The Thorax and Abdomen Sports Medicine 2 Mr

The Thorax and Abdomen Sports Medicine 2 Mr. Smith

Assessment of the Thorax and Abdomen Ü As a preface: Ü Injuries to this region can produce life-threatening situations Ü Because of all the vital organs in this area Ü Athletic trainer’s evaluation should focus on signs and symptoms that indicate potentially life-threatening conditions Ü Will not be able to accurately dx all injuries to these regions…. will need an MRI or CT scan usually Ü Continually monitor breathing, circulation and any indication of internal bleeding or shock Ü Refer if necessary! Call 911 if deemed life threatening
 Ü What happened to cause this injury?")
SOAP Note Ü Subjective (Stands for…? ) Ü What happened to cause this injury? Ü Was there direct contact or a direct blow? Ü What position were you in? Ü What type of pain, was it immediate or gradual, location(s)? Ü Difficulty breathing? Ü What positions are most comfortable? Ü Do you feel faint, light-headed or nauseous? Ü Chest pain?

SOAP Note cont. Ü Subjective cont. Ü Hear or feel snap, crack or pop in your chest? Ü Muscle spasms? Ü Blood or pain during urination? Ü Usually don’t know this right away, but tell them to monitor this… Ü How long has it been since you last ate? Ü Is there a personal or family history of any heart, abdominal problems or other diseases involving the abdomen and thorax?
 Ü Is the patient breathing? Are")
SOAP Note cont. Ü Objective (stands for? ) Ü Is the patient breathing? Are they having difficulty Ü Ü Ü breathing? Does breathing cause pain? Is the patient holding their chest wall? Is there symmetry of the chest during breathing? If the patient’s wind was knocked out, is normal breathing returning? How rapidly? Approaching them on the field… note the body positioning Typical Body Positioning… Ü Thorax injury - leaning towards side that is injured and splinting area w/ hand Ü Abdominal injury - lie on side w/ knees pulled to chest Ü Male external genitalia injury - lying on side holding scrotum

SOAP Note cont. Ü Check for areas of discoloration, swelling or deformities Ü Around umbilicus = intra-abdominal bleed Ü Flanks = swelling outside the abdomen Ü Does the thorax appear to be symmetrical? Ü Are the abdominal muscles tight and guarding? Ü Is the athlete holding or splinting a particular part? Ü If they are vomiting blood Ü Bright red = lung injury Ü Bright red and frothy = injury to esophagus and stomach Ü Coffee grounds- dried blood, very serious!

SOAP Note cont. Ü Cyanosis – respiratory difficulty Ü Monitor vital signs (pulse, respiration, BP) Ü Rapid weak pulse or drop in BP is an indication of a serious internal injury (involves blood loss) Ü Pale, cool, clammy skin indicates low BP
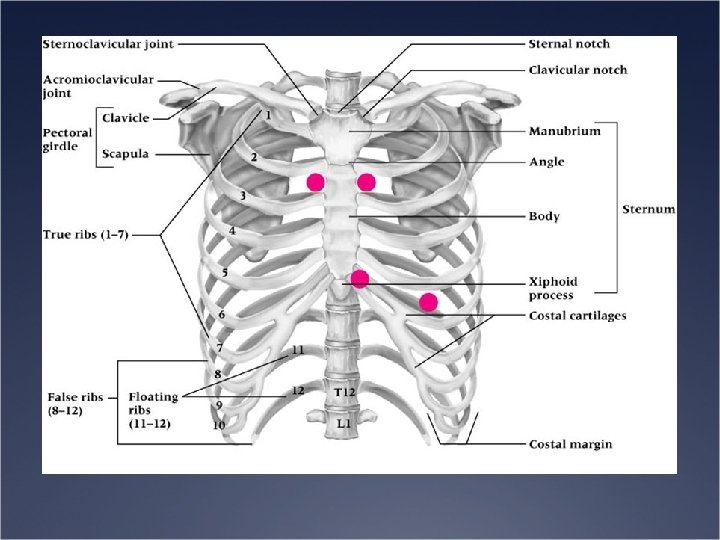

