Thrombotic microangiopathy Dr RAWAL MAHENDRA WHAT IS IT

Thrombotic microangiopathy Dr. RAWAL MAHENDRA

WHAT IS IT?
 �calcineurin inhibitor")
Causes Thrombotic microangiopathy �Autoimmune hemolytic anemia/evans syndrome �DIC �Pregnancy associated(HELLP, eclampsia, ) �calcineurin inhibitor �Malignant HTN �infection typical virus(cytomegalovirus, adenovirus, herpes simplex virus, hiv), severe bacterial(meningococcus, pneumococcus) �Malignancy �TTP/HUS

Classification of thrombotic microangiopathy �Idiopathic TTP: autoimmune ADAMTS 13 DEFICIENCY in majority of patient �Secondary TTP: mechanism mostly unknown associated with cancer, infection, hematopoetic stem cell transplantation , solid organ transplantation, drugs, chemotherapy.
, S. DYSENTERIAE.")
HUS � 1. SHIGA TOXIN INDUCED HUS: E. COLI(O 157: H 7), S. DYSENTERIAE. PATHOGENESISTOXIN MEDIATED ENDOTHELIAL DAMAGE � 2. NEURAMINIDASE HUS: pneumococcal neuraminidase exposes thomsen cryptantigen. � 3. ATYPICAL HUS: defciency of complement regulatory protein

ROLE OF v. WF �Vessel injuries and under high shear stress vwf is synthesized in vascular endothelial cell and megakaryocyte. �Vwf bind to factor viii and paltlet surface glycoproteins �Facilitate platlets aggregation and adhesions

Role of ADAMTS



Schistocytes Increased LDH Coomb’s negative Increased Retic count Low heptoglobin, Increased indirect bilirubin, Hemoglobinuria

Diagnostic approach to TTP-HUS and TMA � ANEMIA , THROMBOCYTOPENIA , INCREASE LDH , INCREASE BILIRUBIN. �STEP 1. EXCLUDE DRUGS. : QUININE , INTERFERON, SIMVASTATIN, CALCINEURIN INHIBITORS(cyclosporin, tacrolimus). �MEDICATION ASSOCIATED WITH PRECIPITATION OF TTP INCLUDE QUININE AND ESTROGEN CONTAINING MEDICATIONS WHICH SHOULD BE AVOIDED TO PREVENT RERLAPSE IN PT WITH PREVIOUS EPISODE OF TTP. �WOMEN WITH PREVIOUS TTP SHOULD BE OFFERED NON OESTROGEN CONTAINING CONTRACEPTION.

�STEP 2: �ANEMIA , THROMBOCYTOPENIA, INCREASE LDH , INCREASE BILIRUBIN. �COOMBS TEST +VE : AUTOIMMUNE HEMOLYSIS/EVANS SYNDROME. �COOMBS TEST -VE/SCHISTOCYTES +nt: other causes of TMA

