Thoracolumbar Fractures Classification Models Fracture Management Case Illustrations

Thoracolumbar Fractures Classification Models Fracture Management Case Illustrations Kevin Chao, MD Stanford Neurosurgery

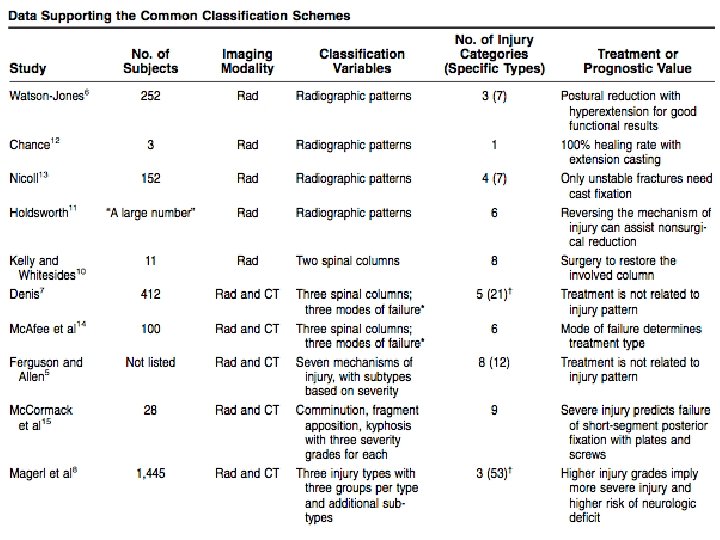
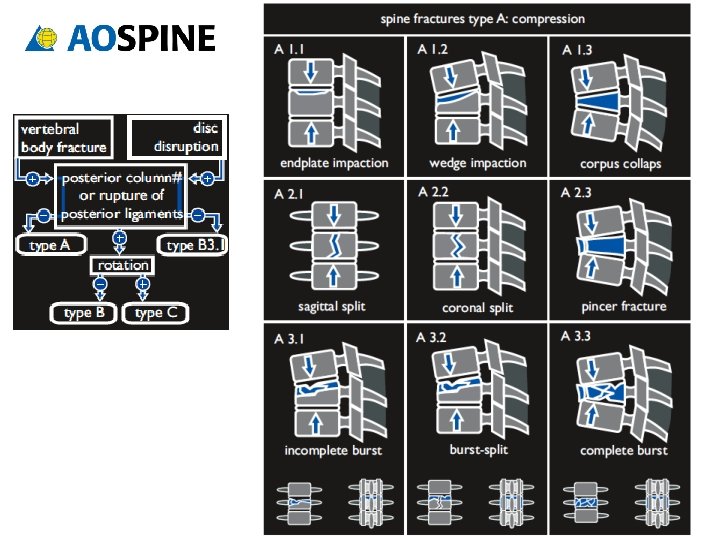
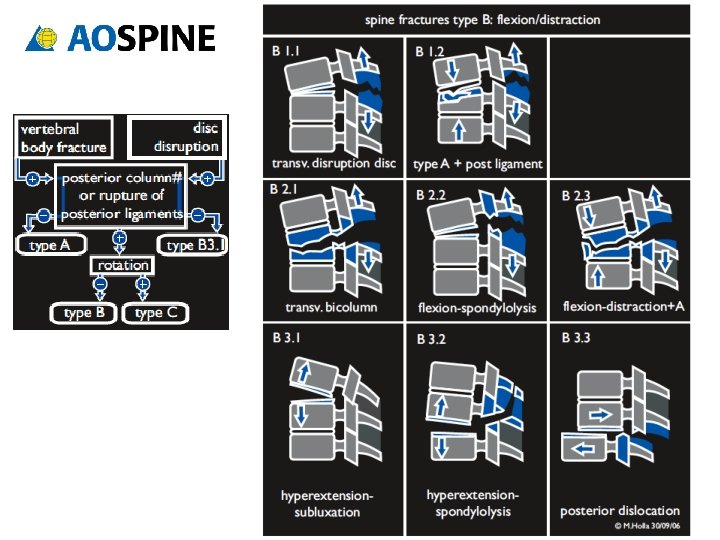
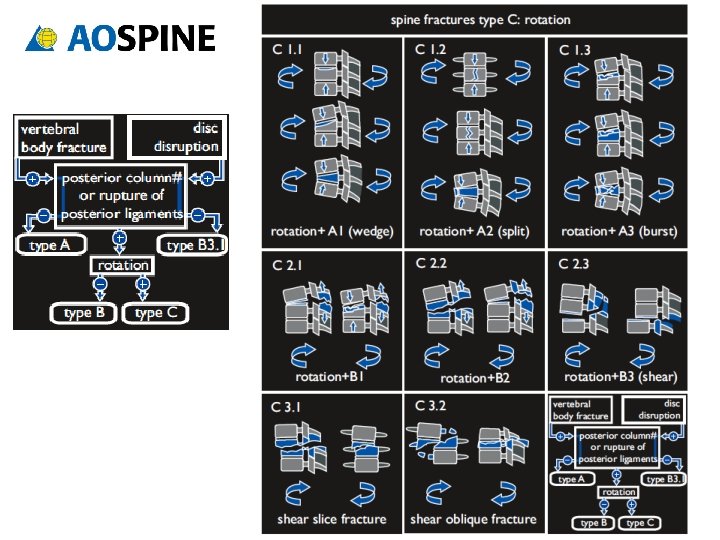
Classification Models Denis • Three-column ANATOMIC biomechanical model • Accounts for mechanism of injury • No rigid guidelines for treatment Magerl/ AO Spine • MECHANISTIC model • Detailed characterization of fracture subtypes Thoracolumbar Injury Classification and Severity Score (TLICS) • Accounts for 1) fracture morphology, 2) neurologic deficit, and 3) posterior complex status • Point-based system guides intervention (TLICS > 4)

