The Viridans streptococci Streptococcus pneumoniae pneumococcus Streptococcus pneumoniae

")



, Beta-galactosidase A (Bga. A), Beta-N-acetylglucosaminidase (Str. H), and Neuraminidase")


 Deacetylate peptidoglycan molecules on")





. Mastoid (mastoiditis). Paranasal sinuses (sinusitis).")
.")




 reaction - Glass slide. - sputum/suspension. - type specific or polyvalent")


 Gram positive Lancet shaped cocci in pairs b) Capsule demonstration")



 • Proteins are coupled to")
 v A heterogeneous group of streptococci which cannot be")
; • S. mutans, • S. oralis,")





- Slides: 37
The Viridans streptococci
Streptococcus pneumoniae (pneumococcus)
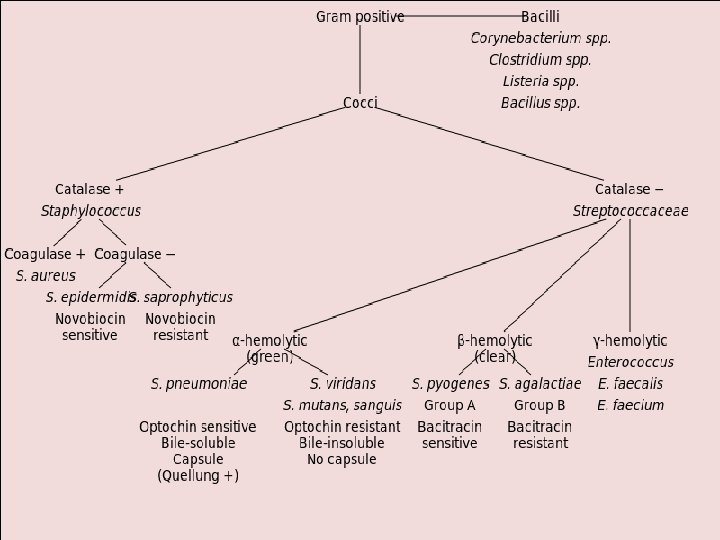
Streptococcus pneumoniae Classic example of a highly invasive extracellular bacterial pathogen. Capsulated. Gram positive. Lanceolate shaped diplococci.
It is a major cause of morbidity and mortality globally causing more deaths than any other infectious disease. Commonly a quiescent colonizer of the upper respiratory tract where up to 60% of small children may carry pneumococci in the nose asymptomatically. Diseases range from mild respiratory tract mucosal infections to more severe diseases.
Bacterial virulence factors CAPSULE Repulses the sialic acid residues of mucus by its negative charge decreasing the likelihood of entrapment. During colonization, the thick capsule prevents Mucus entrapment as well as immunoglobulin and complement binding thereby preventing opsonophagocytosis. PNEUMOLYSIN (Ply) Pore-forming toxin, decreases epithelial cell ciliary beating thereby enabling the pneumococcus to bind to epithelial cells without being removed with the mucus. SALIVARY Ig. A / Ig. A 1 protease Limit Opsonization by: First, the capsule itself prevents binding of s. Ig. A. Second, capsule-bound Ig. A is cleaved by a pneumococcal Ig. A 1 protease.
EXOGLYCOSIDASES Neuraminidase A (Nan. A), Beta-galactosidase A (Bga. A), Beta-N-acetylglucosaminidase (Str. H), and Neuraminidase B (Nan. B): deglycosylate mucus glycoconjugates decreasing mucus viscosity preventing mucus entrapment. Enzymes Peptidoglycan N-acetylglucosamine-deacetylase A (Pdg. A) and an O-acetyltransferase (Adr), deacetylate peptidoglycan molecules on the pneumococcal surface, rendering the bacterium resistant to lysozyme PNEUMOCOCCAL SURFACE PROTEIN A (Psp. A), Binds human apolactoferrin at its active site, thereby inhibiting apolactoferrin mediated bacterial killing
Sequence of events Natural barriers preventing pneumococci from binding to the respiratory mucosal Colonization of the upper respiratory tract surface are the respiratory mucus and lysozyme predisposition Spread of infection to the lower respiratory tract Infection of the middle ear, Neuraminidase cleaves mucin paranasal sinuses Multiply in lungs Infection of meninges by contiguity / blood Enters blood causing bacteremia, Toxin pneumolysin and H 2 O 2 released in copious amounts disrupt the alveolar epithelium Outpouring of edema fluid, WBC, RBC into the alveoli Disseminated infections as in the heart, peritoneum or joint Consolidation
Later Mononuclear cells actively phagocytose the bacteria and cell debris and digest them intracellularly Development of type specific Abs. Recovery begins between 5 – 10 days. Clinical Symptoms / Complications
