Thoracic aortic disease Kittichai Luengtaviboon 21 January 2011

Thoracic aortic disease Kittichai Luengtaviboon 21 January 2011

� Thoracic aortic disease is more common in the last decade world wide. Because increasing life expectancy better diagnostic tools – CTA, MRA more public awareness high incidence of systemic arterial hypertension most patients with hypertension are untreated or inadequately treated. � It usually results in deaths from rupture or dissection, even the growth of aneurysm is slow initially in the asymptomatic period. If the patient does not die from other causes. introduction

�Natural history of thoracic aortic aneurysms – one of progressive expansion and weakening of the aortic wall, leading to eventual rupture. With as associated mortality of 94%. � 5 year survival rate of unoperated TAA 13%. �Whereas 70 -79% of those who undergo elective surgical intervention are alive at 5 years.

�>60 m diameter or > 2 x transverse diameter of an adjacent normal aortic segment �Symptomatic regardless of size �Growth rate of aneurysm > 3 mm/y Circulation 2005; 112: 1663 -1675. Indication for TAA repair

� 1 aneurysm � 2 dissection and acute aortic syndrome � 3 nonspecific aortitis or Takayasu’s disease � 4 aortic trauma � 5 aortic infection Common thoracic aortic problems in Thailand

�Classification – anatomical ascending – root, tubular part arch descending type A, B and C thoraco abdominal Crawford 1 -4 �Etiology atherosclerotic hereditary chronic dissection others – infection, trauma, inflammatory Thoracic aortic aneurysm
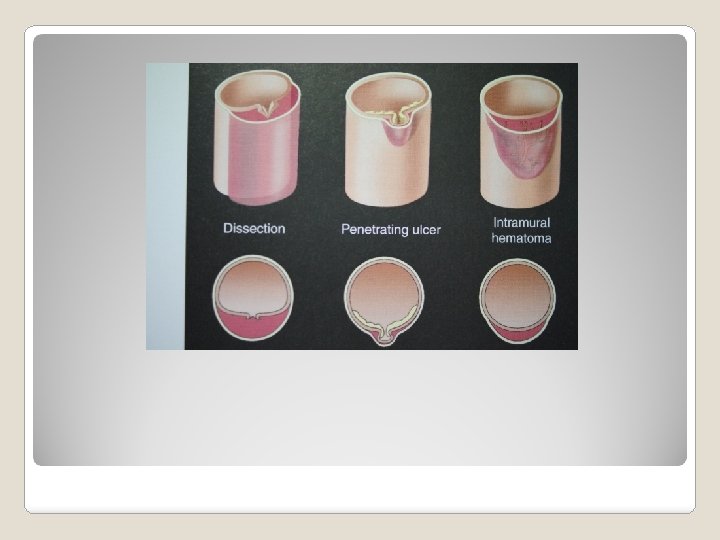

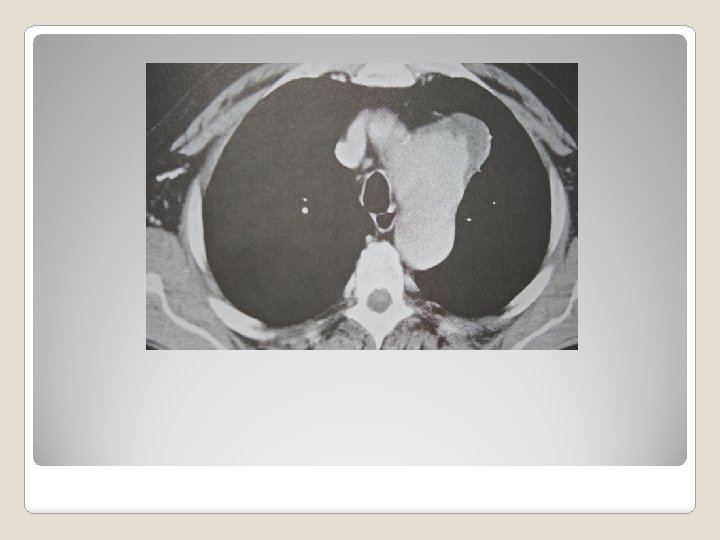
�There are three common types acute aortic dissection intramural hematoma penetrating aortic ulcer �Common etiologic factors hypertension older age atherosclerosis genetic disorder – Marfan, Ehler Danlos, Turner, Loeys Dietz Acute aortic syndrome

