Thoracic Outlet Syndrome TOS By Dr Khaled M
 By Dr. Khaled M. Abdel Aal MD Cardiothoracic surgery Associate")
Thoracic Outlet Syndrome (TOS) By Dr. Khaled M. Abdel Aal MD Cardiothoracic surgery Associate Prof. & Consultant of Cardiothoracic surgery Sohag University

Definition: TOS refers to compression of the subclavian vessels and brachial plexus at the superior thoracic aperture during their passage from the neck to the axilla.
: 1. Scalene syndrome. 2. costoclavicular syndrome. 3.")
Other names: (according to the presumed etiology): 1. Scalene syndrome. 2. costoclavicular syndrome. 3. hyperabduction syndrome, and 4. cervical rib syndrome Whatever the name and etiology most compressive factors operate against the first rib.

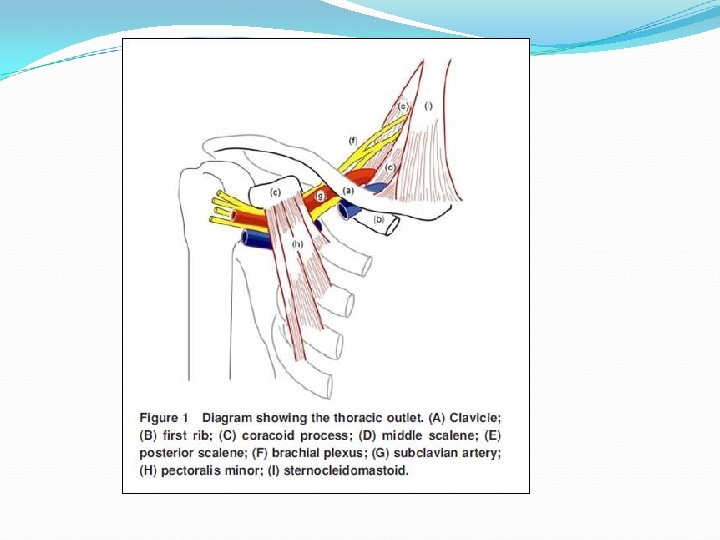
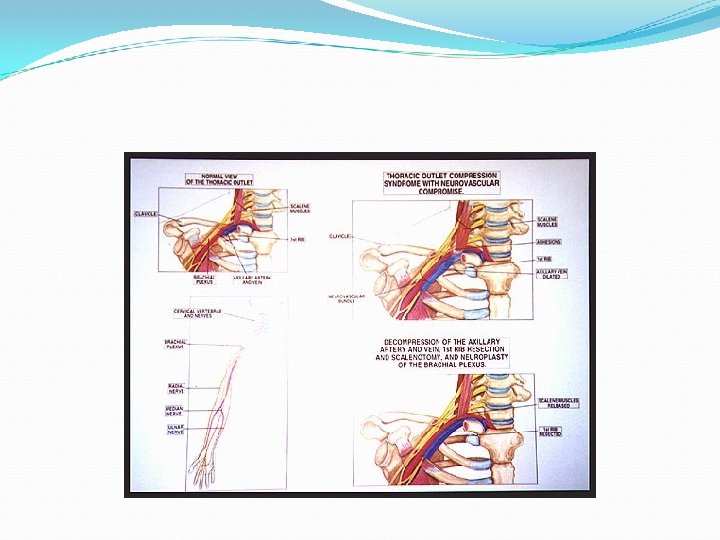
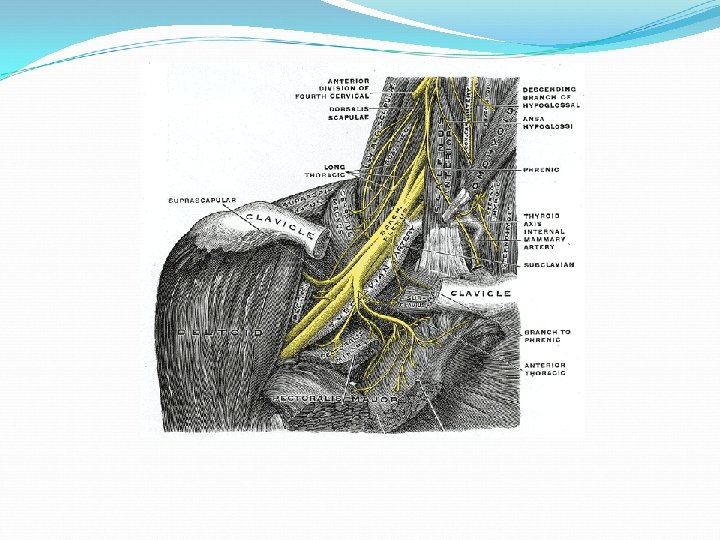
Surgical Anatomy: At the superior thoracic aperture, The brachial plexus and the subclavian Vs traverse the cervicoaxillary canal to reach the upper extremity. The cervicoaxillary canal is divided by the first rib into 2 sections: 1. the distal one (axilla) 2. the prximal section (scalene triangle and the costoclavicular space)
 The proximal division is the more critical for neurovascular compression.")
Surgical Anatomy: (cervicoaxillary canal) The proximal division is the more critical for neurovascular compression. Bounders: 1. superiorly: the clavicle 2. inferiorly: first rib 3. antromedially: costoclavicular lig. 4. postrolaterally: scalenus medius
 The scalinus anticus which inserts in the first rib divids")
Surgical Anatomy: (cervicoaxillary canal) The scalinus anticus which inserts in the first rib divids the costoclavicular space into: ----anteromedial part containing the subclavian vein ----postro lateral part (scalene triangle); contains the br. Plexus and subclavian artery