SOAP Note cont. Ü Objective cont. Ü Palpation and Special Tests Ü Thorax Ü Check for symmetry of chest wall movement and search for areas of tenderness Ü Palpate along ribs and intercostal spaces as well as costochondral junctions Ü A/P pressure to rib cage to assess for fracture Ü Transverse pressure assesses costochondral junction Ü Semi-reclining position is useful if athlete is having difficulty breathing
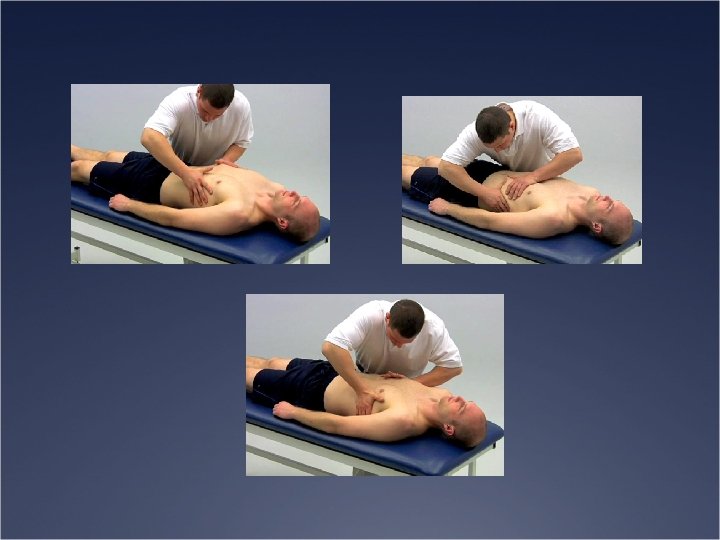

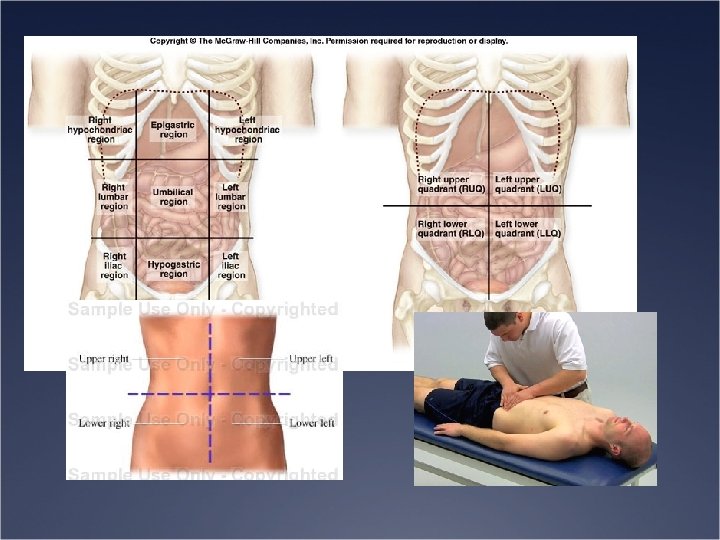
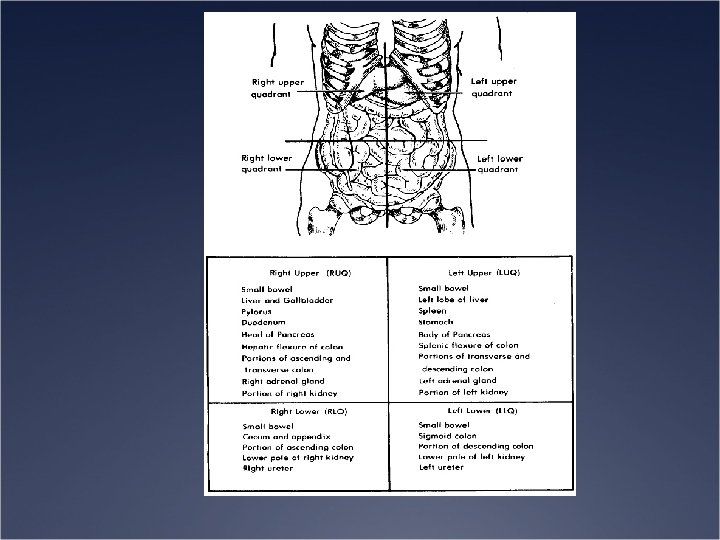
SOAP Note cont. Ü Objective cont. Ü Palpation and Special Tests Ü Abdomen Ü Patient should have arms at side, knees and hips flexed to relax abdomen Ü Four abdominopelvic quadrants (move clockwise starting from upper right quadrant) Ü Feel for guarding and tenderness, rigidity (internal bleeding) Ü Rebound tenderness Ü Assess each organ (if possible)

