Thi Qar college of Medicine Family Community medicine


 HTN 2) Atrial fibrillation AF 3) DM 4) Carotid artery")
 Screen and treat BP to <")

 -Asymptomatic CAS : Medical treatment of asymptomatic CAS should be")





 -One-time screening for AAA by ultrasonography for men aged 65")
 Children aged 7– 11 years Insufficient evidence to recommend for or against")
 Adults: Recommend screening adults for depression -Asking two simple mood questions(Prime-MD)may be as")

 Assess: Ask about or assess")

- Slides: 26
Thi. Qar college of Medicine Family & Community medicine dept. Family Medicine Lec 6 post graduate-FAMCO prepared by: Dr. Muslim N. Saeed Sunday, December 14 th , 2014
Stroke Endocarditis Abdominal Aortic Aneurysm Depression Tobacco use
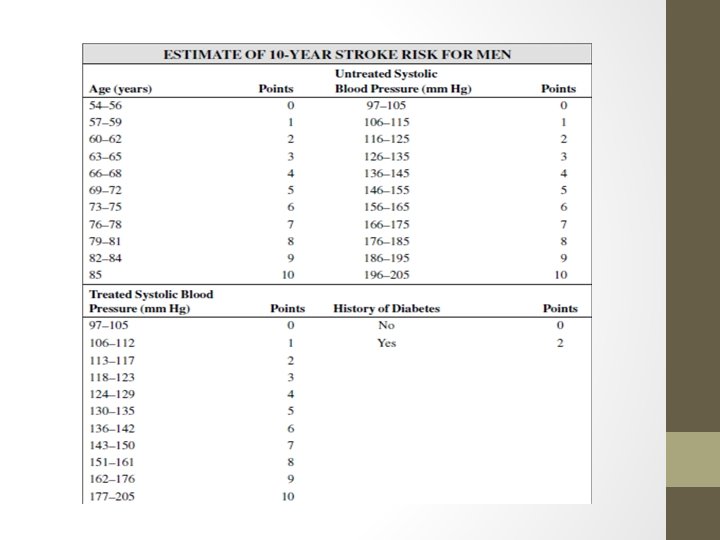
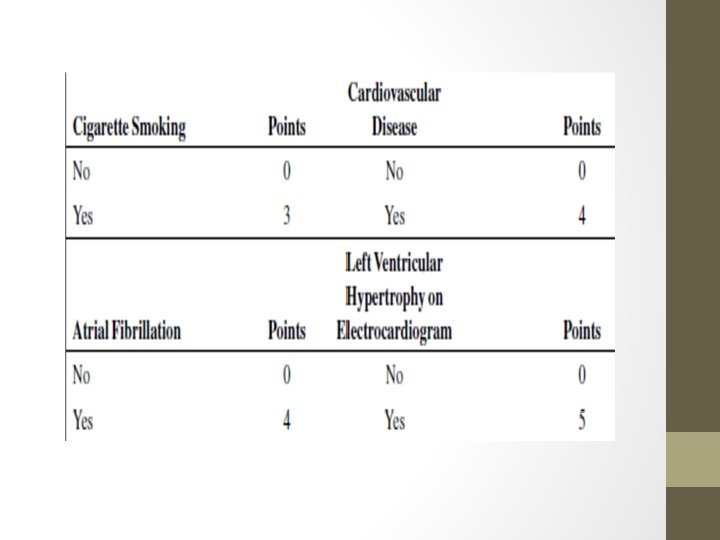
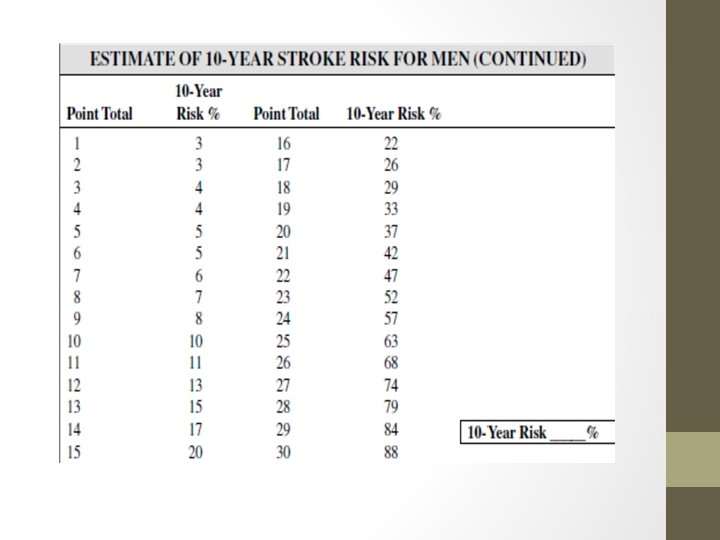
