Thyroid Antithyroid drugs Contents v Physiology of thyroid




 contains four iodine atoms. Deiodination leads to")
 and retinoid X")







 Symptoms Signa Tiredness, weakness Dry")



 Symptoms Signa Hyperactivity, irritability, dysphoria")




")
 1. inhibit the function of TPO, reducing oxidation and organification")
 Treatment")
 Antithyroid drugs")

- Slides: 33
Thyroid & Anti-thyroid drugs
Contents v Physiology of thyroid hormone Abnormal TFT - Hypothyroidism - Thyrotoxicosis v Thyroid hormone & Anti-thyroid drugs - Drug action - Side effects v
Physiology of thyroid hormone
Regulation of thyroid hormone synthesis Left. Thyroid hormones T 4 and T 3 feed back to inhibit hypothalamic production of thyrotropin-releasing hormone (TRH) and pituitary production of thyroidstimulating hormone (TSH). TSH stimulates thyroid gland production of T 4 and T 3. Right. Thyroid follicles are formed by thyroid epithelial cells surrounding proteinaceous colloid, which contains thyroglobulin. Follicular cells, which are polarized, synthesize thyroglobulin and carry out thyroid hormone biosynthesis. TSH-R, thyroid-stimulating hormone receptor; Tg, thyroglobulin; NIS, sodium iodide symporter; TPO, thyroid peroxidase; DIT, diiodotyrosine; MIT, monoiodotyrosine.
Structures of thyroid hormones Thyroxine (T 4) contains four iodine atoms. Deiodination leads to production of the potent hormone triiodothyronine (T 3), or the inactive hormone reverse T 3.
Mechanism of thyroid hormone receptor action The thyroid hormone receptor (TR) and retinoid X receptor (RXR) form heterodimers that bind specifically to thyroid hormone response elements (TRE) in the promoter regions of target genes. In the absence of hormone, TR binds corepressor (Co. R) proteins that silence gene expression. The numbers refer to a series of ordered reactions that occur in response to thyroid hormone: (1) T 4 or T 3 enters the nucleus; (2) T 3 binding dissociates Co. R from TR; (3) Coactivators (Co. A) are recruited to the T 3 -bound receptor; (4) gene expression is altered.
Characteristics of Circulating T 4 and T 3 T 4 T 3 Total hormone 8 g/d. L 0. 14 g/d. L Fraction of total hormone in the free form 0. 02% 0. 3% 21 × 10– 12 M 6 × 10– 12 M 7 d 0. 75 d Fraction directly from the thyroid 100% 20% Production rate, including peripheral conversion 90 g/d 32 g/d 20% 70% 0. 3 1 10– 10 M 10– 11 M Hormone Property Serum concentrations Free (unbound) hormone Serum half-life Intracellular hormone fraction Relative metabolic potency Receptor binding
Thyroid function test : normal & abnormal
Screening for thyroid function
Interpretation of TFT TSH ↓ ↑ FT 4 NL ↓ Hyperthyroidism NL ↑ Thyroid Hr. resistance, TSH-producing pituitary adenoma Subclinical hyperthyroidism euthyroidism Subclinical hypothyroidism Non-thyroidal illness, 2’ or 3’ hypothyroidism Primary hypothyroidism
갑상선기능검사를 해야 하는 경우 • • Congenital hypothyroidism Goiter or thyroid nodules Type 1 diabetes Atrial fibrillation Hyperlipidemia Osteoporosis Subfertility • Beginning at age 35 years and every 5 years thereafter (ATA). • • History of PP thyroiditis Down/Turner syndrome Amiodarone, lithium Post-neck irradiation Post-destructive therapy Vitiligo, leukotrichia Adrenal insufficiency Pernicious anemia