Pathophysiology The brachial plexus trunks and subclavian vessels are subjected to compression or irritation as they course through 3 narrow passageways from the base of the neck toward the axilla and the proximal arm. 1. The scalene triangle 2. the costoclavicular triangle 3. the subcoracoid space
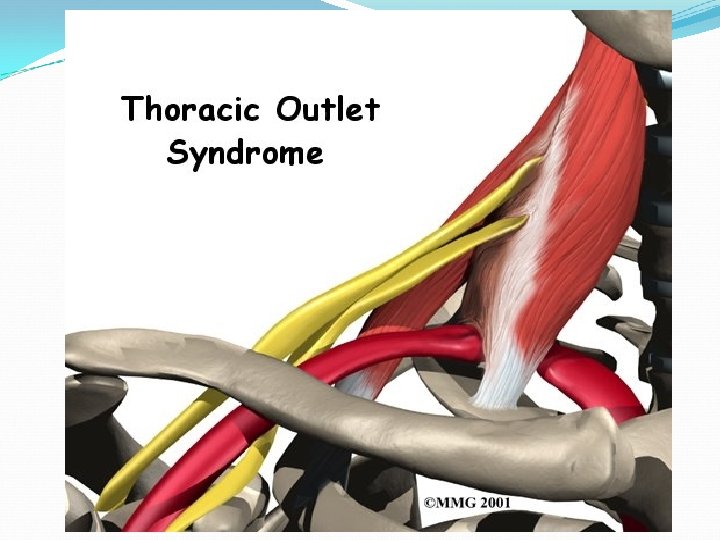

The scalene triangle The most important of these passageways which is also the most proximal Bounders : 1. the anterior scalene muscle anteriorly, 2. the middle scalene muscle posteriorly, 3. the medial surface of the first rib inferiorly

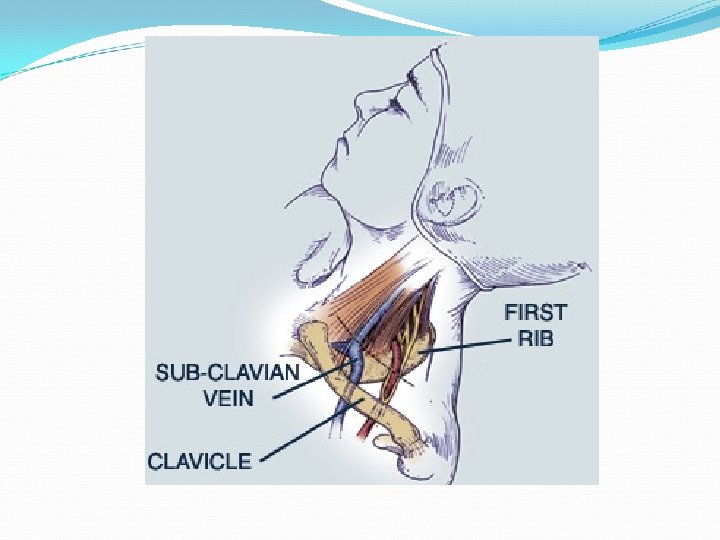
the costoclavicular triangle The second passageway Borders: 1. anteriorly by the middle third of the clavicle 2. posteromedially by the first rib, and 3. posterolaterally by the upper border of the scapula.

Subcoracoid space beneath the coracoid process just deep to the pectoralis minor tendon. In hyperabduction the neurovascular bundle is pulled around the pectoralis minor, the coracoid process, and the humerus head.