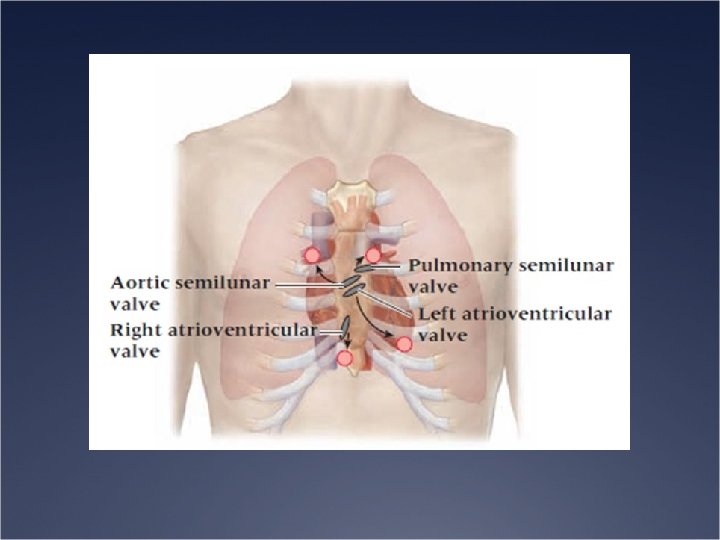
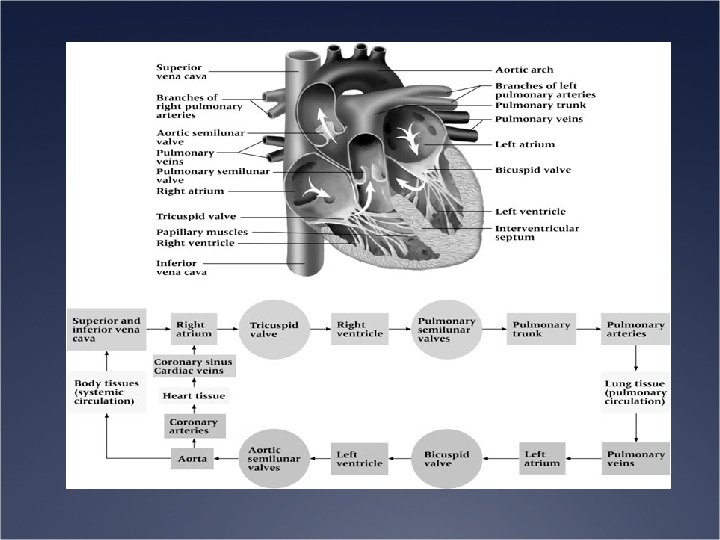
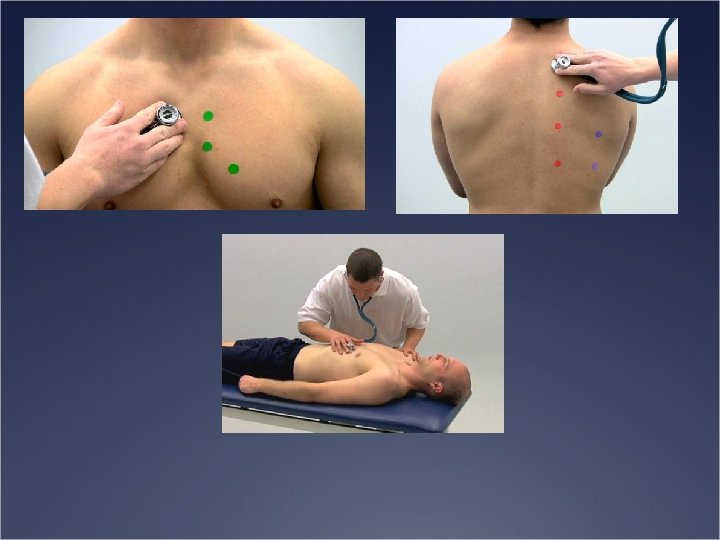
SOAP Note cont. Ü Auscultation Ü Heart Sounds Ü “Lubbdupp” (may hear 3 rd sound in children) Ü Listen for murmur (abnormal period due to valve insufficiency) Ü Listening at a variety of points