갑상선기능이상을 시사하는 검사소견들 Hypothyroidism • Hypercholesterolemia • Hyponatremia • Anemia • Creatine phosphokinase/lactate dehydrogenase elevation • Hyperprolactinemia Hyperthyroidism • Hypercalcemia • Alkaline phosphatase elevation • AST/ALT elevation
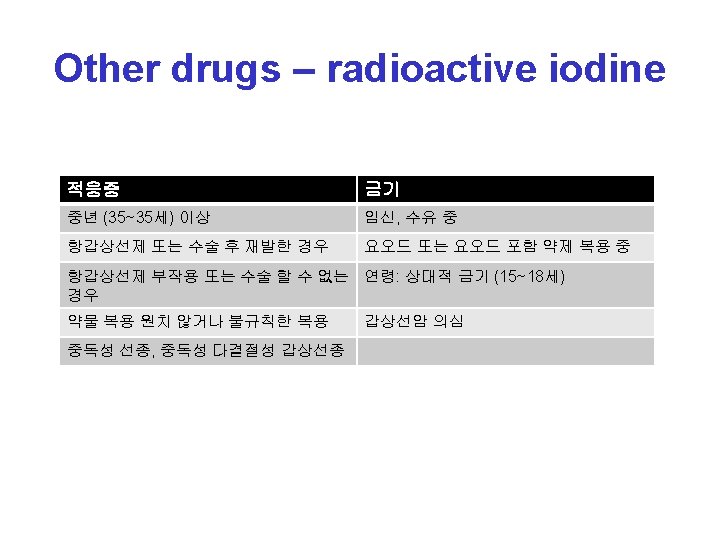
Causes of Hypothyroidism Primary Autoimmune hypothyroidism: Hashimoto's thyroiditis, atrophic thyroiditis Iatrogenic: 131 I treatment, subtotal or total thyroidectomy, external irradiation of neck for lymphoma or cancer Drugs: iodine excess (including iodine-containing contrast media and amiodarone), lithium, antithyroid drugs, p-aminosalicylic acid, interferon- and other cytokines, aminoglutethimide, sunitinib Congenital hypothyroidism: absent or ectopic thyroid gland, dyshormonogenesis, TSH-R mutation Iodine deficiency Infiltrative disorders: amyloidosis, sarcoidosis, hemochromatosis, scleroderma, cystinosis, Riedel's thyroiditis Overexpression of type 3 deoiodinase in infantile hemangioma Transient Silent thyroiditis, including postpartum thyroiditis Subacute thyroiditis Withdrawal of thyroxine treatment in individuals with an intact thyroid After 131 I treatment or subtotal thyroidectomy for Graves' disease Secondary Hypopituitarism: tumors, pituitary surgery or irradiation, infiltrative disorders, Sheehan's syndrome, trauma, genetic forms of combined pituitary hormone deficiencies Isolated TSH deficiency or inactivity Bexarotene treatment Hypothalamic disease: tumors, trauma, infiltrative disorders, idiopathic
Signs and Symptoms of Hypothyroidism (Descending Order of Frequency) Symptoms Signa Tiredness, weakness Dry coarse skin; cool peripheral extremities Dry skin Puffy face, hands, and feet (myxedema) Feeling cold Diffuse alopecia Hair loss Bradycardia Difficulty concentrating and poor memory Peripheral edema Constipation Delayed tendon reflex relaxation Weight gain with poor appetite Carpal tunnel syndrome Dyspnea Serous cavity effusions Hoarse voice Menorrhagia (later oligomenorrhea or amenorrhea) Paresthesia Impaired hearing
Facial appearance in hypothyroidism Puffy eyes and thickened, pale skin
Evaluation of hypothyroidism TPOAb+, thyroid peroxidase antibodies present; TPOAb –, thyroid peroxidase antibodies not present; TSH, thyroid-stimulating hormone.
Causes of Thyrotoxicosis Primary hyperthyroidism Graves' disease Toxic multinodular goiter Toxic adenoma Functioning thyroid carcinoma metastases Activating mutation of the TSH receptor Activating mutation of Gs (Mc. Cune-Albright syndrome) Struma ovarii Drugs: iodine excess (Jod-Basedow phenomenon) Thyrotoxicosis without hyperthyroidism Subacute thyroiditis Silent thyroiditis Other causes of thyroid destruction: amiodarone, radiation, infarction of adenoma Ingestion of excess thyroid hormone (thyrotoxicosis factitia) or thyroid tissue Secondary hyperthyroidism TSH-secreting pituitary adenoma Thyroid hormone resistance syndrome: occasional patients may have features of thyrotoxicosis Chorionic gonadotropin-secreting tumorsa Gestational thyrotoxicosisa