�Aneurysm common indication in all location presence of symptoms pain compressive symptom maximal diameter non marfan and others dissection or non dissection rapid increase in maximal diameter saccular aneurysm Indication for surgery in thoracic aortic disesease

� Acute aortic syndrome require prompt diagnosis and treatment life threatening etiology acute dissection type comorbid, patient’s condition intramural hematoma same as dissection but no problems with malperfusion PAU treatment in all patients with symptoms if no symptoms – controversial- size and depth indication

� 4 types, most common due to infected aortitis � Gold standard open resection with insitu graft replacement � TEVAR still need more evidence BUT recurrent infection is high. More appropriate if used as a bridge. But may make open surgery more difficult and very costly. � Comtemporary result of open repair is promising! � Recurrent infection after open repair is LOW. And operative mortality is NOT HIGH. � In situ graft is safe even in some condition extra anatomical bypass is feasible. Thoracic aortic infection
 decreasing")
Open repair gold standard for all segment ( descending aorta ? ) decreasing mortality, morbidity in early post operative period. good long term outcome long lasting good result TEVAR evidence based support its use in descending aorta Option for treatment of thoracic aortic diseases

�Class 1 1 separate valve and ascending aortic replacement in patients without root dilatation if ascending aorta > 5 cm with aortic valve disease © 2 Marfan, Ehlers Danlos, Loeys-Dietz with dilatation of aortic root -> David or mod. Bentall’s operation (B) Recommendations for open surgery for ascending aortic aneurysm

� Class 2 a ascending aneurysm with proximal arch involvement –partial arch with ascending aortic replacement using right subclavian/axillary inflow and hypothermic circulartory arrest is reasonable. (B) patients with low operative risk, with degenerative or atherosclerotic aneurysm of arch, operative treatment is reasonable for asymptomatic patients when diameter > 5. 5 cm. (B) No recommedation about using Hybrid TEVAR in arch aneurysm. Recommendation for aortic arch aneurysm

�Class 1 chronic dissection without significant comorbid -> open repair if diameter >5. 5 cm (B) degenerative, traumatic aneurysm, diameter > 5. 5 cm -> TEVAR if feasible (B) Recommendation of treatment of descending thoracic aortic aneurysm
 Entity/Subgroup Classification Level")
Society of Thoracic Surgeons Recommendations for Thoracic Stent Graft Insertion (summary) Entity/Subgroup Classification Level of Evidence Asymptomatic III C Symptomatic IIa C I B IIa C I A No ischemia IIb C Subacute dissection IIb B Chronic dissection IIb B >5. 5 cm, comorbidity IIa B >5. 5 cm, no comorbidity IIb C <5. 5 cm III C Reasonable open risk III A Severe comorbidity IIb C Thoracoabdominal/Severe comorbidity IIb C Penetrating ulcer/intramural hematoma Acute traumatic Chronic traumatic Acute Type B dissection Ischemia Degenerative descending Arch Note: Table 15 in full-text version of TAD Guidelines. Reprinted from Svensson et al. Expert consensus document on the treatment of descending thoracic aortic disease using endovascular stent grafts. Ann Thorac Surg. 2008; 85: S 1– 41.

� Joseph E. Bavaria et al � J Thorac Cardiovasc Surgery 2007; 133: 369 -77. � The first completed multicenter trial directed at gaining approval from the US Food and Drug Administration. � From Sep 1999 and May 2001 140 patients with descending thoracic aortic aneurysms enrolled at 17 sites and evaluated for Gore TAG thoracic endograft � Compared to open surgical control cohort of 94 patients (enrolling historical and concurrent subjects) Endovascular stent grafting versus open surgical repair of descending thoracic aortic aneurysms in low risk patients: a multicenter comparative trial

�Perioperative mortality and morbidity were significantly less with TEVAR �Overall stroke rate was similar �Reintervention rate and continued presence of complications, such as endoleaks, is higher in the endograft group. �No survival advantage associated with either strategy after 2 years of follow up. conclusion