Ü Breath sounds Ü Should be consistent Ü Abnormal patterns Ü Want the person to be breathing in and out at a normal rate Ü Listening for: Ü Wheezing Ü Crackles Ü Rattling Ü Noisy breathing Ü Perform over apex, centrally and at base of each lung, both anteriorly and posteriorly

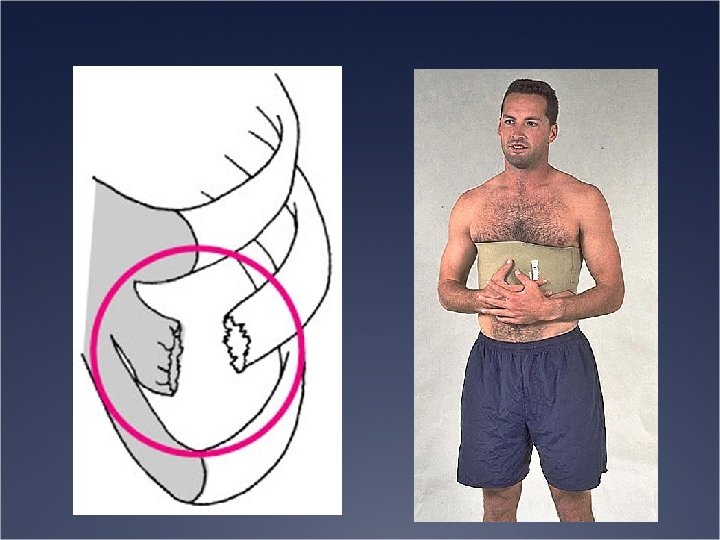
Recognition and Management of Specific Injuries Ü Rib Contusion Ü Etiology Ü Blow to the rib cage can bruise ribs, musculature or result in fracture Ü Signs and Symptoms Ü Painful breathing (particularly if muscles are involved) Ü Point tenderness; pain with rib compression Ü Management Ü RICE and NSAID’s Ü Rest and decrease in activity

Ü Rib Fractures Ü Etiology Ü Caused by a direct blow or the result of a violent muscular contraction Ü Can be caused by violent coughing and sneezing Ü A flail chest is one where 3+ consecutive ribs are fractured Ü Signs and Symptoms Ü History is critically important Ü Pain with inspiration, point tenderness and possible deformity with palpation Ü Management Ü Refer for X-rays Ü Support and rest; brace

Ü Costochondral Separation Ü Etiology Ü Result of a direct blow to the anterolateral aspect of the rib cage Ü Signs and Symptoms Ü Localized pain in region of costochondral junctions Ü Pain with movement; difficulty with breathing Ü Point tenderness and possible deformity Ü Management Ü Rest and immobilization Ü Healing may take 1 -2 months

Ü Sternum Fractures Ü Etiology Ü Result of high impact blow to the chest Ü May also cause contusion to underlying cardiac muscle Ü Signs and Symptoms Ü Point tenderness over the sternum Ü Pain with deep inspiration and forceful expiration Ü Signs of shock, or weak rapid pulse may indicate more severe injuries Ü Management Ü X-ray and monitor patient for signs of trauma to the heart

