THROMBOPHILIA ZAID ALGHNANEEM THROMBOPHILIA A hereditary or acquired

THROMBOPHILIA ZAID AL-GHNANEEM

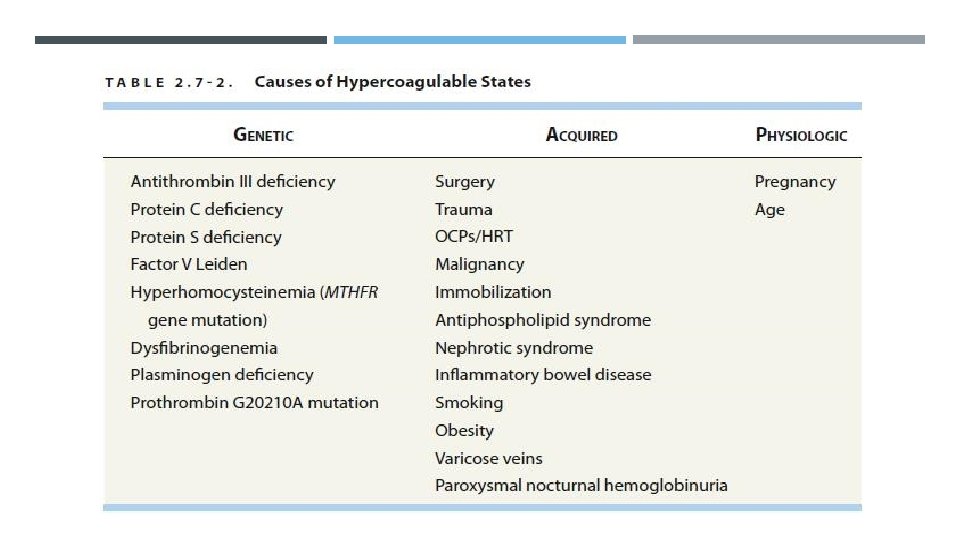
THROMBOPHILIA A hereditary or acquired disorder marked by an abnormal increase in the tendency of blood to clot and higher than normal risk of thrombosis. Causes can be genetic, acquired, or physiologic. Can present with recurrent thrombotic complications: DVT, PE, arterial thrombosis, MI, and stroke. Women may have recurrent miscarriages.
 is the most common cause of direct maternal")
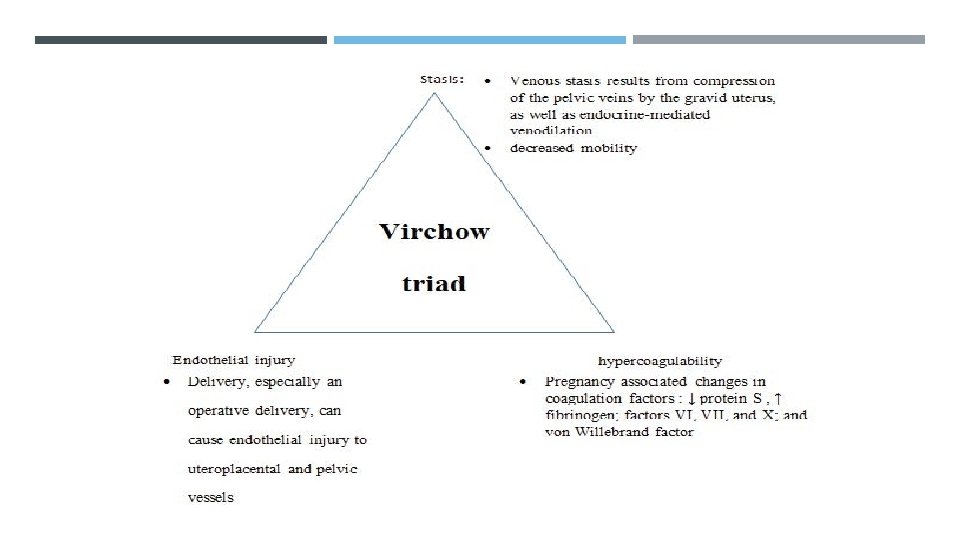
THROMBOPHILIA IN PREGNANCY Venous thromboembolism (VTE) is the most common cause of direct maternal death in the UK. Pregnancy is a hypercoagulable state because of an alteration in the thrombotic and fibrinolytic systems. There is an increase in clotting factors VIII, IX, X and fibrinogen levels, and a reduction in protein S and antithrombin (AT) III concentrations. These physiological changes predispose a woman to thromboembolism and this is further exacerbated by venous stasis in the lower limbs due to the weight of the gravid uterus placing pressure on the IVC in late pregnancy and immobility, particularly in the puerperium. The greatest risk of a venous thromboembolism (VTE) is during the first few weeks postpartum, especially following a cesarean delivery.