Causes: 1. 2. 3. Causes of TOS may be: Boney causes Muscular causes or neural
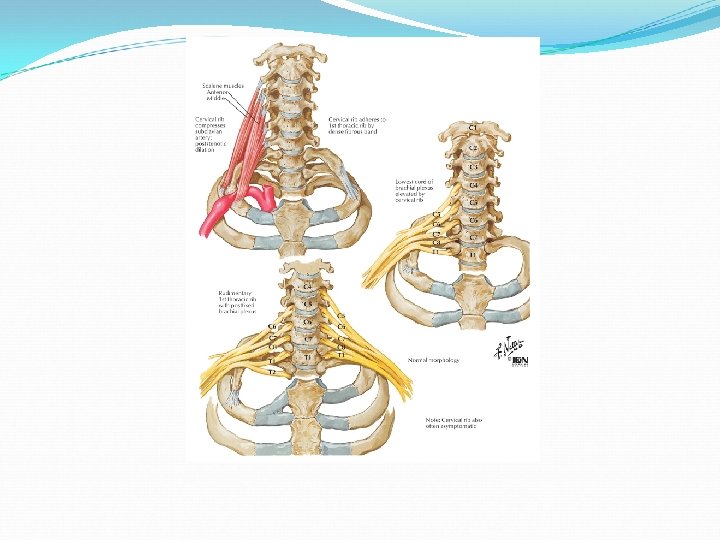
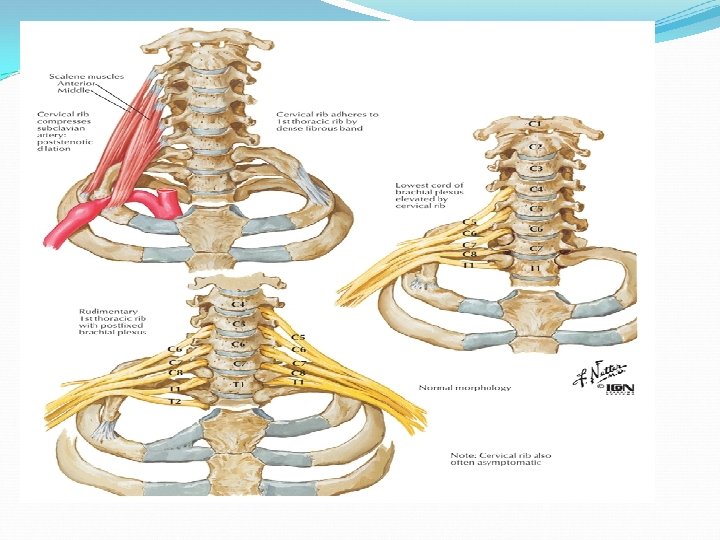
. boney causes: 1. cervical rib: arise from the last (7 th) cervical vertebrae,")
a). boney causes: 1. cervical rib: arise from the last (7 th) cervical vertebrae, may be: a. complete rib, b. incomplete with tapered end, c. just broadening of the transverse process, d. a fibrous band. 2. bifid or flat clavicle. 3. exostosis of the first rib or clavicle 4. dislocated humerus head 5. fracture clavicle
. muscular causes: 1. abnormal insertion of the scalene muscles that narrows the scalene")
b). muscular causes: 1. abnormal insertion of the scalene muscles that narrows the scalene triangle 2. presence of a rudimentary scalenus minimus muscle c). neural causes: post fixation of the brachial plexus

Clinical picture
 Neural Local")
Symptoms: 1. 2. 3. 4. Symptoms of TOS may be: Vascular (arterial) Neural Local or venous
. vascular symptoms: 1. Ischemic pain: intermittent on exercise, relieved by rest with")
Symptoms: a). vascular symptoms: 1. Ischemic pain: intermittent on exercise, relieved by rest with pallor, coldness, numbness, and parasthesia 2. Raynaud’s phenomenon 3. Embolic manifestations: gangrene due to post stenotic (compression)
. Nervous symptoms: Irritation of lower trunk C 8, T 1: ---- shooting")
Symptoms: b). Nervous symptoms: Irritation of lower trunk C 8, T 1: ---- shooting pain with tingling and numbness over the ulner side of the hand forearm. ----There may be atrophy of small muscles of the hands
. Local symptoms: - supraclavicular tenderness or - les commonly mass D). Venous")
Symptoms: c). Local symptoms: - supraclavicular tenderness or - les commonly mass D). Venous manifestations: Due to compression of the subclavian and axillary veins that leads to ------edema and varicosities and may be venous thrombosis
. physical examination: 1). Differences in pulse between the two arms (in volume).")
Signs: a). physical examination: 1). Differences in pulse between the two arms (in volume). 2). Decrease sensation, muscles weakness or atrophy. 3). May be palpable cervical rib or aneurismal dilatation at the root of the neck. 4). auscultation of the distal part of the subclavian artery may reveals systolic bruit.
. Diagnostic tests: 1. Adson’s test 2. Hyper abduction test 3. Hyper extention")
Signs: b). Diagnostic tests: 1. Adson’s test 2. Hyper abduction test 3. Hyper extention test (exaggerated position test) military