Denis Three Column Model Anterior ALL Ant annulus Ant wall VB Middle PLL Post annulus Post wall VB Posterior SSL/ISL Posterior arch Facet capsule Ligamentum flavum
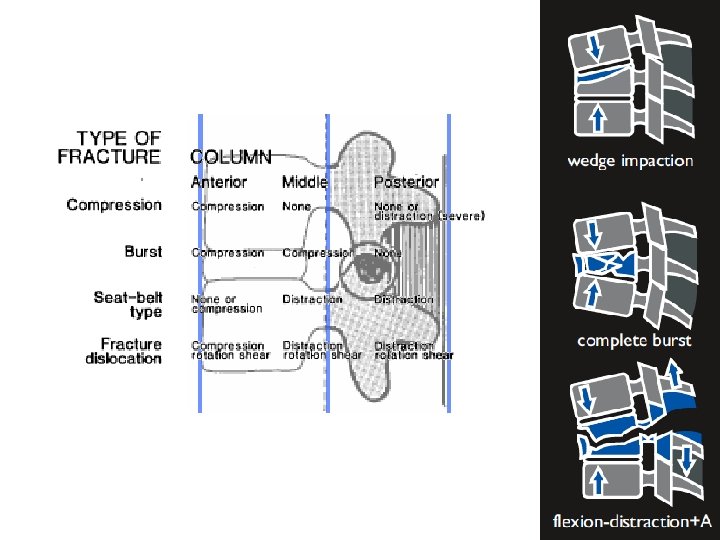

Seat belt-type injuries
 Fracture pattern % Acute neuro deficit Compression 0 Burst")
Denis Series Outcomes (412 pts) Fracture pattern % Acute neuro deficit Compression 0 Burst 48 Seat belt -type 0 Fracture dislocation 75 (52% complete) !! Denis gives NO RIGID PARAMETERS for treatment

TLICS TOTAL ___

ASIA Scale Poor prognosis Good prognosis

Spine Fracture Approach Assessment Management • Mechanism of injury • Neuro exam • Imaging • • – – Levels Bone vs soft tissue Dynamic vs static Vessels? • Degree of instability Surgery vs no surgery Goals? Brace? Activity restrictions • Follow up • Imaging • Rehab

Stable or Unstable? Overall degree of instability 1 st degree: Mechanical instability 2 nd degree: Neurological instability 3 rd degree: Both

