The stomach By Dr Muslim Kandel 2018 19

The stomach By Dr Muslim Kandel 2018 -19

Surgical Anatomy Stomach is “J” shaped flat bag Located in epigastric, left hypochondriac regions Food enters through gastroesophageal (cardiac) sphincter Food empties into the small intestine at the pyloric sphincter Regions of the stomach Cardiac region Fundus Body Pylorus – terminal end Lesser curvature & Greater curvature
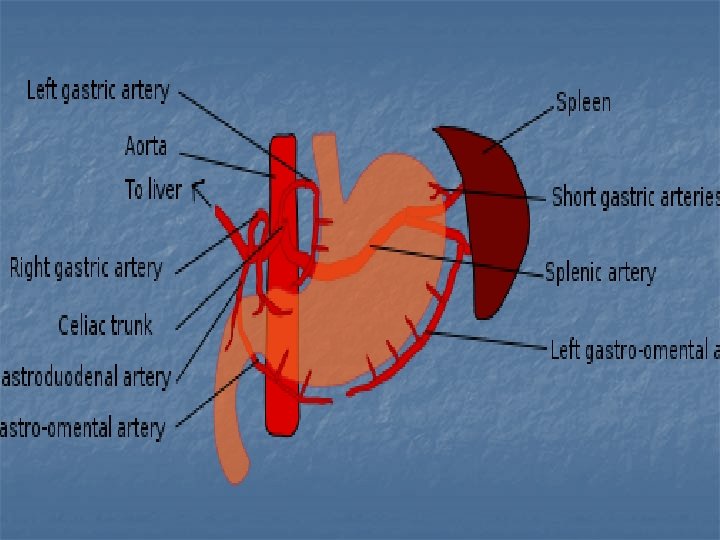

Veins In general the veins are equivalent to the arteries, those along the lesser curve ending in the portal vein and those on the greater curve joining via the splenic vein. Rt &Lt gastric portal vein ↑ Rt&Lt g. epiploic & short gastric v Splenic v

Lymphatics The gastric lymph nodes consist of two sets. e Superior set accompany the left gastric artery and are divisible into three groups : (a) upper, on the stem of the artery; along the cardiac half of the lesser curvature c) paracardial around the neck of the stomach. They receive their afferents from the stomach; their efferents pass to the celiac LN. 2 -The Inferior set , four to seven in number, along the pyloric half of the greater curvature of the stomach.
 ( mucous)")
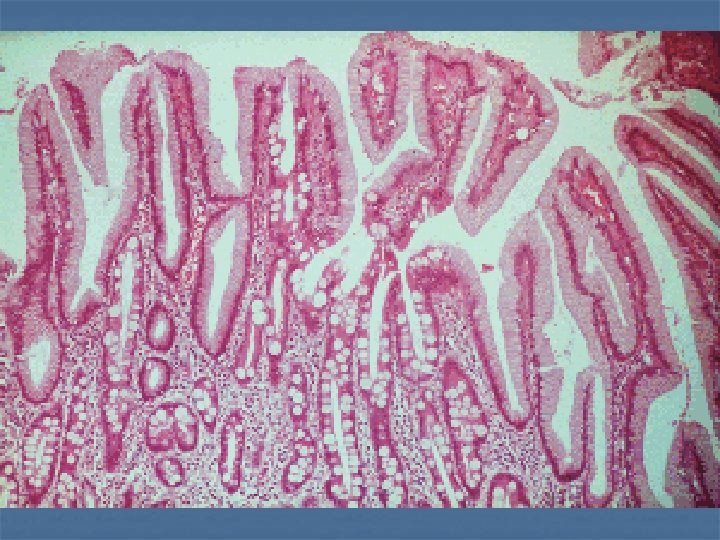
Histological anatomy Stomach Type of cell secretion site 1 -Epith cell (columnar) ( mucous) whole stomach 2 - Parietal cell (acid HCl) secreted by proton pump increase distally (pipsinogen sec. ) proximall 3 -Chief cells 4 -Endocrin cells: -G cells -D cell -ECL (entrochromafin like) in duodenum Bruner glands (gasrten ) ( somatostatin ) (histamin) Antrum whole stomach body (CCK , secreten)