Provocative Maneuver Description Positive Results Supraclavicular Pressure Patient seated with arms § Test at side Examiner places fingers § on upper trapezius and thumb on anterior scalene near the first rib Examiner squeezes § fingers and thumb together for 30 seconds Adson’s Test Patient seated with arms § at side Examiner palpates the § radial pulse Patient inhales deeply § and holds the breath, extends and rotates the neck toward the side of testing Reproduction of pain or paresthesia Change in radial pulse and/or reproduction of pain or paresthesia
 -Loss of radial pulse by Adson’s deep breathing test.")
1. Adson’s test: (scalene test) -Loss of radial pulse by Adson’s deep breathing test. -The arm is pulled down, the radial pulse is palpated, while the patient is asked to extend the head and turn it toward the side of symptoms as far as possible and take a deep breath. -Positive test if the radial pulse become weak indicating compression on the subclavian artery.

2. Hyper abduction test: The arm is abducted 180 degrees and raised above the head and the effect on the radial pulse is noted The neurovascular bundle is pulled around the pectoralis minor, coracoid process and the humerus head
 The possibility of compression of the")
3. Hyper extension test: (exaggerated military position test) The possibility of compression of the neurovascular bundle between the first rib and the clavicle is tested by displacing the shoulder backward and down ward in an exaggerated military position, and seeing the effect on the radial pulse.

Differential diagnosis: 1. Cervical spondylosis 2. Cervical disc 3. Carpal tunnel syndrome 4. Medical neuropathy 5. Raynaud’s disease 6. Vasculitis, collagen disease

Investigations: 1. plain x – ray neck and chest: cervical rib, prominent transverse process or abnormal clavicle 2. CT chest and neck 3. nerve conduction velocity (NCV) 4. EMG (electromyography) 5. Doppler study 6. arteriography
 and EMG (Electromyography) This test s used for D. D.")
Nerve Conduction Velocity (NCV) and EMG (Electromyography) This test s used for D. D. of the causes of pain, numbness and tingling with or without motor weakness of the hand. These symptoms may result from at the thoracic outlet, around the elbow and at he wrist.
 and EMG (Electromyography) For diagnosis (method): cathodal stimulation is applied")
Nerve Conduction Velocity (NCV) and EMG (Electromyography) For diagnosis (method): cathodal stimulation is applied at various points along the nerve, motor conduction velocity across the Ulner, radial and median nerves can be used reliably. Conduction velocity over the proximal and distal segments of the ulner nerve are determined by recording the action potential generated in thenar and hypothenar ms.
 and EMG (Electromyography) The points of stimulation are: ---spraclvicular fossa")
Nerve Conduction Velocity (NCV) and EMG (Electromyography) The points of stimulation are: ---spraclvicular fossa ---middle of the upper arm ---below the lbow ---at the wrist Normal values of UNCV: ---72 m/s or above across the thoracic outlet ---55 m/s or above around the elbow ---59 m/s or above at the forearm ---wrist delay is 2. 5 – 3. 5 m/s
 and EMG (Electromyography Dcrease velocity in a segment or increase")
Nerve Conduction Velocity (NCV) and EMG (Electromyography Dcrease velocity in a segment or increase wrist delay indicate compression e. g. : 1. decrease velocity at outlet------TOS 2. Decrease velocity around elbow----ulner nerve entrapment 3. increase wrist delay ----carpal tunnel syndrome

Treatment
. no symptoms: no treatment b). conservative treatment (medical treatment): In mild cases")
treatment a). no symptoms: no treatment b). conservative treatment (medical treatment): In mild cases i. Anti- inflammatory drugs ii. Vasodilators iii. Neck and shoulder physiotherapy
. surgical treatment: Indications: i. sever pain ii. muscle wasting iii. vascular disturbances iv.")
c). surgical treatment: Indications: i. sever pain ii. muscle wasting iii. vascular disturbances iv. failed medical treatment
. surgical treatment: In the form of: Sclenotomy or sclenectomy Excision of the cervical")
c). surgical treatment: In the form of: Sclenotomy or sclenectomy Excision of the cervical rib with its periostium Excision of the first rib Sympathectomy or neurolysis of the brachial plexus

Surgical approaches for excision of the first rib and cervial rib Transaxillary--- the best Anterior approach Posterior thocoplasty approach

Thank you
- Slides: 44