Thrombosis and embolism Thrombosis Gangrene Infarction Embolism Thrombosis

Thrombosis and embolism

• • Thrombosis Gangrene Infarction Embolism

Thrombosis • inappropriate clot formation within the circulation

pathogenesis is given by Virchow’s triad • endothelial injury • stasis or turbulence of blood flow • blood hypercoagulability


Endothelial Injury • The dominant of the three • Dysfunctional endothelium may elaborate greater amount of pro-coagulant factors or may synthesize lesser amount of anti-coagulant effectors. • Seen commonly in HTN, trauma, radiotherapy, smoking

Hypercoagulability • any alteration of the coagulation pathways that predisposes to thrombosis •
 Mutations like – - Fctor V - Mutation in prothrombin")
Hyper-coagulable states. Primary (Genetic) Mutations like – - Fctor V - Mutation in prothrombin gene Deficiencies like – • - Antithrombin III deficiency • - Protein C deficiency • - Protein S deficiency
 • • Prolonged bed rest or immobilization Atrial fibrillation Tissue damage (surgery,")
Secondary (Acquired) • • Prolonged bed rest or immobilization Atrial fibrillation Tissue damage (surgery, fracture, burns) Cancer Cardiomyopathy Hyperestrogenic states (pregnancy) Oral contraceptive use Smoking, Obesity

Thrombi can form in • Heart • Arterial tree • Veins

• Thrombosis within arteries can lead to necrosis of tissues which it supplies Ex-thrombosis in the coronary vessels lead to myocardial infarction Thrombosis within the renal artery leads to renal infarction

• Thrombosis in the viens can cause blockage of venous drainage of tissues • clots formed within leg veins can ascend to block the pulmonary circulation Pulmonary embolism

Fate of a thrombus • • • Propagation Dissolution Embolisation Organisation Recanalisation


Infarction • Area of ischemic necrosis caused by occlusion of either arterial supply or the venous drainage in a particular tissue • 99% infarcts are from thrombotic/embolic events and almost all are from arterial occlusion. Eg • Myocardial infarction • stroke • gangrene of limbs due to peripheral vascular disease

Factors influencing infarction: • Nature of blood supply • Lungs have dual supply from pulmonary and bronchial arteries • Liver has dual supply from hepatic artery and portal vein • Kidney, spleen and brain have end arteries with no anastomosis • Rate of occlusion: if slow, can allow for collateral formation, • Tissue vulnerability to hypoxia: neural tissue is the most susceptible, dying within 3 to 4 minutes, and myocardium within 30 to 40 min • • Oxygen content in the blood: increased risk of infarction in anemic and cyanosed patient

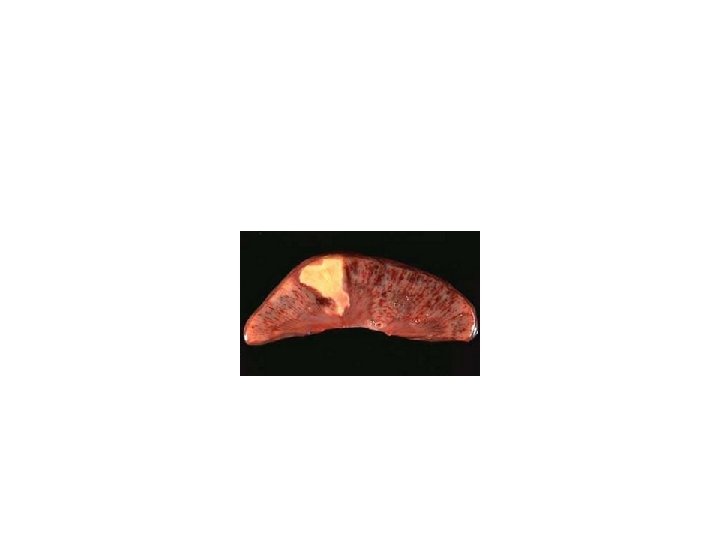
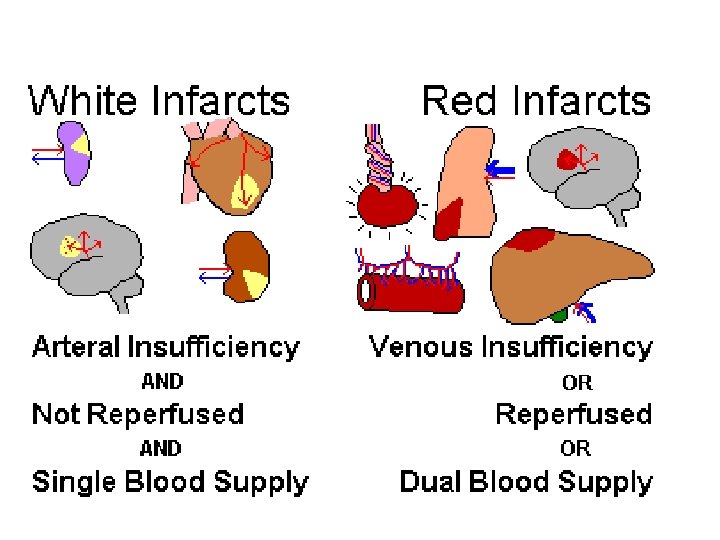
Gross Morphology • Infarction starts as a poorly defined wedge shaped area, with exudates and hemorrhagic area, which gets more defined by a rim of inflammation after some days. • 2 types according to gross appearance

