Thrombosis There are three primary influences on thrombus
:")
Thrombosis ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ There are three primary influences on thrombus formation (called Virchow's triad): (1) Endothelial injury. (2) Stasis or turbulence of blood flow. (3) Blood hypercoagulability

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 1. Endothelial injury : Loss of endothelium leads to exposure of subendothelial ECM, adhesion of platelets, release of tissue factor, and local depletion of PGI 2 and plasminogen activators

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 2. Alterations in Normal Blood Flow Normal blood flow is laminar, such that platelets flow centrally in the vessel lumen, separated from the endothelium by clear zone of plasma. Stasis and turbulence disrupt laminar flow and bring platelets into contact with the endothelium promote endothelial cell injury, resulting in local thrombosis, leukocyte adhesion, etc.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 3. Hypercoagulability : Defined as any alteration of the coagulation pathways that predisposes to thrombosis, and it can be divided into primary (genetic) and secondary (acquired) disorders.
 Mutation in factor V gene (factor V")
Examples Hypercoagulability states: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Primary (Genetic) Mutation in factor V gene (factor V Leiden). Mutation in prothrombin gene. Antithrombin III deficiency. Protein C deficiency. Protein S deficiency. Secondary (Acquired) High risk for thrombosis Prolonged bed rest or immobilization Myocardial infarction. Tissue damage (surgery, fracture, burns). Cancer.

Examples of thrombosis: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Arterial thrombi Produced by platelet and coagulation activation; they are typically a friable meshwork of platelets, fibrin, erythrocytes, and degenerating leukocytes. Usually superimposed on an atherosclerotic plaque, other vascular injury (vasculitis, trauma).

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Venous thrombosis Result of activation of the coagulation cascade, and platelets play a secondary role. Because these thrombi form in venous circulation, they contain more erythrocytes and are therefore called red, or stasis, thrombi. The veins of the lower extremities are most commonly affected (90% of venous thromboses). -Phlebothrombosis(e. g in varicose veins) -Deep venous thrombosis

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Mural thrombi: Thrombi occurring in heart chambers or in the aortic lumen. caused by: Abnormal myocardial contraction. Endomyocardial injury. Ulcerated atherosclerotic plaques. Aneurysmal dilation of the aorta.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Vegetations : Thrombi on heart valves. Bacterial or fungal blood-borne infections can cause valve damage, subsequently leading to large thrombotic masses (infective endocarditis). Sterile vegetations can also develop on noninfected valves in hypercoagulable states, so-called nonbacterial thrombotic endocarditis

Fate of the Thrombus : ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 1. Propagation: Thrombi accumulate additional platelets and fibrin, eventually causing vessel obstruction 2. Embolization: Thrombi dislodge or fragment and are transported elsewhere in the vasculature 3. Dissolution: Thrombi are removed by fibrinolytic activity. 4. Organization and recanalization: Thrombi induce inflammation and fibrosis (organization). These can eventually recanalize (re-establishing some degree of flow)

EMBOLISM ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ An embolus is a detached intravascular solid, liquid, or gaseous mass that is carried by the blood to a site distant from its point of origin. Emboli lodge in vessels resulting in partial or complete vascular occlusion
 of downstream tissue.")
ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ The consequences of embolism include ischemic necrosis (infarction) of downstream tissue. Clinical outcomes of emboli depending on the site of origin, and lodge of in the vascular tree.

Examples of embolism : ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 1. Pulmonary embolism Emboli originate from deep leg vein thrombi above the level of the knee. They are carried through progressively larger channels and pass through the right side of the heart before entering the pulmonary vasculature. Depending on the size of the embolus, it may occlude the main pulmonary artery, impact across the bifurcation or pass out into the smaller, branching arterioles.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 2. Systemic Thromboembolism Is emboli in the arterial circulation. Arise from intracardiac mural thrombi, aortic aneurysms, thrombi on ulcerated atherosclerotic plaques, or fragmentation of valvular vegetations.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • The major sites for arteriolar embolization are the lower extremities (75%) and the brain (10%), with the intestines, kidneys, and spleen affected to a lesser extent.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 3. Fat Embolism Microscopic fat globules can be found in the circulation after fractures of long bones or after soft-tissue trauma. Fat embolism syndrome is characterized by pulmonary insufficiency, neurologic symptoms, anemia, and thrombocytopenia. Typically, the symptoms appear 1 to 3 days after injury.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 4. Air Embolism Gas bubbles within the circulation can obstruct vascular flow. Air may enter the circulation during obstetric procedures or as a consequence of chest wall injury. Generally, more than 100 m. L of air are required to produce a clinical effect.