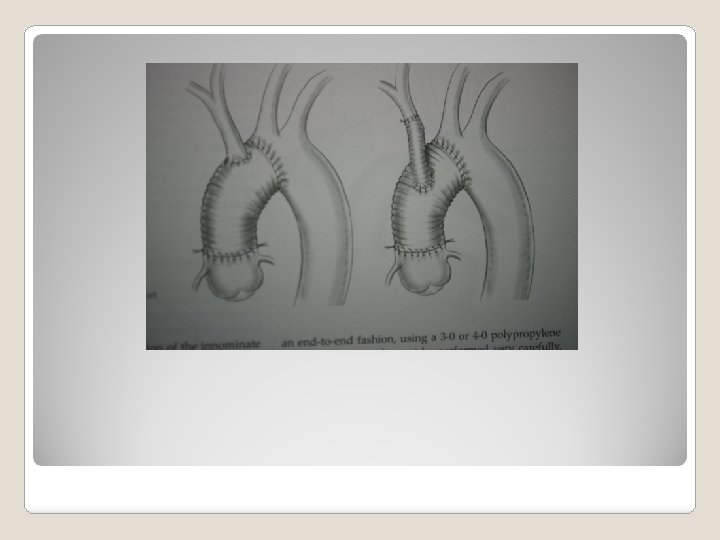
�Ascending aorta involve root – modified Bentall or David not involve root – replace aorta above sinotubular junction Techniques in open repair of thoraic aortic aneurysms

�If with ascending, but no descending – median sternotomy canulate left femoral or left common carotid artery canulate RA for venous return use cardioplegia use DHCA alone or with ACP hemiarch technique preserving greater curve of arch Aortic arch