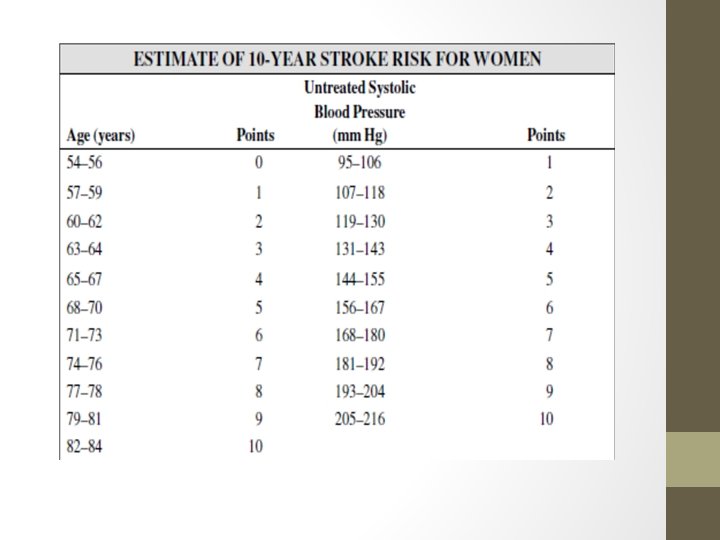
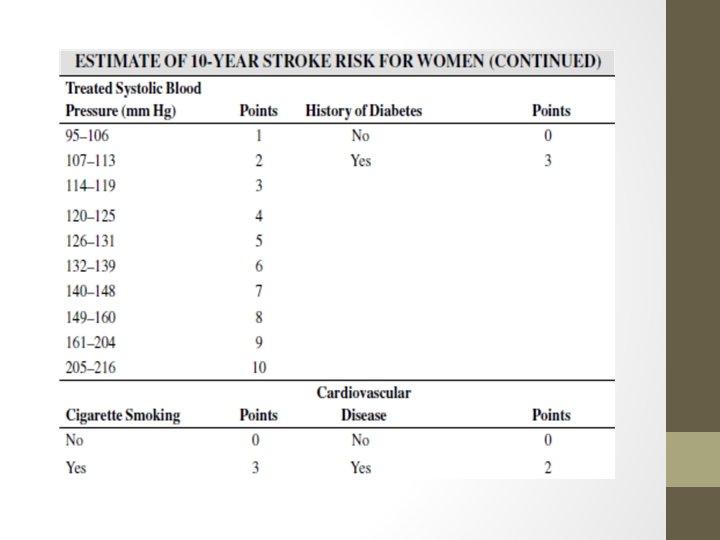
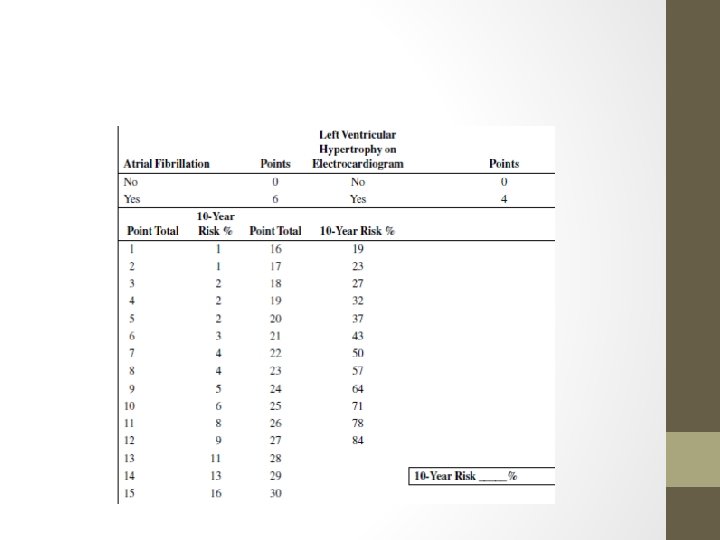
Stroke associated with: 1) HTN 2) Atrial fibrillation AF 3) DM 4) Carotid artery stenosis 5) Sickle cell disease 6) Hyperlipidemia 7) Smoking Risk assessment tool of stroke :
Recommendations -Treat all known CV risk factors 1) Screen and treat BP to < 140/90 mm Hg. If HTN with diabetes or renal disease, treat to < 130/80 mm Hg. 2) Atrial fibrillation - Prioritize rate control; consider rhythm control if this is the first event, if it occurs in a young patient , or if symptomatic. -Rate control goal is < 110 beats per minute. -Antithrombotic therapy is required, anticoagulation or antiplatelet therapy accordingly (previous TIA or stroke or embolus, HTN, poor left ventricular function, age > 75 years, DM, rheumatic mitral valve disease, and prosthetic heart valves.