There is growing evidence that both heritable and acquired thrombophilias are associated with a range of adverse pregnancy outcomes, particularly recurrent fetal loss. The major hereditary forms of thrombophilia currently recognized include: deficiencies of the endogenous anticoagulants protein C, protein S and AT III; abnormalities of procoagulant factors, factor V Leiden (caused by a mutation in the factor V gene) and the prothrombin mutation G 20210 A. Acquired thrombophilia is most commonly associated with antiphospholipid syndrome (APS). APS is the combination of lupus anticoagulant with or without anticardiolipin antibodies, with a history of recurrent miscarriage and/or thrombosis. It may (or, more commonly, may not) be associated with other autoantibody disorders such as systemic lupus erythematosus (SLE).
, means that prophylaxis")
The presence of thrombophilia, with a history of thrombotic episode(s), means that prophylaxis should be considered for pregnancy.

DEEP VEIN THROMBOSIS The commonest symptoms are pain in the calf with varying degrees of redness or swelling. Women’s legs are often swollen during pregnancy, therefore unilateral symptoms should ring alarm bells. The signs are few, except that often the calf is tender to gentle touch. Compression ultrasound has a high sensitivity and specificity in diagnosing proximal thrombosis in the non-pregnant woman and should be the first investigation used in a suspected DVT. Venography is invasive, requiring the injection of contrast medium and the use of X-rays. It does, however, allow excellent visualization of veins both below and above the knee.

Clinical features: Fifty percent of cases are asymptomatic. Pain in the calf in association with dorsiflexion of the foot (positive Homans sign). Dull ache, tingling, tightness, or pain in the calf or leg, especially when walking. Acute swelling and pain in the thigh area, as well as tenderness in the femoral triangle, are suggestive of iliofemoral thrombosis. DVT in pregnancy is usually in the left leg (In a patient complaining of left lower-extremity pain and swelling, the finding of a 2 -cm difference in calf circumference is one of the more reliable clinical signs of a DVT in pregnancy).

So. . For DVT diagnosis Duplex doppler is the best initial test, whereas Venography is the gold standard.

TREATMENT OF DVT Intravenous unfractionated heparin (5 -7 days then convert to LMWH heparin throughout the pregnancy to 6 weeks postpartum) or subcutaneous low-molecular-weight heparin (enoxaparin sodium). Both forms of heparin are safe for the fetus and do not cross the placenta. Low-molecular-weight heparin should be stopped about 24 hours before delivery in the case of a planned induction or cesarean delivery. Alternatively, the patient can be switched to unfractionated heparin that can be stopped 6 hours before delivery. Warfarin is a vitamin K antagonist that crosses the placenta, carries risks of fetal hemorrhage and teratogenesis, and, with few exceptions, should be used only in the postpartum period.

PULMONARY EMBOLUS It is crucial to recognize PE, as missing the diagnosis could have fatal implications, in 70% of cases, DVT is the instigating factor. The most common presentation is of mild breathlessness or inspiratory chest pain in a woman who is not cyanosed but may be slightly tachycardic (>90 bpm) with a mild pyrexia (37. 5°C). Rarely, massive PE may present with sudden cardiorespiratory collapse. If PE is suspected, initial electrocardiogram (ECG), chest X-ray and arterial blood gases should be performed to exclude other respiratory diagnoses.

However, these investigations are insufficient on their own to exclude or diagnose PE and it may be sensible to investigate the lower limbs for evidence of DVT by ultrasound, and if positive treat with a presumptive diagnosis of PE. If all the tests are normal but a high clinical suspicion of PE remains, a ventilation perfusion (V/Q) scan or computed tomography pulmonary angiogram (CTPA) should be performed. Note that Pulmonary angiogram is the most definitive diagnostic procedure.

CLINICAL FEATURES OF PE: In most obstetric patients, the signs and symptoms of a PE are subtle. Symptoms: pleuritic chest pain - shortness of breath - air hunger – palpitations – hemoptysis - syncopal episodes. Signs: tachypnea – tachycardia - low-grade fever - pleural friction rub - pulmonary rales.

