Thrombolysis with Aspiration vs Mechanical Intervention Do we

"Thrombolysis with Aspiration vs Mechanical Intervention: Do we have an Answer? " L. Nelson Hopkins, M. D. Mandy J. Binning, M. D.

DISCLOSURES L. Nelson Hopkins, MD Consulting Fees – Abbott Vascular, Bard Peripheral Vascular, Boston Scientific Corporation, Micrus Endovascular Cordis, a Johnson & Johnson company Grants/Contracted Research – Cordis, a Johnson & Johnson company, Boston Scientific Corporation, Micrus Endovascular Honoraria – Access. Closure, Inc. , Bard Peripheral Vascular, Boston Scientific Corporation, Cordis, a Johnson & Johnson company, market. Rx, Inc. , Micrus Endovascular, Medsn Ownership Interest (Stocks, Stock Options or Other Ownership Interest) – APW Holding, Inc. , Boston Scientific Corporation, Magellan Spine Tech, Inc. , Med. Focus Accelerator Fund, Micrus Endovascular

"Thrombolysis with Aspiration vs Mechanical Intervention: Do we have an Answer? " E Levy MD Adnan Siddiqui, MD, Ph. D L N Hopkins, MD SUNY Buffalo Dept of Neurosurgery

Public Health Impact of Stroke § Stroke is 3 rd leading cause of death (~ 1 of every 15 deaths) § 1/3 die § 1/3 severely disabled § 1/3 recover some form of independence § Stroke is leading cause of long-term care disability. § 5 million Americans currently living with effects of stroke § $70 billion annually in the US

Ischemic Penumbra

Stroke Treatment What about IV t. PA ? ? ?
 − Marginally effective. − Large branch occlusions")
Ischemic Stroke • Intravenous thrombolysis (rt. PA) − Marginally effective. − Large branch occlusions do not respond. − May cause ICH. − Time window: “ 3 hours”. − Mild to moderate stroke. • NIHSS >10 75% decrease odds of recovery (STARS study) NIH Trial NEJM ‘ 95; 333: 1581 MAST Trial Lancet ‘ 95; 346: 1509 ECASS Trial JAMA ‘ 95; 274: 1017 ECASS II Trial Lancet ‘ 98; 352: 1245

IV Alteplase in Acute Stroke FDA Approved NINDS 3 mo death/functional dependency ECASS II Albers 57% 58% 57%

Current Strategies For the Endovascular Management of Acute Stroke • Pharmacologic − Intra-arterial t. PA • Mechanical − − Concentric - Merci Device Penumbra EKOS Foreign body retrieval devices − Alligator, Neuronet, Snares • Best data demonstrate only 5080% recanalization rate • Endovascular Bypass • Stent

Mechanical Therapy • • Why is it our first choice? Higher recanalization rates Low SICH rates 17% re-occlusion rates after IAT AJNR Am J Neuroradiol. 2004; 25: 322 -328
 Distal Device- Merci (FDA")
Mechanical Therapy Options • • • Proximal Device-Penumbra (FDA Approved) Distal Device- Merci (FDA approved) Thrombus disruption − Wire manipulation − Balloon angioplasty − Intracranial Stents
 Retriever alone − 69.")
Concentric Multi-Merci • Multi-Merci Recanalization Rates − 54. 1% (60/111) Retriever alone − 69. 4% (77/111) Post Procedure − 78 L 5 +/- X 5/X 6 − 33 X 5/X 6 − Included 27 patients who failed IV t. PA • Multi-Merci Part II includes an additional 52 patients − m. RS<2: 39% − Mortality: 30% − Symptomatic ICH: 7. 9% − Asymptomatic ICH: 28. 9%

Penumbra Thrombus Perturbation and Aspiration 041 032 026

Aspiration System Reperfusion Catheter 041 Matched 041 Separator Reperfusion Catheter 032 Matched 032 Separator Reperfusion Catheter 026 Matched 026 Separator 1274 B ™

Penumbra

Clot Retrieval Penumbra

Penumbra Data • • NIHSS>8 and less than 8 h from onset 81. 6% revascularization to TIMI 2 or 3 SAE 3. 2% 28 % ICH (11. 2 %of which were sx) NIHSS improved by >/=4 57. 8% m. RS</=2 25% Mortality at 30 d 26. 4%

The Buffalo Experience. .

Methods • Endovascular AIS interventions from 2006 to 2008 were recorded prospectively • Admission: Patient demographics; comorbid conditions; smoking status; hx CVA/TIA; AP/AC status, and/or statin therapy at presentation; time of stroke onset; presentation NIHSS; location of occlusion; degree of occlusion (TIMI).