STEP 3 1. PT , APTT, INR 2. PT , APTT, INR NORMAL TTP/HUS OR OTHER. ABNORMAL FDP HIGH IN DIC, NORMAL IN HELLP

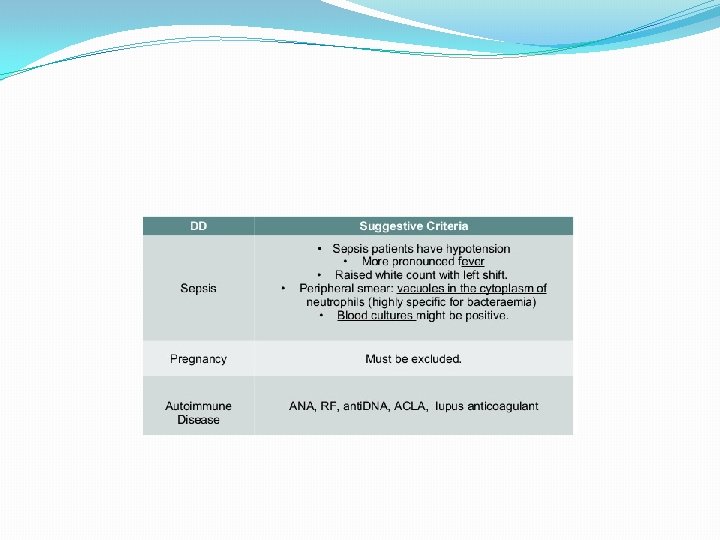
STEP 4 : EXCLUDE OTHER CAUSES

�TTP HAS BEEN REPORTED IN ASSOCIATION WITH PANCREATITIS �SOMETIMES A NUMBER OF DAYS AFTER RESOLUTION OF PANCREATITIS �ALL PT WERE SUCCESSFULLY TREATED WITH PEX AND CORTICOSTEROID(MCDONALD ET AL, 2009)

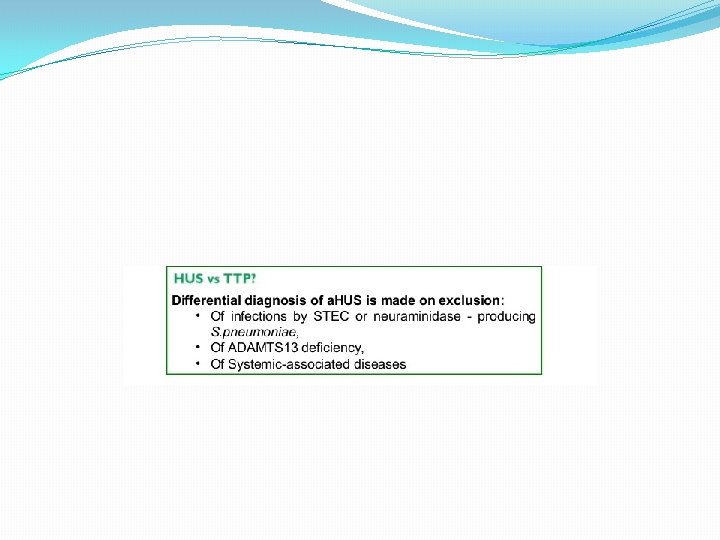
STEP 5 �TTP VS HUS �SHIGA TOXIN HUS OCCURS PRIMARILY IN CHILDREN �WATERY OF BLOODY DIARRHEA �STOOL CULTURE: DETECTION OF E. COLI 0157: H 7 AND OTHER STEC AND THEIR PRODUCT IN STOOL CULTURE

�NEURAMINIDASE HUS: LESS THAN 2 YEAR OLD RESPIRATORY DISTRESS, NEUROLOGIC INVOLVEMENT AND COMA. �ATYPICAL HUS AND TTP: DIFFICULT TO DISTINGUISH ON CLINICAL BACKGROUND ONLY
 exchanges,")
treatment �Plasma Therapy �PEX should be started with 1. 5 plasma volume (PV) exchanges, using solvent/detergent-treated (S/D) plasma in all age groups and reassessed daily (1 B). �The volume of exchange can be reduced to 1. 0 PV when the clinical condition and laboratory test results are stabilizing (2 C). �Intensification in frequency and or volume of PEX procedures should be considered in life-threatening cases (2 B). �Daily PEX should continue for a minimum of 2 d after platelet count has been >150 X 109/l and then stopped (2 B).

�Congenital TTP: �Recommendation 1 S/D plasma infusion or intermediate purity Factor VIII (eg BPL 8 Y) should be used to treat congenital TTP (1 C). � Treatment regimens for congenital TTP should be individualized according to the patient’s phenotype (1 A).
 cannot be")
� Treatment of TTP in Pregnancy � If a thrombotic microangiopathy (TMA) cannot be fully explained by a non-TTP pregnancy-related TMA, then the diagnosis of TTP must be considered and PEX should be started (2 B). � Mothers with congenital TTP should attend a specialist centre and receive ADAMTS 13 supplementation regularly throughout pregnancy and the post-partum period (1 A). � Close liaison with an obstetrician with a special interest in fetomaternal medicine is required in mothers with TTP (1 A). � In mothers with acquired TTP, ADAMTS 13 activity should be monitored throughout pregnancy to help predict the need for adjuvant therapy and outcome (1 B). � Pre-conceptual counselling is advised for subsequent pregnancies and women of child bearing age should be counselled about potential risks of pregnancy and combined oral contraceptive pill (COCP) (2 B).