Exoglycosidase Mucus Degradation Decreases epithelial cell ciliary beating Pneumolysin (Ply) Deacetylate peptidoglycan molecules on the pneumococcal surface, rendering the bacterium resistant to lysozyme
Pathogenesis -> 1. Source of infection: ü Exogenous – Patients / carriers -> shed organisms in their respiratory secretions. (40 – 70% of a population harbor pneumococci at some time during their lifetime). ü Endogenous – Part of the normal flora of URT. 2. Mode of infection – Inhalation of droplet nuclei or by direct / indirect contact.
3. Host predisposing factors Infection & carriage is common but disease occurs only under certain predisposing conditions. A. Abnormalities of the Respiratory tract a) Viral infections damaging surface cells. b) Abnormal accumulation of mucus – allergy. c) Bronchial obstruction – atelectasis. d) Respiratory tract injury due to irritants disturbing its muco-ciliary function.
B. Alcohol / Drug intoxication results in, i. Decreased phagocytic activity. ii. Decreased cough reflex. iii. Facilitates aspiration. C. Abnormal circulatory dynamics i. Pulmonary congestion. ii. Heart failure.
D. Other factors i. Malnutrition. ii. General debility. iii. Old age. iv. Sickle cell anemia. v. Hyposplenism. vi. Complement deficiency. vii. Convulsions.
Clinical findings & complications Ø Lobar Pneumonia - Sudden onset of fever, chills & sharp pleural pain, with expectoration of bloody or rusty colored sputum. Ø Mortality rate in pneumonia is high (30%) if cases are untreated.
Ø Contiguous spread may result Middle ear infection (otitis). Mastoid (mastoiditis). Paranasal sinuses (sinusitis). Pus in pleural space (empyema) may require aspiration / drainage.
Ø bacteremia In 10 – 20% of patients occurs with metastatic involvement. Meninges (meningitis). joints (septic arthritis). Rarely, the endocardium (acute endocarditis). Ø Long-term sequelae After pneumococcal meningitis, including sensomotor deficit, hearing loss, and cognitive impairment, which may occur in up to 30% of surviving patients
Progression of pneumococcal disease. Otitis media sinusitis mastoiditis empyema Bacteremia Aerosol Pneumonia Colonization Asymptomatic colonization Endocarditis Septic arthritis Meningitis
Lab diagnosis 1. Specimen -> ü Sputum, ü Blood, ü CSF, ü Pus from suppurative lesions, ü Synovial fluid, ü Laryngeal swab (in the place of sputum in children)
2. Microscopy -> Gram’s stained smear : Pneumococci are seen as Gram positive lancet or flame shaped cocci in pairs along with pus cells
Capsule demonstration: - i. By negative staining – India Ink or Nigrosin – capsule may be demonstrated as clear halo. ii. Quellung reaction (Capsule swelling reaction)
Quellung (capsular swelling) reaction - Glass slide. - sputum/suspension. - type specific or polyvalent antisera (Abs). . Ag-Ab reaction and a change in the refractive index of the capsular material. . Observed under light microscope . Apparent swelling of capsules around the pneumococci.
Culture Ø Media used - Blood agar , Chocolate agar Ø Specimens are inoculated onto media and incubated at 37 o C under 5 -10% CO 2 Ø Colony characteristics -> - Alpha hemolytic colonies - Dome shaped initially which on further incubation acquires - Draughtsman’ appearance - This is due to the production of autolysins by the streptococci which cause lysis of the older cells in the centre