Physiology. Function of the stomach 1 ---a reservoir for ingested food 2 --- mechanical break down of foodstuffs 3 --- digestion by secreasion of acid & pipsin 4 ---protection of mucosa due to these processes 5 passed these products (chyme) on into the duodenum. -Endocrine cells in the duodenum secrete: 1 –cholecystokinin pancreozymin that stimulates the pancreas to produce trypsin and the gall bladder to contract. --Secretin which inhibits gastric acid secretion and promotes production of bicarbonate
 2 types 1 -")
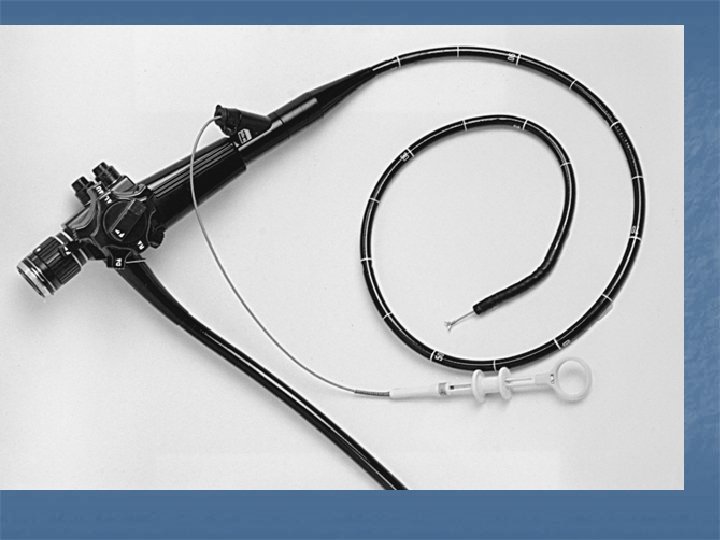
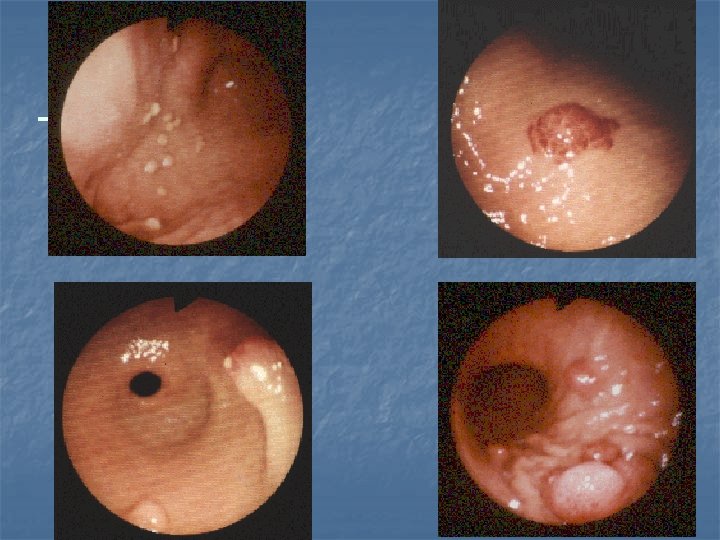
Investigation of the stomach and duodenum 1 - Flexible endoscopy(OGD) 2 types 1 - fibre-optic old style 2 - camera at tip of device The main advantage of this modern instruments is: --not need the fragile fibre optic fibre bundle to transmit the image. --use monitor rather than an eyepiece, .
 endoluminal US laparoscopic US 3 - Contrast radiology(Barium meal) Now less used")
2 -Ultrasonography(US) endoluminal US laparoscopic US 3 - Contrast radiology(Barium meal) Now less used as in previous years because endoscopy is a more sensitive but its better than endoscope in some cases : -
 5 - magnetic resonance imaging (MRI) 6 -Laparoscopy")
4 - Computerised tomography scanning(CT scan) 5 - magnetic resonance imaging (MRI) 6 -Laparoscopy for diagnostic and therapeutic 7 - functional studies -gasrtric acid study -Gastric emptying study

Investigations Ultrasonography detect the classical features in the pyloric canal. Contrast radiology is not now necessary. Differential diagnosis --gastro-oesophageal reflux, --feeding problems, --UTI -- raised intracranial pressure. The condition cannot normally be confused with duodenal atresia or intestinal obstruction because of the absence of bile in the milk vomit.

