THIRD STAGE OF LABOUR DEFINITION Third stage is

THIRD STAGE OF LABOUR

DEFINITION Third stage is that separation and expulsion of the placenta and membranes and also involves the control of bleeding

q EVENTS IN THE THIRD STAGE OF LABOUR ü Seperation and expulsion of the placenta ü Interplay of mechanical and hemostatic factors q TIME ü Last between 5 and 15 minutes

PHYSIOLOGY OF THIRD STAGE OF LABOUR/CONTROL OF HEMOSTASIS Separation and descend of the placenta q Mechanical factors q Hemostasis

MECHANICAL FACTORS q Seperation of the placenta q Expulsion of the placenta

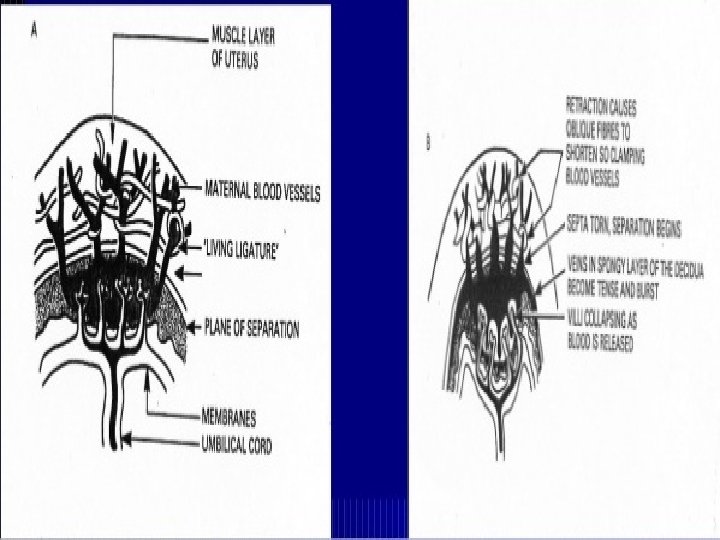
MECHANICAL FACTORS……Contd PLACENTAL SEPERATION 1. Second stage uterine cavity empties 2. Enabling the retraction process to accelerate (1 & 2)Placental site has already begun to diminish in size Placenta becomes compressed Blood in the intervillous space is forced back into the spongy layer of the decidua

MECHANICAL FACTORS…. . Contd Retraction of the oblique uterine muscle fibres exert pressure on the blood vessels so that the blood does not drain back into the maternal circulation Vessels during this process become tense and congested With the next contraction the distended veins burst and a small amount of blood seeps between the spongy layer and placental surface Placenta strip from its attachment Surface area of placental attachment reduces and begin to detach from the uterine wall

MECHANICAL FACTORS…. . Contd Retraction of the oblique uterine muscle fibres exert pressure on the blood vessels so that the blood does not drain back into the maternal circulation Vessels during this process become tense and congested With the next contraction the distended veins burst and a small amount of blood seeps between the spongy layer and placental surface Placenta strip from its attachment Surface area of placental attachment reduces and begin to detach from the uterine wall


MECHANICAL FACTORS……Contd METHODS OF PLACENTAL SEPERATION q. Schultze Method q Matthews Duncan

SEPERATION BEGINS CENTRALLY Retroplacental clot is formed Aids further seperation by exerting pressure at the midpoint of the placental attachment Increased weight helps to strip the adherent lateral borders Increased weight also helps to peel the membrane of the uterine wall Clot formed becomes enclosed in the membranous bag Placenta descends with fetal surface first More complete shearing of both placenta and membrane Less blood loss