DM 1. Six-fold increase of stroke. 2. Short-term glycemic control does not lower macro-vascular events. 3. Hg. A 1 c goal is < 6. 5%. 4. BP goal is < 130/80 mm Hg. 5. Statin therapy. 6. Consider ACE inhibitor or ARB therapy for further stroke risk reduction.
Carotid artery stenosis (CAS) -Asymptomatic CAS : Medical treatment of asymptomatic CAS should be aggressive. -Symptomatic CAS Optimal timing for Carotid end arterectomy CEA is within 2 weeks post-transient ischemic attack.
Hyperlipidemia: Statin therapy post-CVA with intensive lipid-lowering goal after an ischemic stroke or transient ischemic attack with or without CHD reduced the risk of stroke and CV events.
Sickle cell disease -Transfusion therapy is recommended for patients at high-stroke risk. Smoking: counseling of smokers.
Endocarditis is more likely a result of random exposure to bacteremia rather than associated with procedures. Certain persons are at highest risk for adverse sequelae from endocarditis: 1) Patients with prosthetic valves 2) previous endocarditis 3) selected patients with congenital heart disease. 4) Cardiac transplant recipients who develop valvulopathy.
Recommendations Give antibiotic prophylaxis before certain dental as well as certain other procedures(All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of oral mucosa). Antibiotic prophylaxis is recommended for procedures in the respiratory tract or infected skin, skin structures, or musculoskeletal tissue in high-risk patients. Antibiotic prophylaxis for genitourinary (GU) or gastrointestinal (GI) procedures is indicated with ongoing infection.
Standard prophylaxis regimen: -amoxicillin (adults 2. 0 g; children 50 mg/kg orally 1 hour before procedure). -If unable to take oral medications, give ampicillin (adults 2. 0 g IM or IV; children 50 mg/kg IM or IV within 30 minutes of procedure). -If penicillin-allergic, give clindamycin (adults 600 mg; children 20 mg/kg orally 1 hour before procedure) or azithromycin or clarithromycin (adults 500 mg; children 15 mg/kg orally 1 hour before procedure). -If penicillin-allergic and unable to take oral medications, give clindamycin (adults 600 mg; children 20 mg/kg IV within 30 minutes before procedure). -options for non oral treatment also include cefazolin (1 g IM or IV for adults, 50 mg/kg IM or IV for children), oral therapy includes cephalexin 2 g PO for adults or 50 mg/kg PO for children.
Abdominal Aortic Aneurysm (AAA) -One-time screening for AAA by ultrasonography for men aged 65 – 75 years who have ever smoked, or who have a family history of AAA. -routine screening is not recommended for women.