Acid peptic disease Its group of diseases associated with high acid secretion Gastritis : inflammation of mucosa of stomach ( either acute or chronic) Peptic ulcer : extended through sub mucosa &muscular layer may cause hemorrhage. or perforation
 Causes some GITdiseases such as chronic")
Helicobacter pylori (Barry J. Marshall Noble prize 2005) Causes some GITdiseases such as chronic gastritis, peptic ulceration and gastric tumors. spiral shaped and is fastidious in its requirements, being difficult to culture outside the mucous layer of the stomach. How H pylori causes ulcer ? hydrolyse urea ammonia, a strong alkali. - stimulate the antral G cells is to cause increase gastrin - gastric acid hypersecretion. -- The organism ’ s obligate urease activity is utilised by various tests used to detect the presence of the organism, including the C 13 and C 14 breath tests and the CLO test

Gastritis 1 - type A : due to autoimmune affect. Parietal cell (atrophy of the parietal cell mass) decrease of HCl (achlorhydria. ) + intrinsic factor IF malabsorption of vit B 12 (prencious anemia) --Antrum not affected --hypochlorhydria increase gastrine from G cell hypertrophy of the ECLcells microadenomas ( benign Very rarely become malignant) 2 -Type B : due to H pylori affects the antrum, pangastritis, DU , intestinal metaplasia associated with dysplasia has significant malignant

3 -Reflux gastritis 4 -Erosive gastritis 5 -Stress gastritis. Others Ménétrier ’ s disease. Phlegmonous gastritis

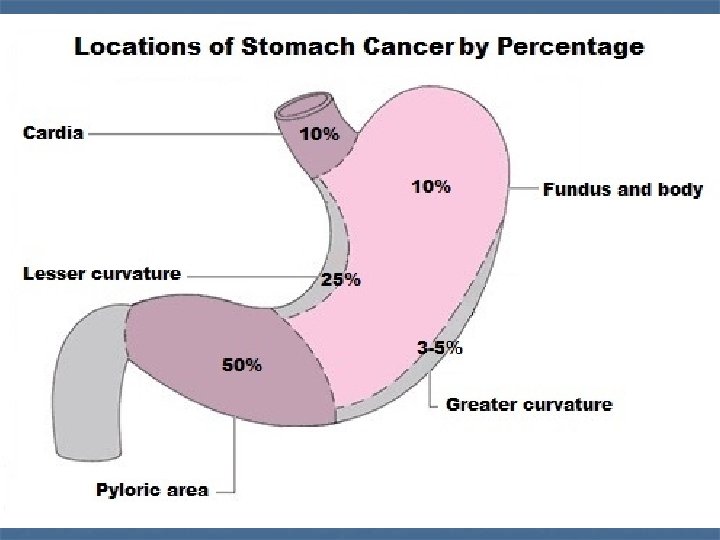
Peptic ulcer Common sites for peptic ulcers are --the first part of the duodenum --the lesser curve of the stomach, --the stoma following gastric surgery, --the oesophagus --Meckel ’ s diverticulum, Malignancy in peptic ulcer -- Chronic duodenal ulcers are not associated with malignancy and, -- gastric ulcers 5% regarded malignant. Multiple biopsies should always be taken

Clinical features of peptic ulcers Pain Periodicity Vomiting, Alteration in weight. Bleeding haematemesis and melaena