Stable or Unstable? UNSTABLE > 50% height loss Minimal anterior column wedge > 20°angulation > 50% canal compromise* Neurologic deficit Progressive kyphosis Above T 8 if ribs and sternum intact Seat-belt type injuries without neurologic deficit

Fracture Management Goals: – Mechanical stabilization – Prevention of secondary neurologic injury – [ Decompression, if needed ] !! Instrumentation only serves as a bridge to fusion (or ligament healing)

Case files
")
35 M paragliding accident Motor - Right hip flexion pain-limited weakness (otherwise full strength) - Normal rectal tone Sensory - Right thigh to knee completely numb - Left knee and shin partly dumb - Saddle anesthesia Reflexes - Diminished at knees and ankles - No clonus 3 rd degree instability TLICS 5 (2+3+0) ASIA D L 2

Two-stage procedure Stage 1 Segmental instrumentation T 12 -L 4 Decompression Posterolateral fusion

Two-stage procedure Stage 2 Lateral corpectomy Interbody cage

Post op result Motor - Improved hip flexion - Able to walk Sensory - Unchanged Bracing - TLSO Follow up - 4 week repeat X rays

Teaching points • Recognize cauda equina syndrome • Define surgical goals • Many approach options (P, A/P, L/P) – Lateral approach technique • No abd surgery exposure needed • L 3 -T 12 (below L 3 often limited by iliac crest) • Rib resection +/- chest tube may be needed • Lumbar lordotic curve significant load bearing in middle and posterior columns

42 M fell from tree Motor - Full strength - Normal rectal tone Sensory - Intact to LT, proprioception, pin prick Reflexes - Normal at knees and ankles - No clonus 1 st degree instability TLICS 7 (4+0+3) ASIA E T 12

Sag CT recon Facet disruption MR Sag STIR Disc extrusion Ligament disruption MR Axial T 2 FS Canal hematoma Facet disruption

Post op result T 11 -L 2 posterolateral fusion Motor - Intact Sensory - Intact Bracing - TLSO Follow up - 6 week repeat X rays pending

Teaching points • Look beyond static image: What was the mechanism of injury? • Ligamentous injury >> bony injury • Ligamentous seat-belt-type fracture management options: – Open surgical instrumentation/fusion – Internal bracing (i. e. percutaneous instrumentation) – Bracing ?

22 M motorcycle crash Motor - 2/5 hip flexion and knee extension - 0/5 below knee - diminished rectal tone Sensory - Diminished sensation to light touch below knee Reflexes - None at knees and patella - No clonus 3 rd degree instability TLICS 9 (3+3+3) ASIA C

1 st attempt at surgery: Aborted due to sacral hemorrhage Wound packed Pelvic binder placed Sacral vessels embolized Transfused p. RBC, FFP, plts Returned to OR 2 days later…

Post op result L 1 -L 5 segmental instrumentation and posterolateral fusion Correction of fracture-dislocation using Wilson frame and reduction screws Motor - unchanged Sensory - some ROF below knees Bracing - TLSO Follow up - 6 week repeat X rays Not yet
")
Teaching points • Fracture-dislocations lead to majority of neurologic deficits from spine traumas (~50%) • Recognize other trauma injuries • Many spine fractures are URGENT (treat within 48 hours). Very few are EMERGENT (treat < 12 hours). – Wait for hemodynamically stability AMAP • Know fracture pattern/ anatomy preop • Be prepared for other injuries (thecal sac/ nerve roots, vascular, ureters, bowel, etc)

Teaching points • Can reduce some fractures with special OR tables (Wilson frame, Axis tilt, Jackson prone) • Reduction screws can be very helpful Reduction screw Wilson frame Axis-Jackson Table

Final point • TP fractures are not always benign – L 4 -5 TP fractures associated with lumbosacral plexus injury – T 1 -2 TP fractures associated with brachial plexus injury

References • Denis F. The Three Column Spine 1983; Vol. 8, No 8: 817 -831 – Classic historic paper with simple classification system – No rigid parameters for treatment • Patel A, Vaccaro A. Thoracolumbar Spine Trauma Classification. J Am Acad Orthop Surg 2010; 18: 63 -71 – New TLICS classification point system to guide treatment • http: //www. aospine. org/ – Pocket cards and protocols
- Slides: 34