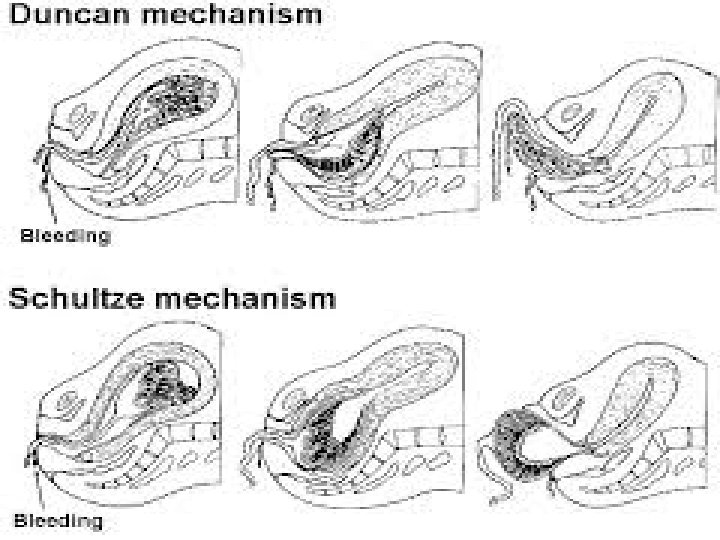

SEPERATION BEGINS LATERALLY Detach unevenly at one of its lateral borders Blood escapes so that seperation is unaided by the formation of a retroplacental clot Placenta descends, slipping sideways Maternal surface comes out first Takes longer time Associated with ragged, incomplete expulsion of the membranes Higher fluid blood loss

TWO METHODS OF PLACENTAL SEPERATION

HAEMOSTASIS q RETRACTION OF THE OBLIQUE UTERINE MUSCLE FIBER q. PRESENCE OF VIGOROUS UTERINE CONTRACTION q ACTIVATION OF THE COAGULATION AND FIBRINOLYTIC SYSTEM

LIVING LIGATURE ACTION OF OBLIQUE UTERINE MUSCLES

MANAGEMENT OF THE THIRD STAGE OF LABOUR q Guard the uterus from massaging prior to placental seperation q Do not massage the uterus before placental expulsion except when partial seperation q Do not pull the umbilical cord before placenta separates q Do not try to deliver the placenta prior to its complete seperation unless in the emergency of third stage haemorrhage q Wait for the natural process to occur

DELIVERY OF THE PLACENTA AND MEMBRANE q Fundus is palpable below the umbilicus q Fundus feels broad as the placenta is still in the upper segment SIGNS OF PLACENTAL SEPERATION

DELIVERY OF THE PLACENTA AND MEMBRANE……Contd METHODS OF PLACENTAL DELIVERY 1. EXPECTANT MANAGEMENT 2. ASSISTED EXPULSION Ø Controlled cord traction (modified Brandt – Andrews method) Ø Expression by fundal pressure

EXPECTANT MANAGEMENT q Placental seperation and descent occur spontaneously q Mothers efforts are used to aid expulsion q Minimal assistance is given if mothers effort fails to deliver the placenta q Method can be practiced when mother has not received any anesthesia or oxytocic drugs at the delivery of the anterior shoulder

EXPECTANT MANAGEMENT STEPS OF THE PLACENTAL DELIVERY 1. A hand is placed over the fundus to feel for the signs of placental seperation 2. When the features of placental seperation and its descend into the lower segment are confirmed, the client asked to bear down simultaneously with the hardening of the uterus 3. As soon as the placenta passes through the introitus, it is grasped by both hands and twisted round and round or slightly up and down with gentle traction applied as the membranes are stripped off intact 4. If the membranes are threatened to tear, they are to be held by an artery forceps and gentle traction is applied to deliver the rest of the membranes