Ü Muscle Injuries Ü Etiology Ü Muscles are subject to contusions and strains Ü Occur most often from direct blows or sudden torsion of the trunk Ü Signs and Symptoms Ü Pain occurs on active motions; pain with inspiration and expiration, coughing, sneezing and laughing Ü Management Ü Immediate pressure and application of cold for approximately one hour if over the clothing or over brace! Ü After hemorrhaging is controlled, immobilize the injury to make the patient comfortable

Ü Lung Injuries Ü Etiology Ü Pneumothorax Ü pleural cavity becomes filled with air, negatively pressurizing the cavity, causing a lung to collapse Ü Will produce pain, difficulty with breathing and anoxia Ü Tension Pneumothorax Ü Pleural sac on one side fills with air displacing lung and heart, compressing the opposite lung Ü May cause shortness of breath, chest pain, absence of breath sounds, cyanosis, distention of neck veins, deviated trachea Ü Hemothorax Ü Blood in pleural cavity causes tearing or puncturing of the lungs or pleural tissue Ü Painful breathing, dyspnea, coughing up frothy blood and signs of shock

Ü Traumatic Asphyxia Ü Result of a violent blow or compression of rib cage Ü Causes cessation of breathing Ü Signs include purple discoloration of the trunk and head, conjunctivas of the eye Ü Condition requires immediate mouth to mouth resuscitation Ü 911 immediately!!! Ü Management Ü Each of these conditions are medical emergencies and require immediate attention Ü Transport patient to hospital immediately

Ü Hyperventilation Ü Etiology Ü Rapid rate of ventilation due to anxiety induced stress or asthma Ü Develop a decreased amount of carbon dioxide relative to oxygen Ü Signs and Symptoms Ü Patient has difficulty getting air in and seems to struggle with breathing Ü Panic state with gasping and wheezing Ü Management Ü Ü Decrease rate of carbon dioxide loss Slow respiration rate and alter respiration techniques Breath into a bag Normal respiration should return within 1 -2 minutes, initial cause must be determined

Ü Sudden Cardiac Death Syndrome in Athletes Ü Etiology Ü Hypertrophic cardiomyopathy- thickening of cardiac muscle w/ a decrease in chamber size Ü Increased chance for heart arrhythmia Ü Anomalous origin of coronary arteries Ü One of the arteries is located in a different site than normal Ü Marfan’s syndrome- abnormality in connective tissue results in weakening of aorta and cardiac vessels Ü Series of additional cardiac causes Ü Coronary artery & peripheral artery disease Ü Right ventricular dysplasia; cardiac conduction abnormalities; aortic stenosis Ü Wolf-Parkinson-White syndrome Ü Non-cardiac causes include drugs and alcohol, intracranial bleeding, obstructive respiratory disease Ü http: //www. nhlbi. nih. gov/health/dci/Diseases/arr_types. html

Ü Sudden Cardiac Death Syndrome in Athletes cont. . Ü Signs and Symptoms Ü Most do not exhibit any signs prior to death Ü May exhibit chest pain, heart palpitations, syncope, nausea, profuse sweating, shortness of breath, malaise and/or fever Ü Management/Prevention Ü Counseling and screening are critical in early identification and prevention of sudden death Ü Screening questions should address the following Ü History of heart murmurs Ü Chest pain during activity Ü Periods of fainting during exercise Ü Family history Ü Thickening of heart or history of Marfan’s syndrome Ü Cardiac screening - electrocardiograms and echocardiograms

Ü Heart Murmur Ü Etiology Ü Abnormal periodic sounds heard during auscultation Ü Functional murmur = no organic heart dysfunction Ü Forceful blood flow (high cardiac output) through healthy valves Ü Abnormal murmur = blood flow through damaged valve Ü Mitral valve prolapse – can lead to infective endocarditis or aortic regurgitation Ü Mitral valve or aortic stenosis – narrowing due to scarring from infections; if untreated could result in heart failure Ü Aortic sclerosis – scarring and thickening of aortic valve due to arthrosclerosis; tends not to be dangerous

