The Silver Trauma Pathway an update Changing our













- Slides: 14
The Silver Trauma Pathway an update Changing our Approach to Trauma in Older People Shane Roberts Head of Clinical Practice Trauma Management WMAS
Notes from the Elderly Trauma Half Day at QEHB May 2016 1. Assessment of elderly trauma patients by pre hospital providers is difficult due to the different and varied physiological responses to trauma in this group 2. The language of “under triage” or “missed injuries” should not be used and rather it should be accepted that the patient simply didn’t present as a concern to the pre hospital team at the time 3. The triage tool is not at fault but elderly patients with a high impact MOI should be treated with a high index of suspicion and low threshold for MTC 4. A modified triage tool for the elderly is not required 5. Most elderly trauma patients can be adequately treated in a TU 6. Elderly trauma patients can suffer Head Injury without dropping their GCS significantly
7. Any elderly trauma patient that is considered a valid stage 4 trigger should be taken to an MTC, in particular any patient over 65 yrs with an SPB <110 8. MTCs should accept the above 9. TUs must accept that due to the difficulties in assessment they will receive elderly trauma patients possibly without alert who are subsequently found to have significant injuries 10. TUs should adopt a Silver Trauma response so that any elderly trauma patient is rapidly assessed in ED and scanned asap if required 11. TUs should rapidly transfer any elderly trauma patient that requires it to an MTC via the hyperacute transfer pathway 12. The response to the issues caused by elderly trauma should be a whole network response to include an elderly trauma working group to establish procedures and an education programme for pre hospital providers
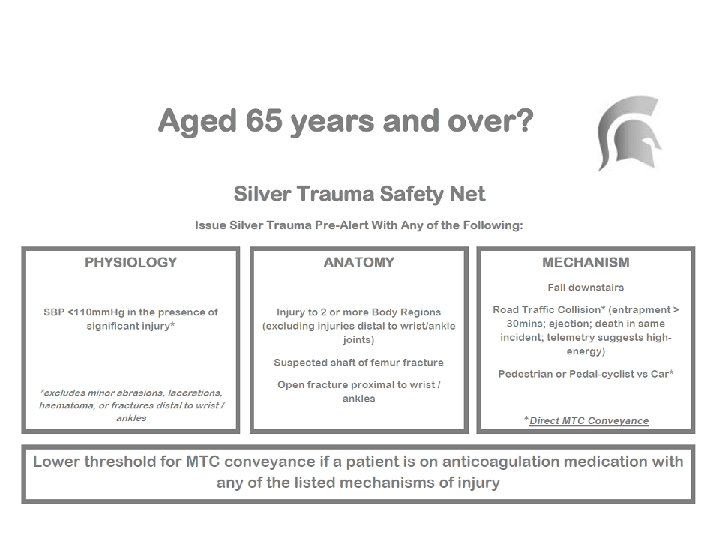
Silver Trauma Safety Net Launched 2017 The Midlands Silver Trauma Group David Raven, ED Consultant HEFT Helen Chamberlain, Trauma Geriatrician UHB Caroline Leech, ED Consultant / PHEM UHCW Richard Hall, ED Consultant UHNM Steve Littleson Trauma Network Data Analyst Sarah Graham, Service Improvement Facilitator MCCTN Shane Roberts, Head of Clinical Practice – Trauma Management WMAS
Executive summary This report shows that our understanding of the demographics of the disease of major trauma is rapidly changing - an older person suffering a fall from standing height is now the commonest type of major trauma in the national database. Assessment of elderly trauma patients by pre hospital providers is difficult due to the different and varied physiological responses to trauma in this group
Key points • The typical major trauma patient in the TARN data has changed from being young and male to being older with a lower degree of male predominance. • Older major trauma patients have a similar injury severity and distribution of injury to younger patients. • Traumatic Brain Injury is the commonest cause of death. • A fall of <2 m is the commonest mechanism of injury in older patients, in contrast to the predominance of road traffic collisions in younger patients. • Current prehospital triage systems are not good at identifying older major trauma patients. • Lack of early identification means that initial treatment is more likely to be in a Trauma Unit, and to be undertaken by a more junior doctor.
• Older patients are much less likely to be transferred to specialist care and have longer times to both investigation and intervention. • Older patients are more likely to die, but those who survive do not have a large incidence of disability compared to younger people. • The death rate increases steeply in older patients from discharge to 1 year – which needs to be taken into account when assessing research outcomes. • There is little seasonal variation in major trauma in older people. • Comorbidity (as measured by the Charlson Comorbidity Index) has an adverse effect on outcome, but it is likely that other factors associated with age have a greater effect. Research is needed to determine the effect of frailty.
Concern raised about an older person who has sustained an injury Pre-Hospital Teams contact the Regional Trauma Desk RTD Applies the Silver Safety Net…… Call to the Emergency Department. . “We’re contacting you with a SILVER TRAUMA ALERT”
ED Reception and Resuscitation – the reality is that ED’s are stretched and therefore there needs to be ways of picking up these patients quickly • ALLOCATE CUBICLE TO RECEIVE PATIENT • ALLOCATE SENIOR CLINICIAN (ST 3 +) • TRAUMA TEAM ACTIVATION IS AT THE DISCRETION OF ED TEAM Aim to prioritise care for people with the potential for major trauma Aim to deliver earlier access to senior clinical input Aim to coordinate earlier access to investigations
Initial Impact
However…. . It didn’t seem to be increasing to the ‘expected’ level, even after a time of bedding in So we looked at the data……… Monthly report from WMAS on the actual number of STA’s passed via them, and the number of TARN submissions that should have had an STA passed, showed that only 1 in 5 were having an STA passed via RTD (and this doesn’t take into account those discharged from ED or within 3 days, so TARN-ve) Due to the submissions times from most TU’s, we had to wait several months to be able to analyse this properly…….
Silver Trauma Safety Net Tool relaunch 2019 Steps we have taken
Conclusions The Silver Trauma Safety Net has had a positive impact on enhancing the care of elderly following trauma The initiative worked well after launch but didn’t continue to perform as expected leading to a relaunch of Comms to both hospital and pre-hospital settings Questions?