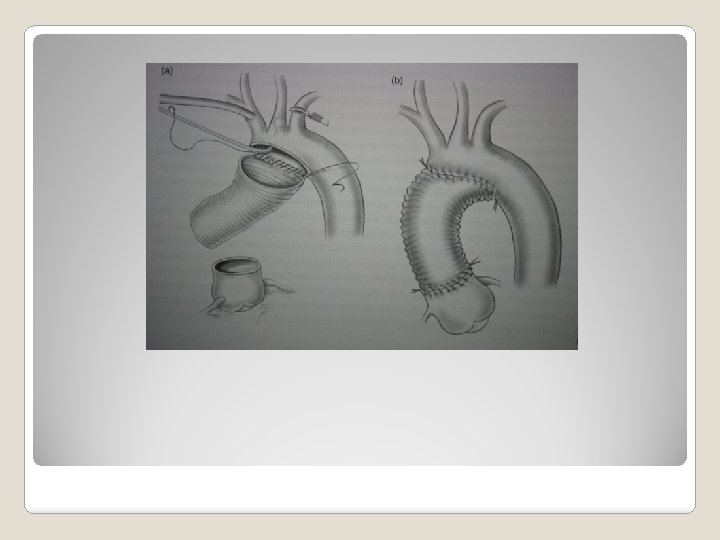
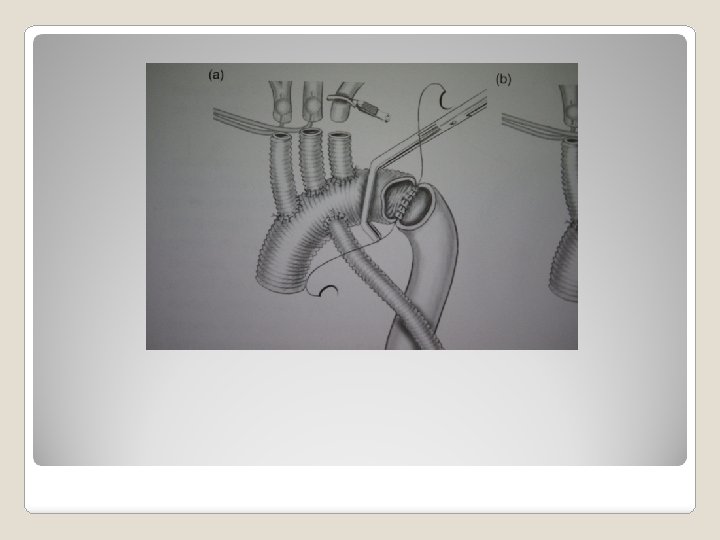
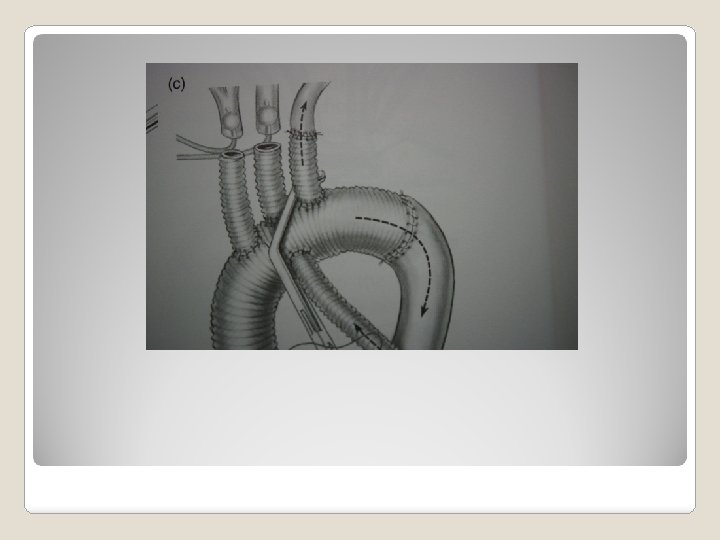
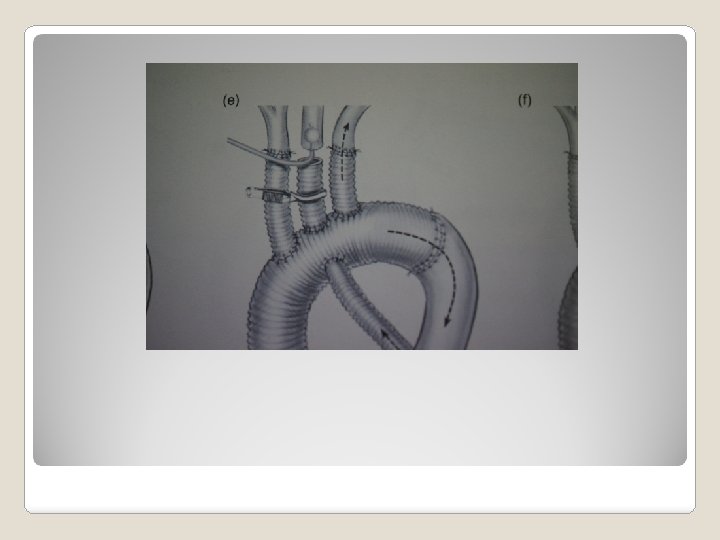
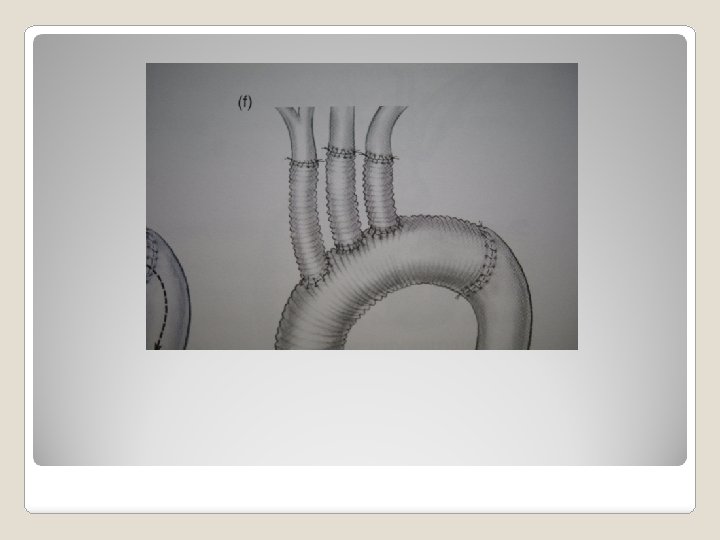
�Incision – median �Cannulation sternotomy arterial – ascending aorta, right subclavian, left common carotid, femroal A venous – right atrium �Technique of arch replacement island – arch first individual arch branch Total arch replacement

�Incision – clamshell �Canulation ascending aorta, femoral artery venous right atrium Ascending, arch and descending aortic aneurysms

�Incision left posterolateral thoracotomy �Use DHCA Descending aorta type A or C

�Incision – left posterolateral thoracotomy �Technique clamp and go femoral vein- descending aorta partial CPB shunt left atrio femoral bypass with centrifugal pump Descending aorta type B
- Slides: 33