Draughtsman’ colonies on blood agar
Identification of isolate a) Gram positive Lancet shaped cocci in pairs b) Capsule demonstration c) Alpha hemolytic colonies d) Bile solubility test –> positive e) Optochin sensitivity test –> sensitive f) Animal pathogenicity test –> Virulent to mouse
Serology • Rapid diagnostic method -> Ø Detection of capsular polysaccharide Ag in blood, CSF By ü Latex agglutination , ü Co-agglutination ü ELISA Antibiotic susceptibility testing Ø Should be done to determine susceptibility pattern
Treatment • Penicillin – drug of choice. • Tetracycline/ Erythromycin – also effective. • Penicillin resistant strains – 3 rd generation Cephalosporin are used.
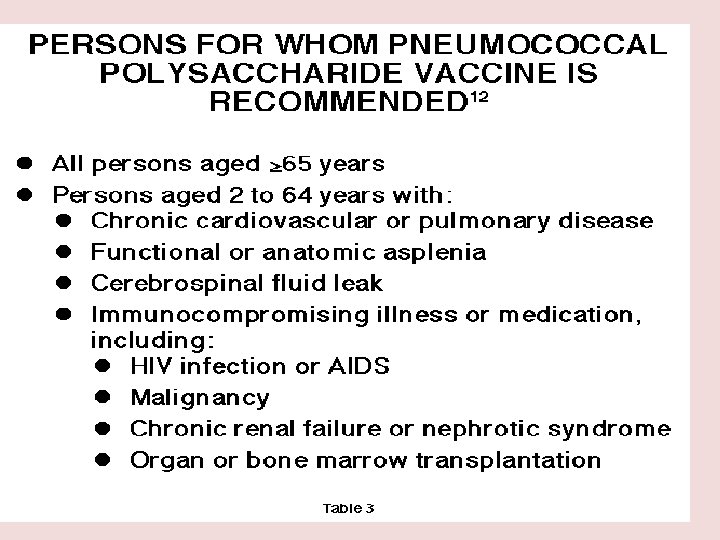
Prevention • Immunity against Pneumococci is type specific. • A polyvalent polysaccharide vaccine containing 23 serotypes is available and administered by single dose injection. • This vaccine is not for general use.
• Newer vaccines are now used (conjugate vaccines) • Proteins are coupled to the polysaccharides to get a more Tcell-dependent immune response. For technical reasons and because of high costs, only a limited number of polysaccharides have been included so far in the conjugate vaccines (7, 10, and recently 13 serotypes).
The Viridans Streptococci Viridis (green) v A heterogeneous group of streptococci which cannot be grouped under Lancefield's classification. v Part of the normal flora of the oral cavity and upper respiratory tract. v Mostly alpha hemolytic (greenish color ‘viridans’). v Insoluble in bile v Resistant to ‘Optochin’
Species: It Has six species groups (viridans group); • S. mutans, • S. oralis, • S. salivarus • S. sanguis • S. milleri • S. mitis
Human pathogenicity 1. Dental caries Str. mutans produces large amounts of slime. Adheres to teeth to form ‘plaques’. Bacteria within plaques ferment dietary starch into acids. Damage dentine resulting in caries.
2. Sub-acute bacterial endocarditis After dental extraction/manipulations. Bacteria enter blood stream. Settle on damaged heart valves. Form vegetation and cause sub-acute endocarditis.
Differences between Str. pneumoniae & Viridans Streptococci Property Pneumococci Viridans Streptococci Morphology Lanceolate, diplococci Spherical / oval cocci In long chains Capsule Present Absent / Slime Colony Draughtsman Dome Bile solubility Soluble Insoluble Optochin sensitivity Sensitive Resistant Animal pathogenicity Virulent (mouse) Avirulent
Characteristic features of different groups of streptococci Lance. group Species Common name Diagnostic tests Disease A Str. pyogens Bacitracin : S, PYR: +, Ribose not URT infection, skin infection , ARF, AGN fermented, SXT: R B Str. agalactiae CAMP: +, Hippurate hydrolysis+ SXT: R Neonatal septicaemia , meningitis C or G Str. dysgalactiae Ribose & Trehalose : Fermented Pharyngitis , endocarditis D Enterococcus spp. BEA: +, Heat test : +, grows in 6. 5% UTI , Wound infections nacl, PYR: +, SXT: R Not Typed Non enterococcus species BEA: +, 6. 5% nacl: no growth, PYR: Genitiurinari infections - ve, SXT: s Viridians str. Optochin : R , species different. on biochemical tests Endocarditis , Dental carries
THANK YOU