INFARCTION ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Is an area of ischemic necrosis caused by occlusion of either the arterial supply or the venous drainage in a particular tissue. Tissue infarction is a common and extremely important cause of clinical illness.
Red infarcts (1) with venous occlusions (such as in ovarian torsion).")
Types: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ (i)Red infarcts (1) with venous occlusions (such as in ovarian torsion). (2) in loose tissues (such as lung). (3) in tissues with dual circulations such as lung and small intestine.
White infarcts Occur with arterial occlusions or in solid organs (such")
ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ (ii)White infarcts Occur with arterial occlusions or in solid organs (such as heart, spleen, and kidney), where the solidity of the tissue limits the amount of hemorrhage.
Septic infarctions Occur when microbes seed an area of necrotic tissue.")
ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ (iii)Septic infarctions Occur when microbes seed an area of necrotic tissue. In these cases the infarct is converted into an abscess, with greater inflammatory response.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Red and white infarcts. A, Hemorrhagic, roughly wedge-shaped pulmonary infarct (red infarct). B, Sharply demarcated pale infarct in the spleen (white infarct).

Examples of infarctions: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 1. Myocardial infarction caused by occlusion of coronary arteries. 2. Pulmonary infarction is a common complication in several clinical settings. 3. bowel infarction. 4. Ischemic necrosis of the extremities (gangrene) is a serious problem in diabetics.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Gangrenous necrosis

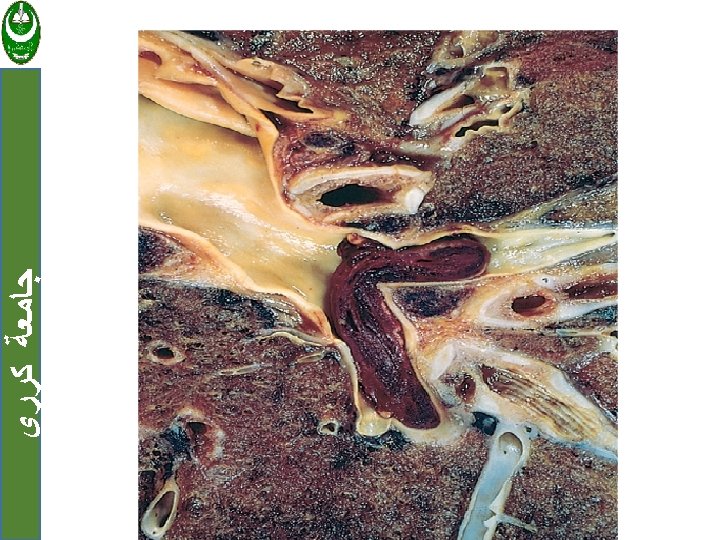
SHOCK ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • Shock is the final common pathway for a number of potentially lethal clinical events. Regardless of the underlying pathology, shock gives rise to systemic hypotension, impaired tissue perfusion, and cellular hypoxia.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ It can be caused either by reduced cardiac output or by reduced effective circulating blood volume and microbial sepsis. It has tree types cardiogenic, hypovolemic and septic shock.

Type of Shock Cardiogenic ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Hypovolemic Septic Causes: Myocardial infarction Ventricular rupture Arrhythmia Cardiac tamponade Pulmonary embolism Principal Mechanisms Failure of myocardial pump resulting from intrinsic myocardial damage, extrinsic pressure, or obstruction to outflow Hemorrhage Inadequate blood or Fluid loss (e. g. , vomiting, plasma volume diarrhea, burns, or trauma) Overwhelming microbial infections Endotoxic shock Gram-positive septicemia Fungal sepsis Superantigens (e. g. toxic shock syndrome) Peripheral vasodilation and pooling of blood; endothelial activation/injury; leukocyte -induced damage; disseminated intravascular coagulation; activation of cytokine cascades.

Stage of shock: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ 1. An initial non progressive stage during which reflex compensatory mechanisms are activated and perfusion of vital organs is maintained. 2. A progressive stage characterized by tissue hypoperfusion and onset of worsening circulatory and metabolic imbalances.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • 3. An irreversible stage that the body has incurred cellular and tissue injury and even if the hemodynamic defects are corrected, survival is not possible

Effects of shock : ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • The cellular and tissue changes induced by shock are essentially those of hypoxic injury , due to combination of hypoperfusion and microvascular thrombosis. • Shock is characterized by failure of many organ systems, particularly evident in the brain, heart, kidneys, adrenal glands, and gastrointestinal tract

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • The adrenal changes in shock there is cortical cell lipid depletion. • The kidneys typically reveal acute tubular necrosis so that oliguria, and electrolyte disturbances dominate the clinical picture. • The gastrointestinal tract may mainfest focal mucosal hemorrhage and necrosis.

ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ • The lungs are seldom affected in pure hypovolemic shock, because they are somewhat resistant to hypoxic injury. However, when shock is caused by bacterial sepsis or trauma, changes of diffuse alveolar damage may develop. • Unfortunately, most patients with irreversible changes due to severe shock die before the tissues can recover.

The clinical manifestations of shock: ﺟﺎﻣﻌﺔ ﻛﺮﺭﻱ Depend on the precipitating factor. In hypovolemic and cardiogenic shock, the patient presents with: hypotension; a weak, rapid pulse; tachypnea; and cool, cyanotic skin. In septic shock, in addition the skin may be warm and flushed as a result of peripheral vasodilation.

- Slides: 38