Thermal Injuries Presented By Dr Hamideh feiz Assisstant

Thermal Injuries Presented By: Dr Hamideh feiz Assisstant proffessor of emergency medicine

Epidemiology Burn injuries are among the most devastating of all injuries and a major global public health crisis. Burns are the fourth most common type of trauma worldwide, following traffic accidents, falls, and interpersonal violence. Approximately 90 percent of burns occur in low- to middle-income countries, regions that generally lack the necessary infrastructure to reduce the incidence and severity of burns.

Epidemiology The American Burn Association estimates that 500, 000 individuals are treated for burns in the U. S. annually. Of these, 40, 000 require hospitalization. The vast majority of burn patients are treated in the acute setting by emergency physicians and discharged with outpatient follow-up.

Epidemiology… -The risk of burns is highest in the 18 - to 35 -year-old age group. -There is a male-female ratio of 2: 1 for both injury and death. - The incidence of scalds from hot liquids is higher in children 1 to 5 years of age and in the elderly. -The death rate in patients >65 years of age is much higher than that in the overall burn population

Pathophysiology

Skin functions as: -semipermeable barrier to evaporative water loss. -protection from the adversities of the environment -control of body temperature, sensation, and excretion

Physiologic Effects of Thermal Injury o Disruption of sodium pump o Intracellular influx of sodium and water o Extracellular efflux of potassium o Depression of myocardial contractility (>60% of body surface area burned) o Increased systemic vascular resistance o Metabolic acidosis o Increase in hematocrit and increased blood viscosity o Secondary anemia from erythrocyte extravasation and destruction Local tissue injury o Release of histamines, kinins, serotonins, arachidonic acids, and free oxygen radicals

Prognosis: Although many factors may influence prognosis, -the severity of the burn, -the presence of inhalation injury, -associated injuries, -the patient's age, -preexisting disease, -and acute organ system failure are most important.

The burn wound is described as having 3 zones: 1 -the zone of coagulation, in which tissue is irreversibly destroyed with thrombosis of blood vessels 2 -the zone of stasis, in which there is stagnation of the microcirculation 3 -the zone of hyperemia, in which there is increased blood flow

BURN SIZE 1 -rule of nines :

BURN SIZE 2 -the area of the back of a patient's hand is approximately 1% of the BSA. The number of “hands” that equal the area of the burn can approximate the percentage of body surface area burned.

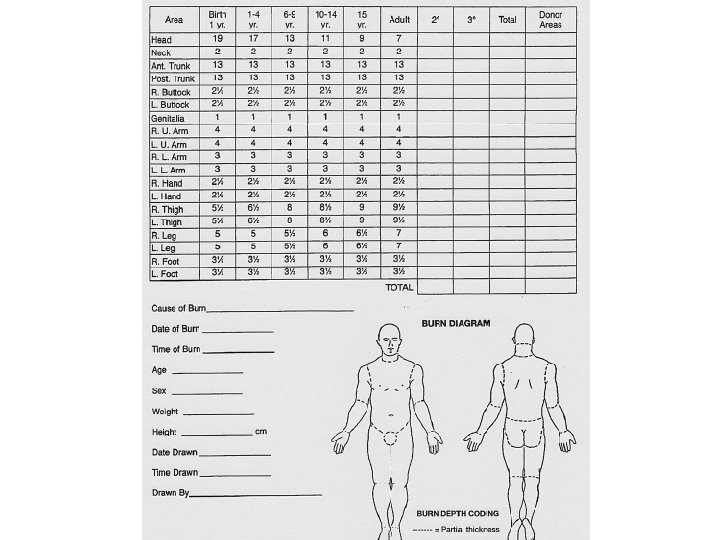
BURN SIZE 3 -Lund and Browder burn diagram: A more precise estimation

first-degree burn -only the epidermal layer of skin. -Sunburn is usually given as a common example -The burned skin is red, painful, and tender without blister formation. -usually heal in about 7 days without scarring -require only symptomatic treatment

 are")
Second-degree burns 1 -superficial partial-thickness: -the epidermis and the superficial dermis (papillary layer) are injured. (The deeper layers of the dermis, hair follicles, & sweat and sebaceous glands are spared. ) -often caused by hot water. -blistering of the skin -the exposed dermis is red and moist at the blister's base. -very painful to touch. -good perfusion of the dermis with intact capillary refill. -heal in 14 to 21 days, scarring is usually minimal, and there is full return of function

. -damage to")
Second-degree burns 2 -deep partial-thickness -extend into the deep dermis (reticular layer). -damage to hair follicles as well as sweat and sebaceous glands -their deeper portions usually survive. -Hot liquids, steam, grease, or flame -The skin may be blistered, and the exposed dermis is pale white to yellow in color. -The burned area does not blanch; it has absent capillary refill and absent pain sensation -Healing takes 3 weeks to 2 months. -Scarring is common -Surgical debridement and skin grafting may be necessary


Third-degree or full-thickness burns -All epidermal and dermal structures are destroyed. -usually caused by flame, hot oil, steam, or contact with hot objects. -The skin is charred, pale, painless, and leathery. -not heal spontaneously, because all dermal elements are destroyed. -Surgical repair and skin grafting are necessary -there will be significant scarring.