Ü Heart Murmur cont. Ü Signs and Symptoms Ü Abnormal or unusual sounds (clicking, whooshing, swishing) Ü Abnormal murmurs could result in symptoms of other heart problems Ü Management Ü Different types require different management Ü Mitral valve prolapse and innocent murmurs don’t require additional management Ü Others will require medication to reduce chance of infection, prevent clots, control irregular beats, control heart beat/fluttering, relax dilated vessels Ü Surgery may be required to fix valve issues or repair congenital defects

Ü Athletic Heart Syndrome Ü Etiology Ü Structural and functional heart changes due to greater than one hour on most days Ü Results in increased left ventricle mass, diastolic capacity dimension, wall thickness Ü Maximum cardiac output increases = low resting heart rate & longer diastolic filling time Ü Systolic and diastolic function remain normal Ü Signs and Symptoms Ü Typically asymptomatic Ü May exhibit bradycardia, systolic murmur, extra heart sounds with ECG abnormalities being common Ü Management Ü If serious cardiac conditions are ruled out – no treatment necessary

Ü Commotio Cordis Ü Etiology Ü Syndrome resulting in cardiac arrest due to traumatic blunt impact to chest Ü Unfortunate timing relative to where the heart is at during its beat. Ü Young athletes are at risk Ü Signs and Symptoms Ü Ventricular fibrillation Ü Management Ü Resuscitation of victim is seldom successful Ü Early defibrillation with AED and resuscitation is critical

Ü Heart Contusion Ü Etiology Ü Result of compression between sternum and spine Ü Most severe consequence would involve an aortic rupture Ü Signs and Symptoms Ü Severe shock and heart pain Ü Heart may exhibit arrhythmias causing a decrease in cardiac output, followed by death if medical attention is not administered Ü Management Ü Immediate referral to an emergency room Ü Prepare to administer CPR and treat for shock

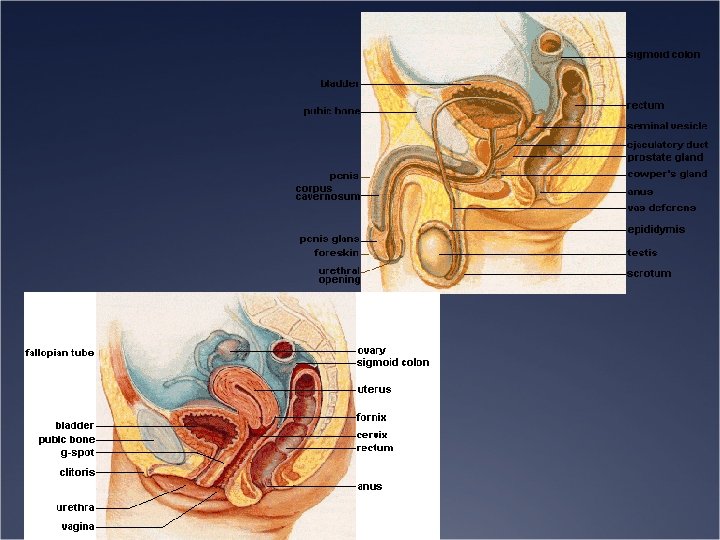
Injuries and Conditions of the Abdomen

Ü Kidney Contusion Ü Etiology Ü Result of an external force Ü Susceptible to injury Ü Signs and Symptoms Ü May display signs of shock, nausea, vomiting, rigidity of back muscles and hematuria (blood in urine) Ü Referred pain (costovertebral angle posteriorly radiating forward around the trunk)
 - refer if necessary Ü 24")
Ü Management Ü Monitor status of urine (hematuria) - refer if necessary Ü 24 hour hospitalization and observation with a gradual increase in fluid intake Ü Surgery may be required if hemorrhaging continues Ü 2 weeks of rest and close surveillance following initial return to activity is necessary