INVESTIGATIONS FOR PE ECG: sinus tachycardia with or without premature heartbeats or right ventricular axis deviation. CXR: atelectasis, pleural effusion, obliteration of arterial shadows, and elevation of the diaphragm. ABG: oxygen tension below 80 mm Hg.

PE is ultimately a radiologic diagnosis, diagnosis 3 algorithms can be used : 1 - Bilateral compression ultrasonography of the lower extremities: If positive for DVT, a PE may be assumed in a symptomatic patient. 2 - Ventilation-perfusion scan: This method poses minimal risk to the fetus, but it cannot be used in patients with an abnormal chest X-ray or in patients with asthma or chronic obstructive pulmonary disease. 3 - Computed tomographic pulmonary angiography: This technique has the advantage of noninvasive visualization of a thrombus. The radiation dose to the fetus is considered acceptably low, but there is concern about the radiation exposure to maternal breast tissue. The acute treatment of PE and follow-up during pregnancy, labor, delivery, and the postpartum period are the same as for DVT

D-dimer is now commonly used as a screening test for thromboembolic disease in non-pregnant women, in whom it has a high negative predictive value. Outwith pregnancy, a low level of D-dimer suggests the absence of a DVT or PE, and no further objective tests are necessary, while an increased level of D-dimer suggests that thrombosis may be present and an objective diagnostic test for DVT and/or PE should be performed. In pregnancy, however, D-dimer can be elevated due to the physiological changes in the coagulation system, limiting its clinical usefulness as a screening test in this situation.
 Warfarin is given orally and prolongs the prothrombin time (PT).")
TREATMENT OF THROMBOEMBOLISM (REVIEW) Warfarin is given orally and prolongs the prothrombin time (PT). Warfarin is rarely recommended for use in pregnancy (exceptions include women with mechanical heart valves) as it crosses the placenta and can cause limb and facial defects in the first trimester and fetal intracerebral haemorrhage in the second and third trimesters. Low molecular weight heparins (LMWHs) are now the treatment of choice. They do not cross the placenta and have been shown to be at least as safe and effective as unfractionated heparin (UFH) in the treatment of VTE, In addition, LMWH is safe and easy to administer. Women are taught to inject themselves and can continue on this treatment for the duration of their pregnancy.

Following delivery, women can choose to convert to warfarin (with the need for stabilization of the doses initially and frequent checks of the international normalized ratio (INR) or remain on LMWH. Both warfarin and LMWH are safe in women who are breast feeding. Newer anticoagulants such as fondaparinux (a direct factor Xa inhibitor) and lepirudin (a direct thrombin inhibitor) are not licensed for use in pregnancy and experience with them is limited. Graduated elastic stockings should be used for the initial treatment of DVT and should be worn for 2 years following a DVT to prevent post-thrombotic syndrome.

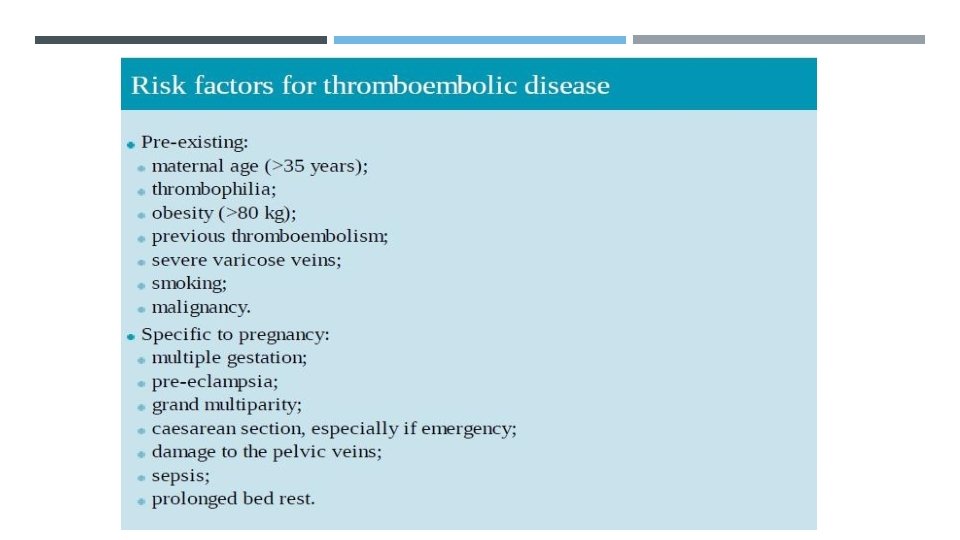
THROMBOPHILIA EVALUATION A thrombophilia workup should be considered for patients with a PE or DVT, especially those with: 1 - recurrent thromboses. 2 - a positive family history. 3 - an obstetric history suggestive of antiphospholipid syndrome. à LABS: - Acquired thrombophilia: lupus anticoagulant, anticardiolipin antibody. - Inherited thrombophilias: factor V Leiden and the prothrombin G 20210 A mutations, as well as proteins C and S and antithrombin III titers.

