The Shoulder Complex Anatomy Joint type Ball and

The Shoulder Complex Anatomy

Joint type �Ball and socket joint ◦ Same as hip, but much shallower ◦ Relies on musculature for stability

Bones �Clavicle �Sternum �Scapula �Humerus

Clavicle ” shaped bone �Spans between sternum to tip of shoulder �Supports anterior shoulder �Lying superficial w/ no muscle or fat protection subjects clavicle to direct blow �“S

Sternum �AKA “breastbone” �Divided into 3 parts: ◦ Manubrium ◦ Body ◦ Xiphoid process �Only source of axial attachment for shoulder complex
 ◦ Acromion (lateral")
Scapula �Flat and triang- ular � 3 projections: ◦ Spine (supraspinous/infraspinous) ◦ Acromion (lateral tip) ◦ Coracoid process (hook-like projection) �Glenoid Fossa ◦ Receives the head of the humerus

3 views of scapula

Humerus �Bicipital groove ◦ Bicep tendon moves up and down in grove during flex/ext of elbow ◦ Proximal end of Humerus

Humerus
 ◦ Acromioclavicular (AC joint) ◦ Glenohumeral")
Articulations � 4 Articulations ◦ Sternoclavicalar (SC joint) ◦ Acromioclavicular (AC joint) ◦ Glenohumeral (GH joint) ◦ Scapulothoracic – not a true joint
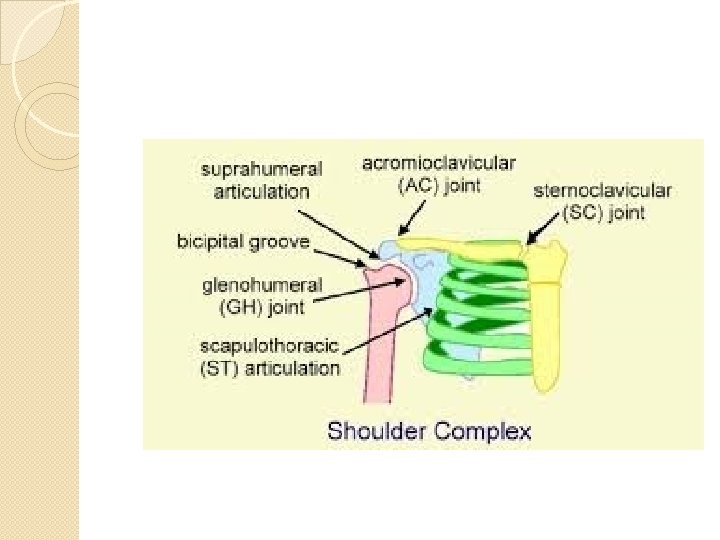

�SC Joint �Medial �AC shock absorber Joint �Thin fibrous capsule surrounds joint. Weak and easily injured
 ◦ Deepened by labrum in Glenoid")
�GH Joint ◦ Enarthrodial (ball and socket joint) ◦ Deepened by labrum in Glenoid Fossa �Scapulothoracic Joint ◦ Not a true joint due to lack of bony articulation ◦ Important for stabilization of shoulder joint ◦ Motions – elevation, depression, protraction, retraction, abductions,

Ligaments – able to identify �Coracoacromial lig �Coracohumeral lig �Superior GH lig �Middle GH lig �Inferior GH lig �Transverse humeral lig