� HIV-related TTP � If a patient with TTP is found to have HIV infection then viral load should be measured an HIV physician should be closely involved in management (1 A). � TTP should be considered in an HIV-positive individual with a MAHA and thrombocytopenia (1 A). � PEX in conjunction with highly active antiretroviral therapy (HAART) (triple or quadruple therapy) should be started as soon as the diagnosis of HIV-associated TTP is made (1 B). � HAART should be given immediately after PEX therapy to maximize time for absorption (1 A). � HAART should be continued after remission to prevent further relapse (1 B). � In resistant HIV-related TTP, rituximab could be considered (2 B).

�Malignancy-Associated Thrombotic Microangiopathy �PEX is not indicated in the management of malignancy and bone marrow transplant-associated TMA (1 A). �In cancer associated TMA, further treatment for the underlying cancer should be considered (1 A).

Further Treatments in Acquired TTP � Corticosteroids � Intravenous daily methylprednisolone (e. g. , 1 g/d for three consecutive days – adult dose) or high dose oral prednisolone (e. g. , 1 mg/kg/d) should be considered (1 B). � Rituximab � In acute idiopathic TTP with neurological/cardiac pathology, which are associated with a high mortality, rituximab should be considered on admission, in conjunction with PEX and steroids (1 B). � Patients with refractory or relapsing immune-mediated TTP should be offered rituximab (1 B). � Ciclosporin A (CSA) and Tacrolimus � CSA may be considered as second line therapy in patients with acute or chronic relapsing acquired TTP (1 C). � Splenectomy may rarely be considered in the non-acute period of immunemediated TTP but has limited proven benefit (2 C).

� Antiplatelet Agents � The clinical efficacy of antiplatelet agents in TTP is unproven but they are relatively safe (1 B). � Low dose aspirin (75 mg once per day [OD]) may be given during platelet recovery (platelet count >50 X 109/l) (2 B). � Supportive Therapy � Red cell transfusion should be administered according to clinical need especially if there is cardiac involvement (1 A). � Folate supplementation is required during active haemolysis (1 A). � Platelet transfusions are contraindicated in TTP unless there is lifethreatening haemorrhage (1 A). � Thromboprophylaxis with low molecular weight heparin (LMWH) is recommended once platelet count has reached >50 X 109/l (1 B).
")
�Refractory TTP(progression of clinical symptoms or persistent thrombocytopenia despite 7 daily PEX procedure. ) �Increased frequency of PEX and addition of rituximab can be considered in refractory TTP (1 B). �Relapse ( episode of acute TTP more than 30 day after remission and occurs in 20 -50% of cases) �Increased PEX and/or rituximab therapy are the agents of choice in relapsing disease (1 B). �Patients should be counselled about symptoms, signs and risk of relapse before discharge with verbal and written information (1 A). �In patients with a documented reduction of ADAMTS 13 activity to <5%, elective therapy with rituximab can be considered (1 B).
 �No role of antibiotics")
Shiga toxin associated HUS treatment �Generally supportive(including RRT if required) �No role of antibiotics except �Patient presenting with bacteremia �Shigella dysentery type 1 �Azithromycin has some benefit on duration of bacterial shedding in adult patient from german O 104: H 4 epidemic
 COMBINED WITH PLASMA")
Atypical HUS �PLASMA EXCHANGE �PLUS IMMUNOSUPPRESSANTS(CORTICOSTEROID AND AZATHIOPRINE OR MYCOPHENOLATE MOFETIL) COMBINED WITH PLASMA EXCHANGE ALLOWED LONG TERM DIALYSIS FREE SURVIVAL IN 60 TO 70 % OF PATIENT.

THANK YOU
- Slides: 34