Thromboangiitis Obliterans Buergers Disease Nonatherosclerotic segmental inflammatory disease

Thromboangiitis Obliterans Buerger’s Disease Nonatherosclerotic segmental inflammatory disease affecting small and medium-sized arteries/veins in upper/lower extremities Categorized as a vasculitis – Highly inflammatory thrombus with sparing of vessel wall Most commonly seen in young men with heavy tobacco use
: first case of 57 yo male with foot pain leading")
History 1879 (von Winiwarter): first case of 57 yo male with foot pain leading to gangrene – Pathologic specimen showed intimal proliferation, thrombosis, and fibrosis – Suggested that vessel changes distinct from atherosclerosis 1908 (Buerger): detailed description of 11 amputated limbs at Mt. Sinai with endarteritis and endophlebitis 1928 (Allen & Brown): 200 cases at Mayo Clinic – Jewish men that were heavy smokers

Epidemiology More prevalent in Middle and Far East than in N. America – Mayo Clinic showed decline from 104/100 k in ’ 47 to 12/100 k in ’ 86 – International series widely variable in terms of causes of limb ischemia Western Europe 0. 5 -5. 6% Poland 3% E. Germany 6. 7% Czech Republic 11. 5% Yugoslavia 39% India 45 -63% Women have increasing incidence – Published series prior to 1970: 1 -2% – 23% at Cleveland Clinic (1970 -1987) – 19% at OHSU (1987)

Etiology UNKNOWN! – Distinct from other vasculitis 1. thrombus is highly cellular with less intense cellular reaction in vessel wall 2. normal immunologic markers Strong association with smoking No gene association found yet Conflicting studies regarding hypercoagulable states – Increased urokinase plasminogen activator – Impaired endothelium-dependent vasorelaxation Immunologic mechanisms may be contributory – Increased cellular sensitivity to Types I and III collagen

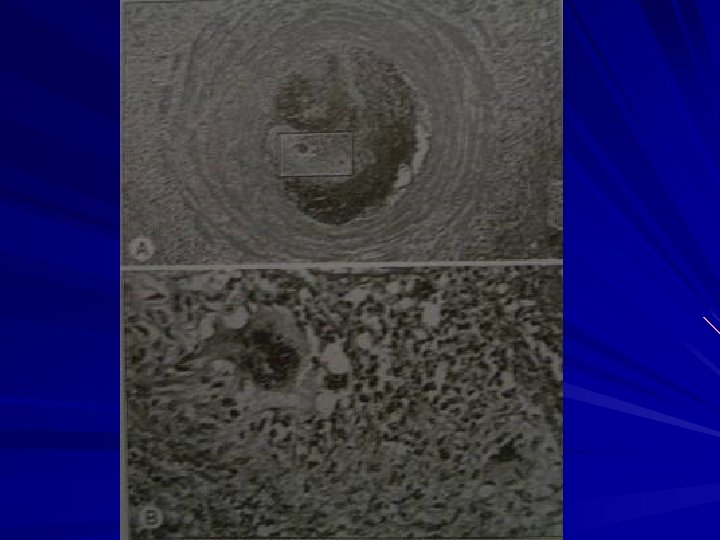
Pathology Inflammatory thrombosis that affects arteries and veins – Acute-phase Inflammation involving all layers of vessel wall with occlusive thrombosis Microabscesses & multinucleated giant cells – Intermediate phase Progressive organization of occlusive thrombus Prominent inflammatory infiltrate within thrombus – Chronic phase Extensive recanalization Adventitial & perivascular fibrosis Segmental in distribution – Skip areas noted – Rare to involve cerebral, coronary, renal, or mesenteric vessels Non-necrotizing involvement of vessel wall



Clinical Features Classic presentation – Young male smoker with onset of symptoms before age 40 -45 – Ischemia of distal small arteries and veins Cleveland Clinic 1990: presenting signs/symptoms in 112 patients intermittent claudication 63% rest pain 81% Ischemic ulcers 76% Thrombophlebitis 38% sensory findings 69% abnormal Allen’s test 63% Initial site of claudication is arch of foot Usually >2 limbs involved Not uncommon to see angiographic findings in asymptomatic limbs Upper extremity involvement distinguished from atherosclerosis

Clinical Features Classification Systems – Major Criteria Onset of distal extremity ischemic symptoms prior to aqe 45 Tobacco abuse Undiseased arteries proximal to brachial & popliteal Objective documentation of distal occlusive disease by plethysmography Exclusion of proximal embolic source, trauma, autoimmune disease, hypercoagulable state, atherosclerosis – Minor Criteria Migratory superficial phlebitis Raynaud’s syndrome Upper extremity involvement Instep claudication No typical lab abnormalities

Arteriography Involvement of small and medium-sized vessels – Digital arteries of fingers and toes – Palmar, plantar, tibial, peroneal, radial, and ulnar Segmental occlusive lesions More severe disease distally Corkscrew collaterals Normal proximal arteries


Treatment STOP ALL SMOKING! – Complete abstinence is the only way to stop progression of disease and prevent future amputation All otherapies are palliative – – – Prostaglandin (iloprost) Calcium channel blockers for vasospasm Pentoxifylline Sympathectomy Thrombolytic therapy Surgical revascularization Limited due to skip lesions and distal disease Usually <10% patients in series are bypass candidates – 5 year patency 49% in large series from Europe 67% in those that stopped smoking and 35% in smokers
 Amputation 43% No amputation 57%")
Outcomes Cleveland Clinic 1970 -1996 120 patients Smoking (n=68) Amputation 43% No amputation 57% Ex-smoking (n=52) Amputation 6% No amputation 94%

Nonatheroslerotic, segmental, inflammatory disease affecting small and medium sized arteries and veins of upper and lower extremities Typically occurs in younger males with heavy tobacco use Smoking cessation is key to therapy
- Slides: 15