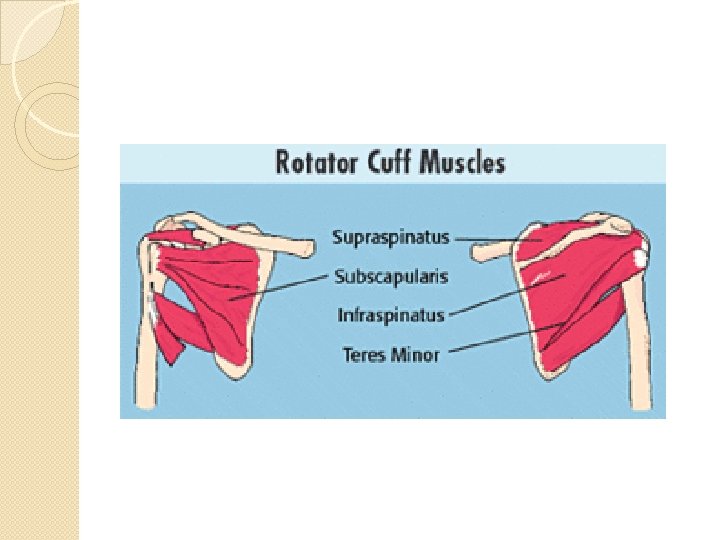
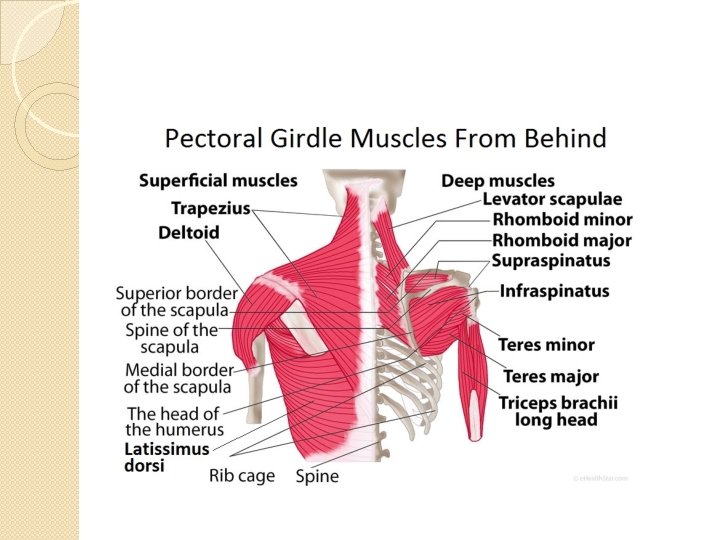
Muscles �Rotator Cuff ◦ Consist of four muscles: �Subscapularis �Infraspinatous �Teres Minor �Supraspinatous �Assoc tendons insert on humerous ◦ Responsible for In. Rot, Ex. Rot, AB-duction �Triceps ◦ 3 heads ◦ Lays over humerus, but acts on Elbow; secondary shoulder extention

Muscles Cont’d �Deltoid ◦ Found over head of humerus ◦ 4 heads ◦ ROM: AB-ducts, Flex, Extend Shoulder �Pecs ◦ Major and Minor �Biceps ◦ Lays over Humerus, but act on Elbow w/ secondary shoulder flexion ◦ 2 heads
 �Abduction (abd) �Adduction (add) �Horizontal adduction (H add) �Horizontal")
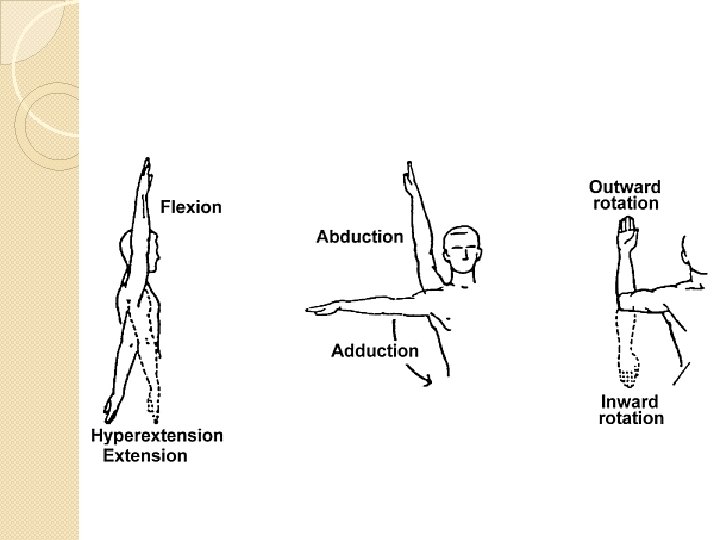
ROM �Flexion �Extension *circumduction (/) �Abduction (abd) �Adduction (add) �Horizontal adduction (H add) �Horizontal abduction (H abd) �Internal rotation (In rot) �External rotations (Ex rot)

Injuries �Shallow structure of the shoulder joint makes it very susceptible to injury �Ways to prevent injury: ◦ Address muscular weakness �Important to strengthen muscles OPPOSING common motion ◦ Use padding �Contact sports with shoulder contact ◦ Modify Activity �Overuse injury �Ath 9 -14 no curve balls; 75 pitch/game;