Fourth-degree burns -extend through the skin to the subcutaneous fat, muscle, and even bone. -devastating, life-threatening injuries. -Amputation or extensive reconstruction is sometimes required.


Inhalation Injury -As treatment of burn shock and sepsis has improved, inhalation injury has emerged as the main cause of mortality in burn patients. -Toxic inhalants are divided into three large groups: tissue asphyxiants, pulmonary irritants, and systemic toxins. -The two major tissue asphyxiants are carbon monoxide & hydrogen cyanide

Inhalation Injury -damaging endothelial cells, produces mucosal edema of the small airways, and decreases alveolar surfactant activity, resulting in bronchospasm, airflow obstruction, and atelectasis. -Although lower airway edema may not be clinically evident for up to 24 hours, upper airway edema can occur rapidly. -Approximately half of intubated burn patients admitted to burn centers develop acute respiratory distress syndrome. -Therefore, when inhalation injury is present, careful fluid resuscitation guided by hemodynamic monitoring can help avoid pulmonary edema and ARDS.

Inhalation Injury -The initial diagnosis of smoke inhalation: ü history of exposure to a fire in an enclosed space and ü physical signs that include facial burns, singed nasal hair, soot in the mouth or nose, hoarseness, carbonaceous sputum, and expiratory wheezing

Inhalation Injury Treatment of suspected inhalation injury : should be instituted prior to definitive diagnosis. -Humidified oxygen (100%) -ABG, including carboxyhemoglobin levels -Control of the upper airway by prompt endotracheal intubation.
 (2) (3) (4) (5) (6) full-thickness burns")
Inhalation Injury Indications for intubation include: (1) (2) (3) (4) (5) (6) full-thickness burns of the face or perioral region circumferential neck burns acute respiratory distress progressive hoarseness or air hunger respiratory depression or altered mental status supraglottic edema and inflammation on bronchoscopy

Chemical Burns

INTRODUCTION AND EPIDEMIOLOGY More than 25, 000 products are capable of producing chemical burns. Exposures occur both occupationally and in homes. As many as 10% of all burn center admissions are the result of chemical burns. Although a smaller percentage of total burns, the mortality is high and may account for as many as 30% of all burn deaths.

PATHOPHYSIOLOGY Although the outer stratum corneum layer of the skin functions as an excellent barrier against many chemicals, some penetrate it readily. Chemicals can produce burns, dermatitis, allergic reaction, thermal injury, and/or systemic toxicity. Most chemicals produce tissue damage by their chemical reaction rather than by thermal injury. Certainly, some chemicals produce significant heat by means of an exothermic reaction. However, most skin damage is the result of the chemical’s unique characteristics

PATHOPHYSIOLOGY Factors Influencing Tissue Damage: v Concentration of agent v Quantity of agent v Duration of contact v Mechanism of action v Extent of penetration

PATHOPHYSIOLOGY Most chemical burns are caused by acids or alkalis. At similar volumes and manner of contact, alkalis usually produce far more tissue damage than acids. Acids tend to cause coagulation necrosis with protein precipitation and form a tough leathery eschar. The eschar typically limits deeper penetration of the agent. Alkalis produce liquefaction necrosis and saponification of lipids. The result is a poor barrier to chemical penetration and deeper, ongoing burns. Other chemical injuries occur by various pathophysiologic mechanisms. Some chemical agents cause injury by more than one mechanism.

PATHOPHYSIOLOGY Death early after severe chemical burns is usually related to hypotension, acute renal failure, and shock as a result of fluid loss. However, systemic toxicity and subsequent morbidity and mortality may also occur if chemicals are absorbed. Acidosis, hypotension, hyperkalemia, dysrhythmia, and shock can occur with systemic absorption of acids.

Systemic Effects Associated with Chemical Burns Ø Hydrofluoric acid: Hypocalcemia, hypomagnesemia, hyperkalemia, cardiac arrhythmias, sudden death Ø Tannic acid, chromic acid, formic acid, picric acid, phosphorus: Hepatic necrosis, nephrotoxicity Ø Gasoline: Severe pulmonary, cardiovascular, neurologic, renal, and hepatic complications Ø Sodium nitrate, potassium nitrate: Severe methemoglobinemia with refractory cyanosis
- Slides: 36