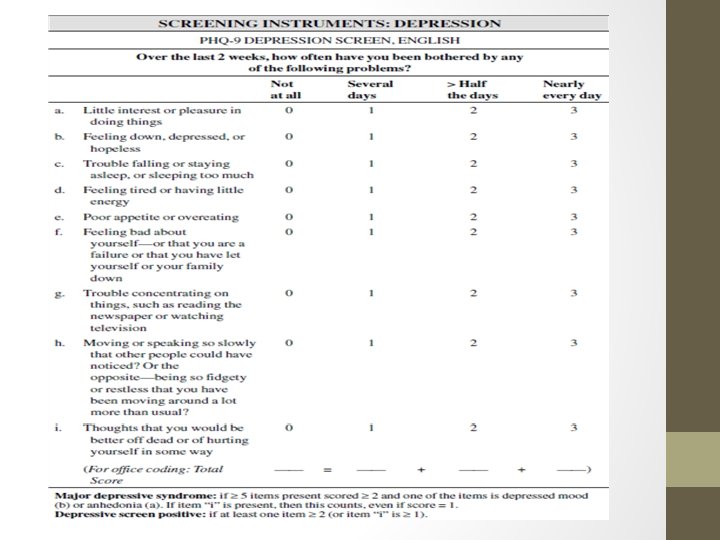
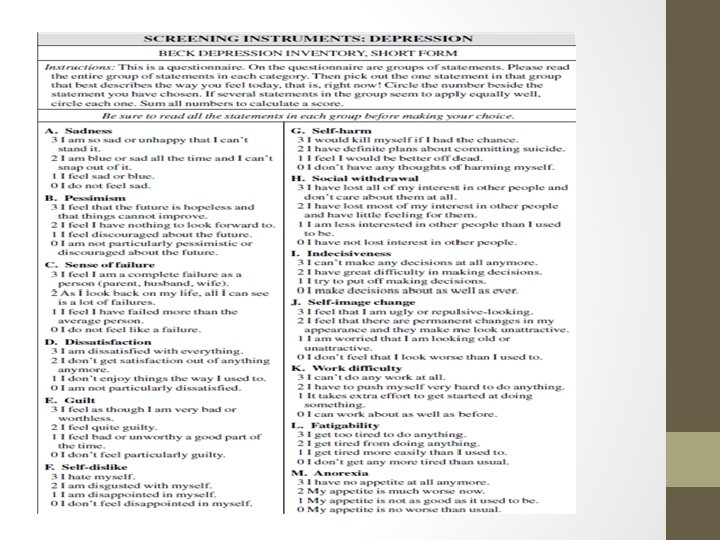
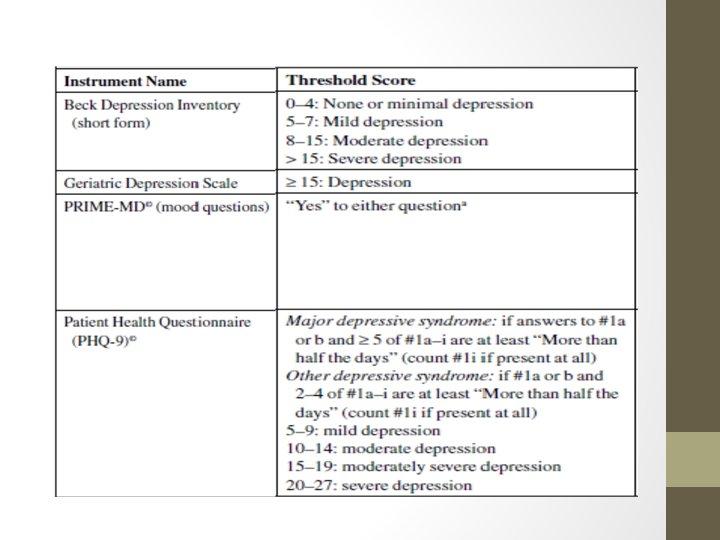
Depression 1) Children aged 7– 11 years Insufficient evidence to recommend for or against routine screening. 2) Adolescents: Screen all adolescents aged 12– 18 years for major depressive disorder (MDD) Screen in primary care clinics with the Patient Health Questionnaire (PHQ) (73% sensitivity; 94% specificity) or the Beck Depression Inventory-Primary Care (BDI-PC) (91% sensitivity; 91% specificity).
3) Adults: Recommend screening adults for depression -Asking two simple mood questions(Prime-MD)may be as accurate as formal screening tools: a. “Over the past 2 weeks, have you felt down, depressed, or hopeless? ” b. “Over the past 2 weeks, have you felt little or no interest or pleasure in doing things? ”
Tobacco Use -Recommends screening all adults for tobacco use and provide tobacco cessation interventions for those who use tobacco products. -Recommends screening all pregnant women for tobacco use and provide pregnancy-directed counseling and literature for those who smoke. -The “ 5 -A” framework is helpful for smoking cessation counseling.
The Five “A” Components of Behavior Counseling Interventions 1) Assess: Ask about or assess behavioral health risks and factors affecting choice of behavior change goals or methods. 2) Advise: Give clear, specific, and personalized behavior change advice, including information about personal health harms and benefits. 3) Agree: Collaboratively select appropriate treatment goals and methods based on the patient’s interest in and willingness to change the behavior. 4) Assist: Using behavior change techniques, aid the patient in achieving agreed-on goals by acquiring the skills, confidence, and social or environmental supports for behavior change, supplemented with adjunctive medical treatments when appropriate (e. g. , pharmacotherapy for tobacco dependence, contraceptive drugs or devices). 5) Arrange: Schedule follow-up contacts (in person or by telephone) to provide ongoing assistance or support and to adjust the treatment plan as needed, including referral to more intensive or specialized treatment. Intervention to help patients change unhealthy behaviors often requires repetition over time.
Thank you