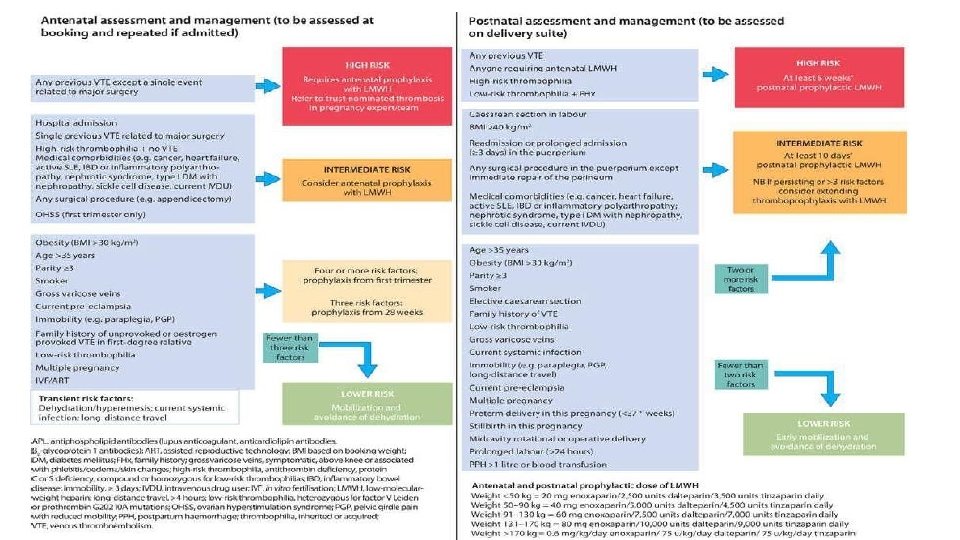
PROPHYLACTIC ANTICOAGULANT THERAPY In pregnant patients with a past history of a PE or DVT, prophylactic doses of heparin or low-molecular-weight heparin should be given during pregnancy and continued for 6 weeks postpartum. Subcutaneous injections of a prophylactic dose of heparin (5000 to 10, 000 U every 12 hours) or enoxaparin sodium (40 mg once daily) provide sufficient prophylaxis for most patients, although some pregnant women may require full anticoagulation. All pregnant women having cesarean delivery should have pneumatic compression stockings placed for thromboprophylaxis.
, sometimes known as Hughes syndrome, is a disorder of")
ANTIPHOSPHOLIPID SYNDROME Antiphospholipid syndrome (APS), sometimes known as Hughes syndrome, is a disorder of the immune system that causes an increased risk of blood clots. APS is an autoimmune condition. This means the immune system, which usually protects the body from infection and illness, attacks healthy tissue by mistake. APS can affect people of all ages, including children and babies. But most people are diagnosed with APS between 20 and 50 years of age, and it affects 3 to 5 times as many women as men. Pregnant women with APS also have an increased risk of having a miscarriage, although the exact reasons for this are uncertain.
 is used to describe the association of anticardiolipin")
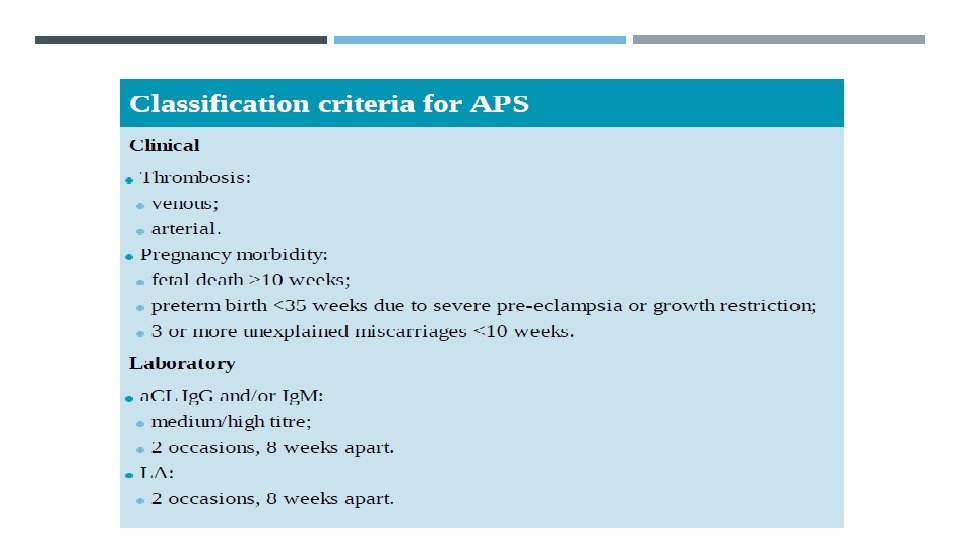
The term antiphospholipid syndrome (APS) is used to describe the association of anticardiolipin antibodies (a. CL) and/or lupus anticoagulant (LA), with the typical clinical features of arterial or venous thrombosis, fetal loss after 10 weeks’ gestation, three or more miscarriages at less than 10 weeks’ gestation or delivery before 34 weeks’ gestation due to FGR or pre-eclampsia. APS may be primary or found in association with SLE.

