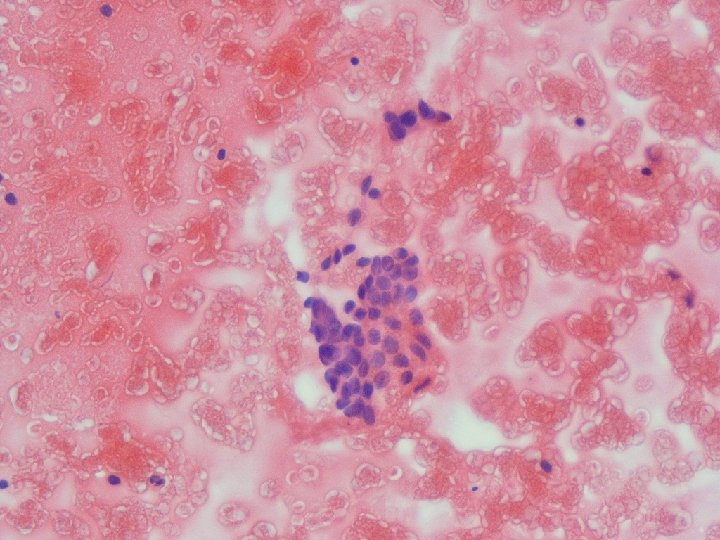
Atypical lymphoid cells, rule out lymphoma Atypical or monomorphous lymphoid infiltrate Note: Recommendation for flowcytometry
Atypia of undetermined significance with atypical lymphoid cells
Risk of malignancy (ROM) In the first edition 5– 15% In the second edition 10– 30% After introduction of NIFTP 6– 18% Cytologic (nuclear) atypia> Architectural atypia> Hürthle cell-type
How to Report • Subclassification of FLUS with descriptive language (Such as Focal cytologic atypia) • Recommendation
Management § Repeat FNA § Molecular testing § Lobectomy When the FNA is repeated 10– 30% of FLUS nodules are reported again as FLUS.
Decision for surgery or observation is based on: • • • Cytology Molecular findings Clinical findings Radiologic findings Clinical risk factors Patient preference
THANK YOU