The use of contrast media which injected intravenously








 A high spatial")

 SL 1 mm same position standard resolution (smooth)")


 from lung apices to liver n")
 Cor. 5 mm/5 mm")

 from lung apices to diaphragm")
 from chin to kidney Cor. 5 mm/5")

 from lung apices to IC Bolus")




- Slides: 54
The use of contrast media which injected intravenously is important for visualization of structures within the mediastinum. Ø Ø Department protocols/radiologist preferences determine the specific type, volume and site of injection. ( Average dose 80 ml) For children 1. 5 ml per kilogram body weight.
1. To detect lesions 2. To distinguish vessels from lesions 3. To demonstrate displacement of vessels by masses 4. To demonstrate the enhancement of pathologies
切面厚度Slice thickness 切面間距Slice spacing 視野Field of view 重組函數Reconstruction algorithm 影像呈現設定Imaging display settings
Single attenuation value of voxel represents average of all attenuation of all various structures within it Thicker the slice greater the averaging called partial volume effect Partial volume effect reduced by thinner section Determined by size of structure being assessed and number of scans required to evaluate the patient
Reconstruction algorithm Lung parenchyma : high spatial algorithm High spatial algorithm reduces smoothing Better depiction of normal and abnormal parenchymal interface Mediastinum and chest wall standard soft tissue algorithm
Slice spacing Adequate assessment of patient 10 mm interval 1 to 2 mm slice with 10 mm interval allows only 10 to 20% of lung Improved spatial resolution allows better assessment of normal and abnormal findings Pulmonary metastasis requires 5 to 7 mm thick sections Trachea and central bronchi 3 to 5 mm thick sections Pulmonary parenchyma and peripheral bronchi requires 1 to 2 mm sections
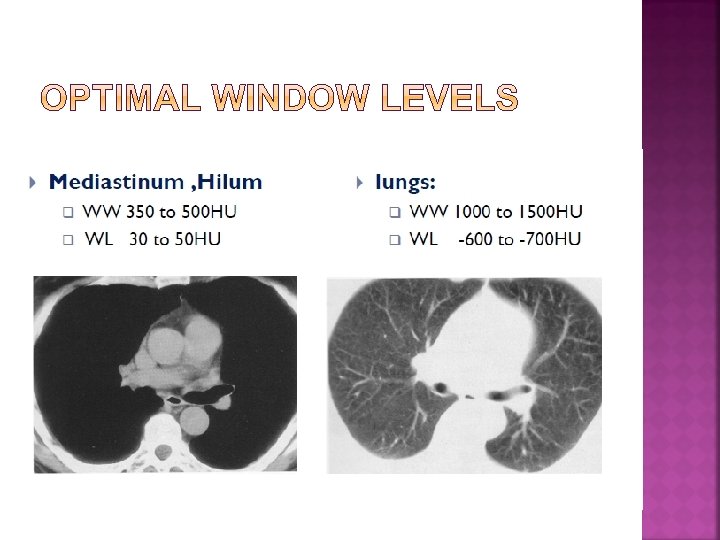
Image display settings Two parameters: window width and window level Average density of each voxel : Hounsfield unit These units are arbitrary so 0 is for water, 1000 for air Range of Hounsfield in thorax is wider ranging from -850 HU for aerated lung to 700 HU for ribs Display of images determined by window level and window width
Solitary pulmonary nodule Evaluation of diffusely CXR -Cystic fibrosis, Sarcoidosis, Interstitial lung disease, Histocytosis X, ARDS
A narrow slice width is used (usually 1– 2 mm) A high spatial resolution image reconstruction algorithm is used Field of view is minimized, so as to minimize the size of each pixel Prone scanning
5 mm 1 mm same Reconstruction in High resolution algorithm same scan data
high resolution (sharp) SL 1 mm same position standard resolution (smooth)
A Scan FOV 40 cm B Target FOV 25 cm
Indications : General screening of Pathology Patient Position : Supine arms elevated above head Topogram: from chin to below liver Breathing Breath hold in inspiration ( single breath hold) Contrast I. V : 80 ml
C-: 5 mm/5 mm (Soft tissue widow ) from lung apices to liver n C+: 5 mm/5 mm(Soft tissue widow ) from chin to kidney n
Lung window 5 mm/5 mm (lung apices to below diaphragm) Cor. 5 mm/5 mm
Patient Position : Supine arms elevated above head Topogram : From lung apices to liver Breathing : Breath hold in inspiration ( single breath hold) Contrast I. V : 80 ml
C-: n Inspiration: 1 mm/5 mm (lung window ) from lung apices to diaphragm n Expiration: 1 mm/5 mm (lung window) from lung apices to diaphragm 5 mm/5 mm (soft window) From lung apices to liver
C+: 5 mm/5 mm (Soft tissue widow) from chin to kidney Cor. 5 mm/5 mm Lung window 5 mm/5 mm
Patient Position : Supine arms elevated above head Topogram : From chin to aortic bifurcation Breathing : Breath hold in inspiration ( single breath hold) Contrast I. V : 80 ml (2. 5 mm/s)
C-: 5 mm/5 mm (Soft tissue widow ) from lung apices to IC Bolus tracking ROI setting at aortic arch C+: 5 mm/5 mm(Soft tissue widow ) from chin to IC
Lung window 5 mm/5 mm Sag. 3 mm/3 mm Cor. . 3 mm/3 mm
CTA-VRT