Due to these significant risks, pregnant women with SLE and APS require intensive monitoring for both maternal and fetal indications and should be prescribed low-dose aspirin to start by 12 weeks’ gestation. Baseline renal studies, including a 24 -hour urine collection for protein, should be performed. Blood pressure should be monitored closely because of the increased risk of preeclampsia. Serial ultrasonography is performed to assess fetal growth, umbilical artery Doppler and liquor volume. If antenatal treatment is required for SLE, steroids, azathioprine, sulfasalazine and hydroxychloroquine may be given safely. NSAIDs can be given until week 32 of pregnancy.

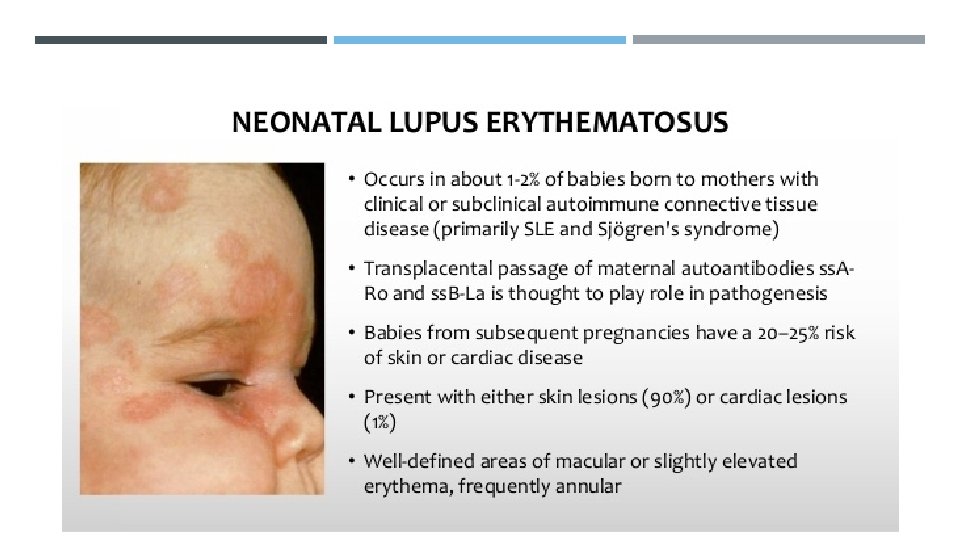
In women with APS who have suffered repeated pregnancy loss or severe obstetric complications, the combined use of low-dose aspirin and lowmolecular-weight heparin has been shown to reduce the pregnancy loss rate. Finally, 30% of mothers with SLE also have anti-Ro/La antibodies, which cross the placenta and can cause the clinical syndromes neonatal lupus and congenital heart block.

THANK YOU
- Slides: 30