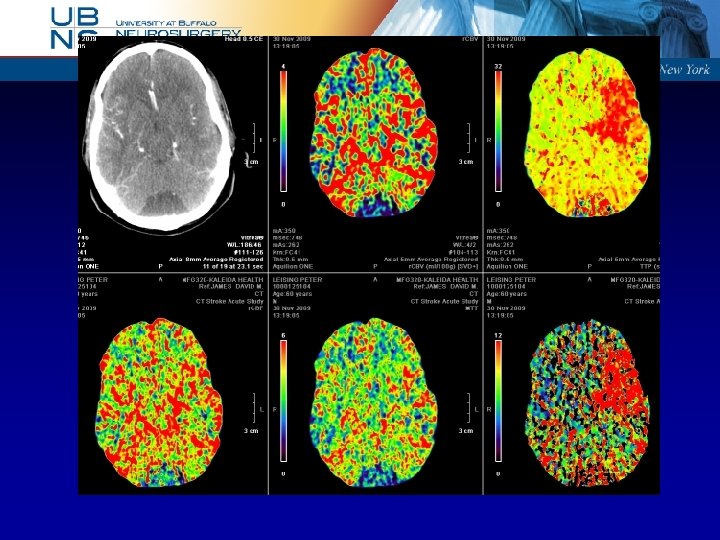
Methods • CT Perfusion Study (Aquilion One – 320 slice scanner or 64 slice scanner) • All analyzed and processed by Endovascular Fellow • Preserved Volume Map (>30%)
")
Demographics • • 193 patients Mean age 68. 4 + 17. 8 (Median 73) Male- 82, Female- 111 Mean presenting NIHSS 13. 9 + 5. 3 (Median 14)

Occlusions and Recanalization • Occlusions − TIMI 1 - 32 − TIMI 0 - 161 • Recanalization (70%) − TIMI 3 − TIMI 2 67 68
 108 67. 6 Penumbra 4 100")
Types of Therapy No. patients Recanalization rate (%) 108 67. 6 Penumbra 4 100 Intracranial stent 52 71. 2 Intracranial angioplasty 55 63. 6 Extracranial stent 36 72. 2 Extracranial angioplasty 24 75 Intravenous 38 76. 3 Intra-arterial 54 66. 7 Merci retriever GPIIb-IIIa antagonist

Summary NINDS Proact II IMS II MULTIMERCY # pts 333 180 81 164 125 193 140 NIHSS 14 17 19 19 17 14 14 66% 58% 68% 82% 70% 66% Recan Penumbra Buffalo Exp < 8 hr s. ICH 6% 10% 10% 11% 9% 6% m. RS (0 -2) 39% 40% 46% 36% 25% 39% 44% 17 25% 16% 26% 32% 28% 26% Mortality

Primary Stent for Stroke – a new paradigm

SARIS FDA approved pilot study 20 patients Multicenter Note: Due to administrative issues 1 center recruited all patients Using the Wingspan stent Evaluate safety Prospective!!

FDA approved prospective pilot study to evaluate safety 20 patients using the Wingspan stent as a bail out therapy Multi-center: Due to administrative issues 1 center recruited all patients Presentation NIHSS 14 Recanalization 100% SICH 5% m. RS < 2 at 3 months 45% Mortality at 3 months 25% Stroke. 2009 Nov; 40(11): 3552 -6 Limitation- Cherry picked few ideal patients

Retrospective Study from 4 centers 20 patients with Enterprise stent for salvage after other modalities failed for revascularization of AIS Presentation NIHSS 17 TIMI 2/3 recanalization 100% Mean NIHSS improvement at discharge 8 points J Neurosurg. 2009 Sep 18.
 < 8 hr")
SARIS outpaces the Buffalo Mechanical Revascularization Experience Buffalo Exp (2006 -2008) < 8 hr > 8 hr SARIS 0 -3 hr Endo # pts 193 140 30 20 94 NIHSS 14 14 13 14 15 Recan 70% 66% 67% 100% 70% s. ICH 9% 6% 10% 5% 5% m. RS (0 -2) 39% 44% 20% 45% 37% Mortality 28% 26% 33% 25% 26%