Red infarct • due to venous obstruction • Due to infarction of tissues with dual blood supply like intestine • Due to reperfusion-restoring blood supply
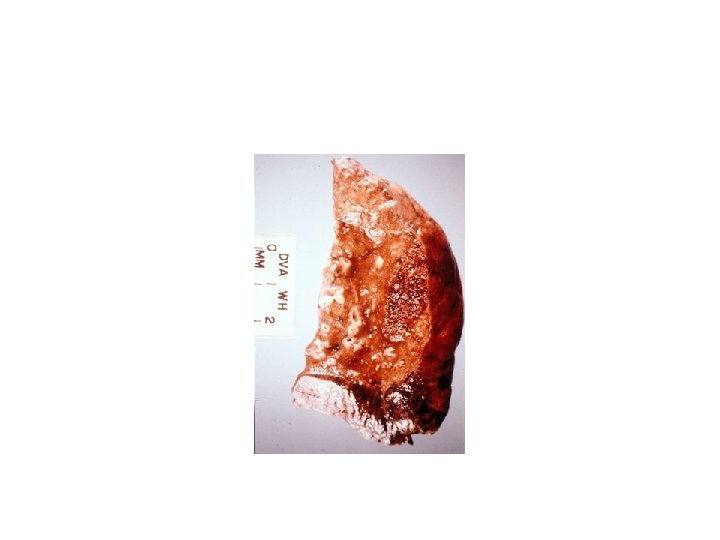

White infarct • Solid organs like kidney and liver with arterial occlusion
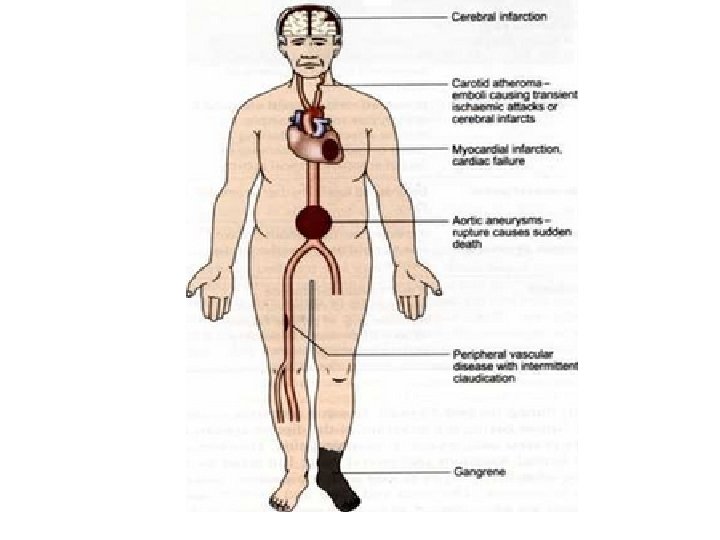

Gangrene • Gangrene refers to the death of body tissue due to a lack of blood flow complicated by bacterial infection. • Gangrene most commonly affects the extremities, including toes, fingers and limbs


Embolism • A detached intravascular solid, liquid or gaseous mass that is carried by the blood to a site distant from its point of origin • 99% of the emboli are dislodged thrombi, hence, the term THROMBOEMBOLISM • Potential consequence of embolism is INFARCTION of the tissue distal to it.

Types • Thromboembolism • Fat embolism eg after fractures • Air embolism, eg in open carotid injury, after obstetric proceedures. • Amniotic fluid embolism in pregnancy

Pulmonary thromboembolism • A common cause of death among hospitalized patients • In greater than 95% of cases, pulmonary emboli originate from deep leg vein thrombi above the level of the knee • Immobilization is a strong risk factor

What is fat embolism Describe the patho physiology of the tissue damage in fat embolism

Thank you….
- Slides: 31