STEPS OF THE PLACENTAL DELIVERY 1. A hand is placed over the fundus to feel for the signs of placental seperation 2. When the features of placental seperation and its descend into the lower segment are confirmed, the client asked to bear down simultaneously with the hardening of the uterus 3. As soon as the placenta passes through the introitus, it is grasped by both hands and twisted round and round or slightly up and down with gentle traction applied as the membranes are stripped off intact 4. If the membranes are threatened to tear, they are to be held by an artery forceps and gentle traction is applied to deliver the rest of the membranes
 q Several checks to")
ASSISTED EXPULSION CONTROLLED CORD TRACTION (MODIFIED BRANDT – ANDREWS METHOD) q Several checks to be made before proceeding 1. An oxytocic drug has been administered 2. It has been given time to act 3. The uterus is well contracted 4. Counter traction is applied 5. The signs of placental seperation and descend are present
 1. The")
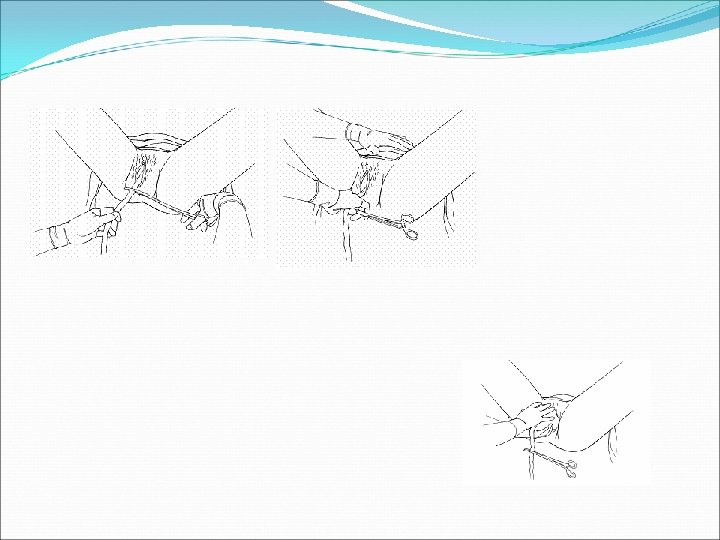
ASSISTED EXPULSION……Contd METHODS OF CONTROLLED CORD TRACTION (MODIFIED BRANDT – ANDREWS METHOD) 1. The left hand is placed above the level of the symphysis pubis 2. Palmar surface facing toward the umbilicus to exert pressure in an upward direction 3. Body of the uterus is displaced upward towards the umbilicus with left hand 4. With the right hand a steady tension is given in a downward and backward direction following the line of birth canal by holding on the clamp placed on the cord at the vulva 5. It is important to apply a steady traction by pulling the cord firmly 6. There should be a pause before another contraction is palpated and further attempt is made

Controlled cord traction
 1. Inversion")
ASSISTED EXPULSION……Contd COMPLICATIONS OF CONTROLLED CORD TRACTION (MODIFIED BRANDT – ANDREWS METHOD) 1. Inversion of the uterus 2. Partial seperation of the placenta 3. Haemorrhage 4. Detachment of cord
 1. Reduced")
ASSISTED EXPULSION……Contd ADVANTAGES OF CONTROLLED CORD TRACTION (MODIFIED BRANDT – ANDREWS METHOD) 1. Reduced blood loss 2. Reduction in third stage of labour

ASSISTED EXPULSION EXPRESSION BY FUNDAL PRESSURE 1. Place four fingers of the hand behind the fundus and the thumb in front of the fundus to use as a piston 2. The uterus is made to contract by gentle rubbing 3. When the uterus is hard it is pushed downwards and backwards 4. The pressure is to be withdrawn as soon as the placenta passess through the introitus

USE OF OXYTOCIC AGENT TIME OF ADMINISTRATION Ø At the crowning of the baby’s head Ø At the delivery of the anterior shoulder Ø At the end of second stage of labour Ø Following the delivery of the placenta PROPHYLACTIC USE Ø Prevention of post partum haemorrhage Ø Active management of third stage of labour THERAPEUTIC USE Ø Ergometrine 0. 5 mg IM Ø Methergin 0. 2 mg IM