Comparison DU&GU DU Common Young high developed No high social countries malig acid GU Less Old low developing <5% social countries low acid
 Medical treatment 1 --modifications to the patient ’ s")
Treatment of peptic ulceration I) Medical treatment 1 --modifications to the patient ’ s lifestyle, particularly the cessation of cigarette smoking. Avoid NSAID, coffee , alcohol 2– Drugs therapy A-Neutralize gastric secretion (HCL): ANTACID B-Inhibits Secretion of Acid: 1)- H 2 - receptor antagonists Cimitidin , ranitidin , famotidin 2)-Proton pump inhibitors(PPI) such as omeprazole, lansoprazol , Pantoprazole the majority within 2 weeks.
 Binds to protein in the")
C- Protection of Gastric Mucosa 1 -Sulfated disaccharide (sucralfate) Binds to protein in the ulcer as protective coat It can inhibits peptic activity 2 -Colloid bismuth Binds protein & against H. pylori D--Eradication therapy is AB against H pylori now we given: Amoxicillin (or clarthromycin ) &metronidazol with PPI ) for 2 weeks then continue other 4 with PPI
 of peptic ulcer surgery Early : - 1 _Heamorrage. , 2 -paralytic")
Sequelae( Complication) of peptic ulcer surgery Early : - 1 _Heamorrage. , 2 -paralytic ileus (truncal vagotomy ) 3 -doudenal fistula due to leaking from suture lines 4 -stomal obstruction due to many causes : Oedema , retrograde intussusption, technical , atonic stomach , 5 -acut pancreatitis
 recurrence* n 2) G J colic fistula diarrhea after eating &vomiting")
Late Complication 1) recurrence* n 2) G J colic fistula diarrhea after eating &vomiting of feacal meterial 3)postgastroctomy syndrome* all stomach small frequent meals -dumping syndrome y dumping hypotention after eating due to apid stomach evacuation dumping hypoglycaemia after eating due to rapid absorption ) c -Bilios vomiting due to afferent loop obstruction
-postvagotomy diarrhea 5) malignant changes alnutrition , Anemia may be due to")
Late complication 4)-postvagotomy diarrhea 5) malignant changes alnutrition , Anemia may be due to er iron or B 12 deficiency Bone disease her may be due to calcium or Vitamin D 7)Intestinal Obstruction due to adhesion allstone disease due to stasis after vagotomy

Recurrent ulceration functional and true recurrence Common site of recurrence following an operation : --in truncal vagotomy same position of the original ulcer (first part of the duodenum) --in gastrojejunostomy, at the anastomosis but on the jejunal side. --in gastrectomy on the jejunal side of the stoma.
 Perforated peptic ulcer - most commonly")
The complications of peptic ulceration ( I ) Perforated peptic ulcer - most commonly occur in elderly female patients. -NSAIDs --the most common site of perforation is the anterior aspect of the duodenum. However, the anterior or incisural gastric ulcer may perforate, --gastric ulcers may perforate into the lesser sac, which can be particularly difficult to diagnoses. n

Clinical features ** Classic presentation is: - n The patient, have a history of peptic ulceration, develops sudden onset severe generalised abdominal pain due to the irritant effect of gastric acid on the peritoneum. shocked. board-like regidity **The less dramatic presentation occur in : - 1 -- elderly patient who is taking NSAIDs 2 -- younger athletic patients 3 --when the leak from the ulcer may not be massive. *S& S of acute appendicitis *Sometimes perforations will seal owing to the inflammatory response and adhesion within the abdominal cavity and so the perforation may be self-limiting.

Investigations 1 - erect plain chest radiograph will reveal free gas under the diaphragm in excess of 50 per cent of cases with perforated peptic ulcer 2 -serum amylase distinguishing between peptic ulcer, perforation and pancreatitis. 3 - Diagnostic peritoneal lavage will usually easily distinguish between perforation and pancreatitis, 4 -ultrasound &- CT scan will normally be diagnostic in both conditions, although this is seldom necessary. * water soluble contrast swallow should not use free leak peritonitis and adhesion

free gas under the diaphragm
 --nasogastric suction -- gastric antisecretory")
Treatment resuscitation --analgesia. (which may mask sign & symotom) --nasogastric suction -- gastric antisecretory agents --IV fluid Laparotomy (laparoscopy may be employed) peritoneal toilet Omental patch to closed perforation
Haematemesis and melaena common causes are: bleeding peptic ulcer 60%, multiple erosions")
( II )Haematemesis and melaena common causes are: bleeding peptic ulcer 60%, multiple erosions 26% , Mallory—Weiss tear 4% bleeding oesophageal varices 4% Ca stomach 0. 5%

principles of management -- resuscitateion -- IV fluid , blood , urine catheter --urgently OGD to determine the cause of the bleeding. -- If bleeding is secondary to a coagulopathy. (i. e warfarin therapy. ) fresh frozen plasma. --if due to gasteric bleeding medical and surgical
 Medical treatments --H 2 antagonist or a proton pump antagonist,")
Bleeding peptic ulcers A) Medical treatments --H 2 antagonist or a proton pump antagonist, --tranexamic acid (cyclocapron ), an inhibitor of fibrinolysis, reduces the rebleeding rate. -- Octreotide, a somatostatin analogue, has not proved effective. endoscopic devices -- injection apparatus (inexpensive )