Signs and Symptoms of Thyrotoxicosis (Descending Order of Frequency) Symptoms Signa Hyperactivity, irritability, dysphoria Tachycardia; atrial fibrillation in the elderly Heat intolerance and sweating Tremor Palpitations Goiter Fatigue and weakness Warm, moist skin Weight loss with increased appetite Muscle weakness, proximal myopathy Diarrhea Lid retraction or lag Polyuria Gynecomastia Oligomenorrhea, loss of libido
Features of Graves' disease A. Ophthalmopathy in Graves' disease; lid retraction, periorbital edema, conjunctival injection, and proptosis are marked. B. Thyroid dermopathy over the lateral aspects of the shins. C. Thyroid acropachy.
Evaluation of thyrotoxicosis a. Diffuse goiter, positive TPO antibodies, ophthalmopathy, dermopathy; bcan be confirmed by radionuclide scan. TSH, thyroid-stimulating hormone.
Causes of Thyroiditis Acute Bacterial infection: especially Staphylococcus, Streptococcus, and Enterobacter Fungal infection: Aspergillus, Candida, Coccidioides, Histoplasma, and Pneumocystis Radiation thyroiditis after 131 I treatment Amiodarone (may also be subacute or chronic) Subacute Viral (or granulomatous) thyroiditis Silent thyroiditis (including postpartum thyroiditis) Mycobacterial infection Chronic Autoimmunity: focal thyroiditis, Hashimoto's thyroiditis, atrophic thyroiditis Riedel's thyroiditis Parasitic thyroiditis: echinococcosis, strongyloidiasis, cysticercosis Traumatic: after palpation
Clinical course of subacute thyroiditis The release of thyroid hormones is initially associated with a thyrotoxic phase and suppressed thyroid-stimulating hormone (TSH). A hypothyroid phase then ensues, with low T 4 and TSH levels that are initially low but gradually increase. During the recovery phase, increased TSH levels combined with resolution of thyroid follicular injury leads to normalization of thyroid function, often several months after the beginning of the illness. ESR, erythrocyte sedimentation rate; FT 4, free or unbound T 4.
Anti-thyroid drug (thionamides)
MOA (mode of action) 1. inhibit the function of TPO, reducing oxidation and organification of iodide 2. reduce thyroid antibody levels 3. inhibits deiodination of T 4 T 3 (PTU)
Common side effects v Rash, urticaria, fever, and arthralgia (1– 5% of patients) Treatment - may resolve spontaneously or after substituting an alternative antithyroid drug - antihistamine v Transient leukopenia (m/c) : 12% of adults - not progress to agranulocytosis v
Rare but major side effects v v Hepatitis, SLE-like syndrome, agranulocytosis (<1%) Antithyroid drugs must be stopped and not restarted Agraulocytosis - written instructions should be provided regarding the symptoms of possible agranulocytosis (e. g. , sore throat, fever, mouth ulcers) - CBC - onset is idiosyncratic and abrupt : not predictable v
Drug & Thyroid function test TSH 증가시키는 약제 TSH 감소시키는 약제 요오드를 포함하고 있는 약제: lugol’s sol. Amiodarone, contrast agent 도파민 작용 물질: 도파민, L-dopa, 2 bromocryptine, lisuride, pyridoxine, apomorphine, perbidil lithium α-noradrenergic 차단제: phentolamine, thioridazine 도파민 수용체 차단제: domperidone, metoclopramide 세로토닌 억제제: cyproheptadine, methylseride 도파민 차단제: sulpride 당류코르티코이드 Decarboxylate inhibitor: benserazide 아스피린 L-도파 억제제: chloropromazine, biperidine, 성장호르몬 haloperidol cimetidine 소마토스타틴 항에스트로겐제: clomifene Opiates amphetamine spironolactone