FUNDAL HEIGHT DURING THIRD STAGE Ø At the beginning fundus palpable below the umbilicus, feels broad as the placenta still in the upper segment Ø As the placenta separates, becomes rounder, smaller and more mobile as it rises in the abdomen to the level of umbilicus or just above the level of umbilicus Ø At the end of third stage fundus is about 4 cm below the umbilicus

COMPLETION OF THE THIRD STAGE Ø Ensure that uterus is well contracted Ø Fresh blood loss is minimal Ø Inspection of the perineum and the lower vagina Ø Suture the episiotomy or any slight laceration Ø Change all the soiled linen Ø Cleanse the perineum Ø Application of sterile pad Ø Examination of the placenta membrane
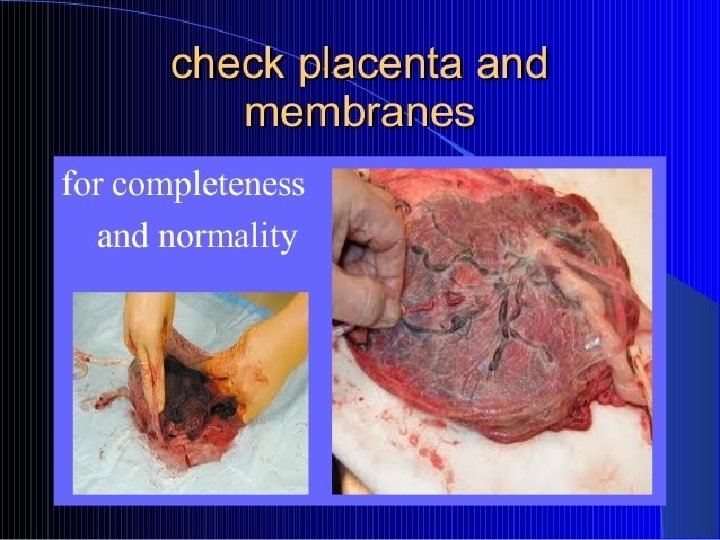
 or old(gray patches) Ø")
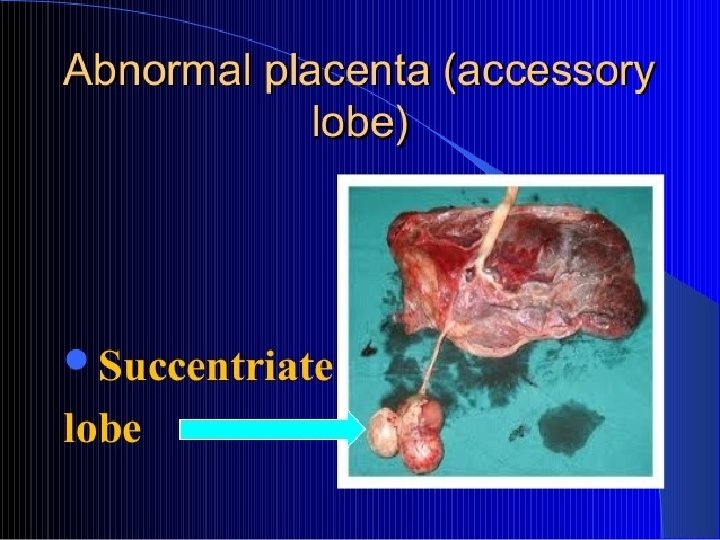
ASSESSMENT OF THE PLACENTA Ø Infractions that are recent(bright red) or old(gray patches) Ø Localised calcification(flattened white plaques) Ø Lobes Ø Blood vessels Ø Insertion of the cord Ø Umbilical vessels Ø Cord length Ø Weight of the placenta

IMMEDIATE CARE OF BABY Ø Well being and security Ø Cord clamp need to be checked Ø Warmth Ø Full neonatal assessment Ø Baby kept close to the mother Ø Breast feeding

IMMEDIATE CARE OF MOTHER Ø Cleansing the body Ø Mouth wash Ø Empty her bladder Ø Vital signs Ø Bleeding checked every 15 minutes
- Slides: 39