B-Surgical treatment. • Indication of surgery. n -- continues to bleed --visible vessel in the ulcer base, -- a spurting vessel --an ulcer with a clot in the base are statistically n likely to require surgical treatment to stop the bleeding. --Elderly patients are more likely to die as a result of bleeding than younger patients. Ironically, they should have early surgery. -- A patient who has required more than 6 units of blood in general needs surgical treatment
Gastric outlet obstruction The two common causes -- gastric cancer -- pyloric")
( III )Gastric outlet obstruction The two common causes -- gastric cancer -- pyloric stenosis secondary to peptic ulceration. Clinical features --there is usually a long history of peptic ulcer disease. --the pain may become unremitting and may largely disappear. --The vomitus is totally lacking bile. it is possible to recognise foodstuff. --lossing weight, and appears unwell and dehydrated. --succussion splash may be audible on shaking the patient ’ s abdomen.

Management A-Conservetive --correcting the metabolic abnormality normal saline with potassium supplementation. -- treat anaemic, ( the haemoglobin being spuriously high on presentation. ) -- A large nasogastric tube The stomach should be emptied. and lavage the stomach until it is completely emptied. --antisecretory agent such as ranitidine, given initially intravenously to ensure absorption -- endoscopy and contrast radiology. -- Biopsy of the area around the pylorus is essential to exclude malignancy.
")
Neoplesia of stomach a- Benign : -- gastric polyps: -- metaplastic P ( common) associated with ( H pylori ) --inflammatory P (common) -- fundic gland P associated. with excessive use PPI & familial polyposis disease. ) --Adenomatous P (tubular or villous) premalig. nant -- carcenoid P increase of (ECL cells) associated with P. anemia --Hamartamatous P
 : 1: --Adenocarcinoma ( common 95%) -- colloid Ca (infiltration of")
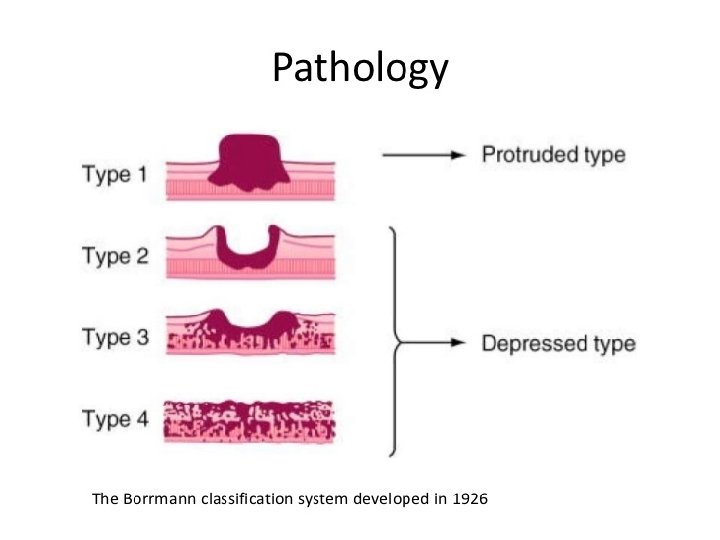
b- Malignant (90%) : 1: --Adenocarcinoma ( common 95%) -- colloid Ca (infiltration of all layers with areolar geltenous substances tissues , Give classical Krukenberg phenomenon ---lentis plastica proliferation of fibrous tissues specialy submucosa deformity of stomach --generlise hour glass & tea pot deformity --localised pyloric obstruction mucosa look normal in OGD while Ba meal look all &distorded mall
--lymphoma (4%) ( primary or part of generalized lymphoma) Primary lymphoma 2")
2 --sarcoma a)--lymphoma (4%) ( primary or part of generalized lymphoma) Primary lymphoma 2 types: --MALT (mucosa Ass. Lymph tissues )ass. With H y eradicated of H pylori --GALT (gut ass. Lymph tissues ) b)--stroma tu. -- leomyosarcoma –vascular tu. -- neurofibrosarcoma --fibrosacoma

Carcinoma of stomach Adenocarcinoma of the stomach has been described as one of the ‘ Captains of the men death, Causes : - 1 - environmental 2 - Premalignent :

Causes 3 -Smocking , dust dysplasia 4 - Carcinogenic Diet : - - H. pylori : ) (Proximal gastric cancer does not associated with H. pylori , in contrast to carcinoma of the body and distal stomach. )
; --twice in black than white --6 -7")
Clinical features : --Male: Female (2: 1); --twice in black than white --6 -7 decade of life: but if it occurs in young(30 -40 y) becomes more aggressive (linitis plastica or signet ring histology) --Low socioeconomic.