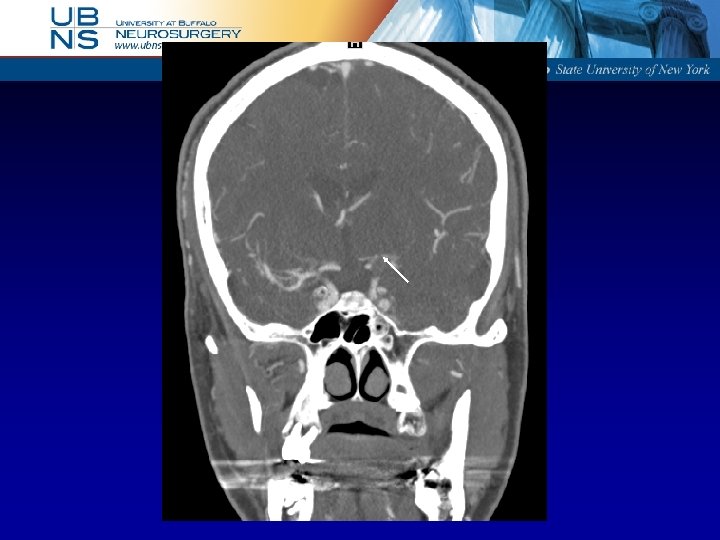
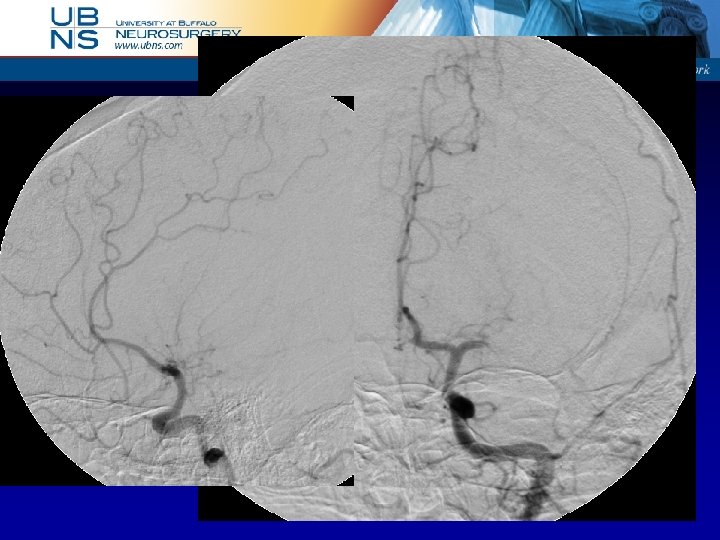
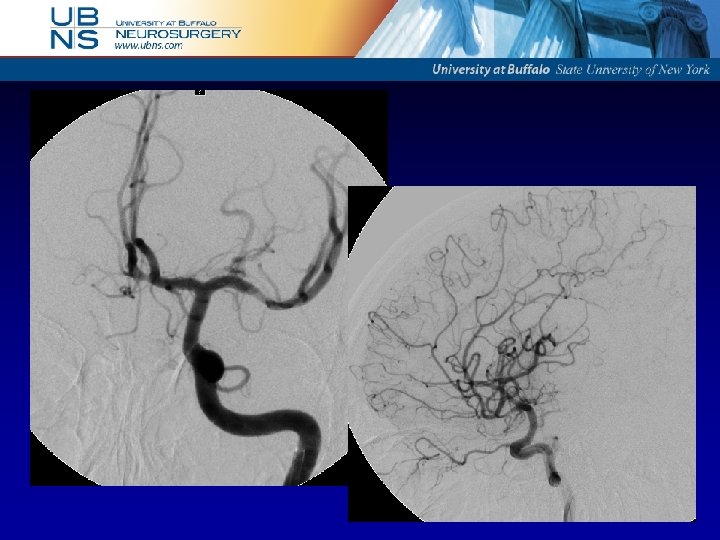
SARIS CASE • 60 yo M • Presented with R-sided weakness and dysphasia that improved to NIHSS 2 • History of afib, off coumadin due to recent fall with small SDH • CTA showed L ICA T-occlusion • Started on ASA/Plavix/Heparin gtt • 7 hours later exam declined acutely to NIHSS 10 • CT no change in SDH • Angiogram, migration of thrombus to L M 1
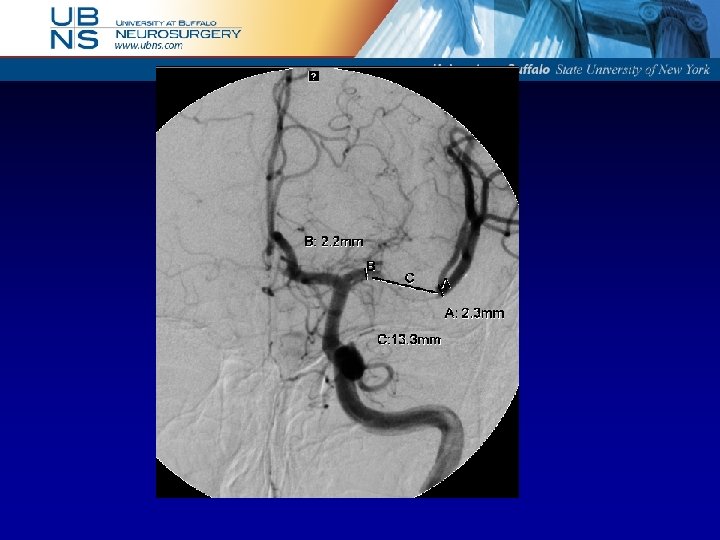

Devices used • • • 8 F sheath 6 F Envoy Nautica/Goldtip BMW Wingspan stent 2. 5 x 20 mm Heparin 5000 U

Outcome • Immediate improvement on table NIHSS 10 to 4 • POD #2 NIHSS 1 (slight dysphasia)

Post-procedure CTP

Stent patent

Post-procedure Day #2

SARIS II University of Florida Mc. Knight Brain Institute

Conclusions • Mechanical Endovascular Treatment is Preferred in Acute Stroke • Technical Nuances of Mechanical Revascularization − Penumbra, Merci − Intracranial stent (SARIS) • Buffalo Experience-Recanalization with Penumbra and Merci not as successful as stenting • The word is still out—maybe stenting will be best

Thank you!
- Slides: 44