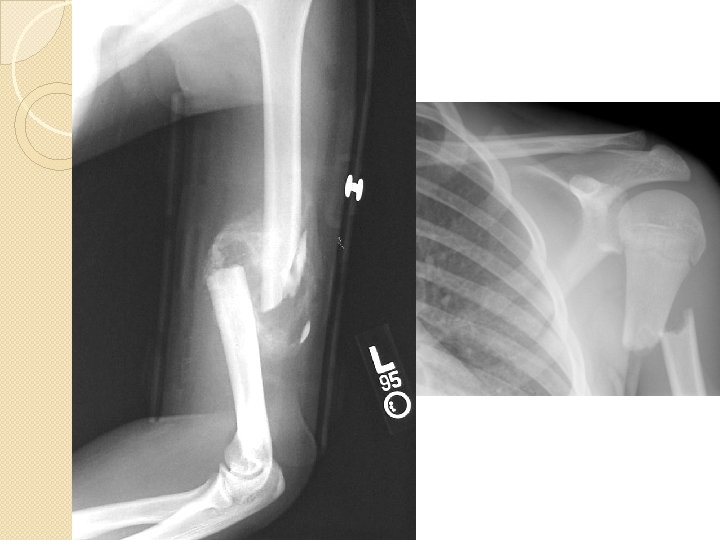
Bone Injuries �s/s: ◦ Pain, Inability to move arm, desire to hold or “coddle” arm, hearing/feeling “pop”, obvious deformity �Clavicular Fx: ◦ Distal 1/3 where “S” changes direction, most common site for fx ◦ MOI: Direct Blow or falling on tip of shoulder ◦ Tx: fig-8 harness; ORIF if necessary; 6 to 8 wks to heal, minimal PT after release



�Humeral Fx: ◦ Musculature can hide fx to humeral head ◦ Sprains can often mimic fx ◦ MOI: Direct blow (most common), falling on elbow (axial load), overuse (least common) ◦ Tx: cast, ORIF (if necessary), modify activity (stress fx)

�Epiphyseal Injuries ◦ Injury to growth plate ◦ MOI: Direct blow, falling on elbow, overuse (most common) ◦ Can cause permanent growth impairment �Avulsion Fx: ◦ Lig/tendon pulls away from bone ◦ Most commonly occurs during shoulder dislocation

�Dislocation/Subluxation ◦ MOI: excessive abduction and external rotation ◦ Shoulder appears flat ◦ May be assoc fx or labral tear, must f/u with Ortho �Multiple disloc occur, surgery may be necessary


Muscle & Tendon Injuries �Rotator Cuff Strain ◦ MOI: most commonly – overuse; excessive motion ◦ Graded 1, 2, 3 �Supraspinatus most commonly injuries ◦ C/O p w/ and w/o movement, p w/ sleeping ◦ Tx: RICE, ROM activites, PRE

�Impingement Syndrome: �MOI: untreated Rotator Cuff injury �Supraspinatus and Biceps tendon run through space beneath acromion process. When space narrows from swelling, tendinitis, poor posture, it impinges the muscle and tendon. �P w/ overhead movement �Tx: modify activity, PRE for posterior muscles, ROM (to improve flexibility of tight pecs)

�Biceps Tendinitis ◦ Inflamed tendon in Bicipital groove ◦ Tx: same as other tendinitis injuries. Immobilizing in sling may provide further comfort �Biceps Tendon Ruptre ◦ MOI: Direct blow, sever contraction forces. ◦ Ath unable to flex elbow, muscles balls up by elbow ◦ Tx: immediate immob, surgery


Ligament and Joint Injuries �AC Joint and GH Joint most commonly injured. �Acromioclavicular Joint Sprain ◦ “Separated shoulder” ◦ MOI: impact to top of shoulder; FOOSH; falling on bent elbow shoving head of Humerus up and into AC joint ◦ C/O P w/ ROM, “Step Deformity”

Step Deformity

�Glenohumeral Joint Strain ◦ MOI: Direct blow when arm is AB-ducted and externally rotated (most often from disloc or sublux) �Can tear labrum as well

� THE END
- Slides: 38