Common clinical Manifestation: 1 -Weight loss due to anorexia and early satiety is the (most common) symptoms 2 -Abdominal pain (not severe but common) 3 -Nausea / vomiting 4 -Anemia (common )due to chronic occult blood loss &GIT bleeding (5%) 5 -Dysphagia (cardia involvement)
: For pre-operative staging")
Diagnosis 1 --Endoscopy OGD 2 -CT scan (intravenous and oral contrast): For pre-operative staging --CBP = Hb %PCV, ESR - --Ba study (lintis plastica usually look normal OGD) -- gastric secretary study (achlorhydria) -- Diagnostic laparoscopy

Spread : - -- direct abd. Wall , adjacent structure. - lymphatic tiers of LN N 1=LN near stomach 6 gr. , N 2=LN along branches of caeliac a 5 gr N 3 =LN more distal LN 15 gr] -- blood spread liver , spleen … -- transperitonial (Krukenberg disease ) ovary , colon
 endoscopic mucosal resection stages (T 1 b)")
Treatment options early stages (T 1 a) endoscopic mucosal resection stages (T 1 b) partial gastrectomy&nearby LN Stage II & III subtotal or a total gastrectomy + chemotherapy + or radiation therapy Stage IV palliative Mx ( No surgery )
 Radical surgery is treatment of choice for gastric cancer")
Surgical Treatment : - A) Radical surgery is treatment of choice for gastric cancer Except: 1 -unoperable pateint Can’t tolerate abdominal surgery 2 -unoperable tumor Overwhelming metastasis B) Palliation surgery for non-resective tumors GOAL: - resect all tumors, negative margins (5 cm) and - adequate lymphadenectomy - Enbloc resection of adjacent organ is done if needed.

1 -Endoscopic Resection of Ca. stomach Criteria: stage T 1 a - Tumor < 2 cm in size Lymph Node negative - Tumor confined on the mucosa one Lymph Nodes metastasis : - <3 cm tumor No mucosal ulceration No lymphatic invasions
—subtotal gasterctomy Billoruth I, II stage I, distal tu. (with LN clearance) 3 --total")
2)—subtotal gasterctomy Billoruth I, II stage I, distal tu. (with LN clearance) 3 --total gastrectomy) - stages II, III , upper gastric tumor --Oesophagus will be resected 9 cm proximal to. Tu. section of stomach in bloc with greater &lesser omentum --Close of duodenum. --- oesophago-jejenostomy or stomach reservoir (S or W ype ) --- lymphodenectomy(LN clearance)prepyloric , subpyloric along hepatic art. , splenic hilum 4)--palliative surgery(stage IV) (bypass) gastrojejonostomy

total gasterectomy

other treatment modalities 1 - radiotherapy palliative for painfull bone metasteses 2 - chemotherapy 5 FU, cisplatenium epirepucin In Japan use mitocin C imperegnated charcoal Prognosis : 5 y survival 90% in Japan , 70 % in. UK

Duodenal tumours A-Benign duodenal tumours n Duodenal villous adenomas --occur principally in the periampullary region. -- familial adenomatous polyposis. malignant transformation in such adenomas is the commonest cause of death in patients with polyposis treatment should be locally excised with histologically clear margins.

Endocrine tumours Zollinger—Ellison syndrome gastrin-producing endocrine tumour is often found in the duodenal loop(, although it also occurs in the pancreas, especially the head. ) persistent peptic ulceration. its part of multiple endocrine neoplasia (MEN) type I Dx -- serum gasterin 24 hr PH study a very high basal acid output but no marked response to pentagastrin, Rx proton pump inhibitors such as omeprazole Carcenoid tu.

B-Duodenal adenocarcinoma . periampullary region. Clinical Features -- anaemia due to ulceration of the tumour -- intestinal obstruction as the polypoid neoplasm begins to obstruct the duodenum. --obstructive jaundice due to Direct involvement in the ampulla. -- ascitis due to metastases are commonly to regional lymph nodes and the liver. Rx pancreatrco duodenectomy (Whipples procedure).
- Slides: 58