Ü Contusion of Ureters, Bladder and Urethra Ü Etiology Ü Blunt force to the lower abdomen may contuse/rupture bladder Ü Hematuria is often associated with contusion of bladder Ü Injury to the urethra (more common in males) may produce severe perineal pain and swelling Ü Signs and Symptoms Ü Pain, discomfort of lower abdominal region, abdominal rigidity, nausea, vomiting, shock, bleeding from the urethra, increased quantity of bloody urine, Ü Inability to urinate will present in case of ruptured bladder
 Ü Referred")
Ü Contusion of Ureters, Bladder and Urethra Ü Signs and Symptoms (continued) Ü Referred pain to low back and trunk as well as upper thigh region anteriorly and suprapubically Ü Prevention Ü Check periodically for blood in urine Ü Empty bladder prior to practice or competition Ü Wear protective equipment

Ü Abdominal Muscle Strain Ü Etiology Ü Result of sudden twisting or reaching of trunk, tearing abdominal musculature Ü Signs and Symptoms Ü Severe pain and hematoma formation Ü Generally involves rectus abdominis Ü Management Ü Ice and compression with conservative treatment Ü Exercise within pain free limits

Abdominal Muscle Strains Muscles Actions Rectus Abdominis Flexion of vertebral column External Oblique Assists flexion, Rotation to the other side Internal Oblique Assists flexion, Rotation to the same side Transverse Abdominis Compresses the abdominopelvic cavity Quadratus Lumborum Abduction of vertebral column

Abdominal Wall Anatomy Ü Posterior Wall Ü Quadratus Lumborum Ü Psoas Major Ü Iliacus

Quadratus Lumborum Ü Originates from rib 12 and transverse process of upper three lumbar vertebrae Ü Inserts medial surface, crest of the ilium and transverse process of L 5 Ü Action: Hip hike, lateral flexion of trunk

Psoas Major Ü Originates from T 12 to L 5 transverse processes, vertebral bodies, and intervertebral discs Ü Combines with iliacus to insert on lesser trochanter of femur Ü Flexor of the hip

Iliacus Ü Originates on inner surface of iliac fossa Ü Joins psoas major to insert on lesser trochanter of femor Ü Flexor of the hip

Abdominal Wall Anatomy Ü Anterior Wall and Lateral Wall Ü Rectus Abdominus Ü External Abdominus Oblique Ü Internal Abdominus Oblique Ü Transverse Abdominus

Rectus Abdominus Ü Originates on costal cartilages of 5 th-7 th ribs Ü Inserts on pubic crest Ü Tendons separate sections (gives off look of “ 6 pack”) Ü Flexes trunk and allows for upright posture

External Oblique Ü Originates on 5 th-7 th ribs Ü Interdigitates with serratus anterior Ü Upper fibers become external oblique aponeurosis Ü Lower fibers insert to iliac crest

Internal obliques Ü Originates from thoracolumbar fascia and iliac crest Ü Lower fibers insert to inguinal ligament Ü Upper fibers insert to lower 3 ribs

Transverse abdominus Ü Originates on costal margin between 6 th-12 th rib, crest of ilium, and inguinal ligament

Ü Contusions of Abdominal Wall Ü Etiology Ü Caused by a compressive force - generally occurring in collision sports Ü Extent of injury depends on whether force is blunt or penetrating Ü Signs and Symptoms Ü May cause a hematoma to develop under fascia of surrounding muscle tissue Ü Swelling may cause pain and tightness w/in the region Ü Management Ü Cold pack and compression Ü Be sure to check for signs of internal injuries

Core Rehab. Ü The oblique muscles of the core perform or assist the actions of… Ü Trunk rotational and diagonal movements Ü Side bending Ü Trunk flexion Ü Deep muscles assist in respiration

Core Rehab. Ü Rectus Abdominus Ü Most anterior part of the abdominal muscles Ü Largest muscle of the core Ü Action is trunk flexion Ü Protects organs from external forces

Core Rehab. Ü The middle and low back muscles perform or assist the actions of… Ü Trunk extension Ü Trunk rotation Ü Lateral side bending Ü Standing up
- Slides: 55