The Role of the Coroner HM Senior Coroner



 Act removed the detection of crime from")




 Radiological examination")










- Slides: 20
The Role of the Coroner HM Senior Coroner Nadia Persaud 17 September 2018
OVERVIEW • • History of the Coroner Modern Coroner Administration of the Coroner’s service Statutory Framework Investigations and Inquests Public Duty Function (PFD reports) How does the Inquest fit with other investigations/court proceedings? • Relationship with Safeguarding teams
HISTORY OF THE CORONER • Evidence of the office dating back to 1194 • Initially King Richard I developed the role which had judicial and financial responsibilities • Responsibilities included examining cases of sudden death and revenue collecting for the Crown • Original Coroners investigated all unnatural deaths, including criminal offences • Original Coroners had received a knighthood and were men of stature and significant financial means
• In 1926 the Coroners (Amendment) Act removed the detection of crime from the remit of the Coroner (Inquest to be suspended) • The 1926 Act also introduced the requirement for a Coroner to have a medical or legal qualification • Coroner is an independent judicial officer • The office is funded by the Local Authority • Now governed by the Coroners and Justice Act 2009 and associated Rules and Regulations • Coroners are supported by a team of Coroner’s Officer (in East London, these are MPS employees)
• A local service – not centrally funded • Coroner’s are independent judges, but the service is not funded by the Mo. J • In East London service is funded by 5 LA Boroughs (one Lead Borough) • In East London, Coroner’s officers (MPS) and administration staff (LA) • 1 full time Coroner, plus Assistant Coroners • 1 Court building • 2017 – 2, 300 deaths reported; 42 investigations opened; 371 Inquests concluded
DUTY TO INVESTIGATE Section 1 of the Coroners and Justice Act 2009 confirms a duty to investigate in the following circumstances: Where the body is lying in the Coroner’s area and there is reason to suspect • The deceased died a violent or unnatural death • Cause of death is unknown • The deceased died in custody or state detention
CUSTODY AND STATE DETENTION • Prison custody • • Police custody Immigration Detention Centre Detained under the Mental Health Act For deaths occurring after 3 April 2017, state detention for the purposes of Section 1, will not include death under Do. LS authorisations • It WILL include those who are deprived of their liberty, but not under a Do. LS authorisation
PRELIMINARY INQUIRIES When the duty to investigate is triggered, preliminary enquiries may take place before a decision is made as to whether to open an Inquest. Preliminary enquiries may include: • Post mortem examination • Medical checks from GP/hospital • Background history from family
FORM OF POST MORTEM EXAMINATION • • Full autopsy Radiological examination (non-invasive) Radiological examination and minimally invasive investigations Toxicology Histology Hair analysis DNA Odontology
INQUESTS • • • Inquest will always be formally opened in Court Once opened, an Inquest must be concluded Witnesses can be summonsed to attend the hearing The Coroner can compel documents to be provided Delays in providing a report can result in a Schedule 5 notice (which can result in a £ 1, 000 fine)
INQUESTS • Inquests should be held within 6 months (any cases over 1 year old have to be reported to the Chief Coroner) • Inquests are inquisitorial, not adversarial • Purpose is set out in Section 5 – who, where, when, how • No “parties” – there are interested persons • Coroner cannot determine criminal liability on part of named person or civil liability
JURY Most cases are heard by a Coroner alone. Certain cases require a jury. These are: • Deceased died in custody/state detention and the cause of death is violent; unnatural or unknown • Death is due to the act or omission of a police officer in the execution of their duties • Death is caused by a notifiable accident, poisoning or disease The Coroner also has a discretion to call a jury
ARTICLE 2 Article 2 – Right to Life • Operational obligation • General obligation Difference between Article 2 and traditional inquests
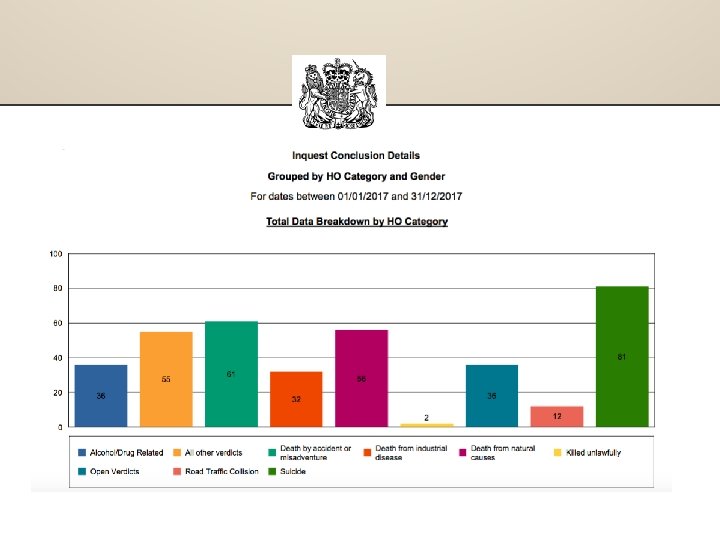
INQUEST CONCLUSIONS The usual inquest outcomes are: • Natural causes • Accidental death • Suicide • Drug related – alcohol related, or a combination of both of these • Lawful or unlawful killing • Road traffic collision • Narrative conclusion • A rider of neglect may be added • Open
CHALLENGING DECISIONS • Judicial review to the High Court • Application to the Attorney General • No appeal to the Chief Coroner Complaints may be made to: • Judicial Conduct Investigation Office • Coroner (if relating to the general service)
PREVENTING FUTURE DEATHS REGULATION 28 REPORTS If during the course of the investigation, evidence gives rise to concern that there is a risk that further deaths will occur, the Coroner has a duty to write a report to the person or organisation which has the power to make changes to improve the systems in place.
HOW DOES THE INQUEST FIT WITH OTHER INVESTIGATIONS? Unnatural/unexplained death in a Care Home Internal investigation CQC notification Local Adult Safeguarding notification and investigation Police investigation HSE or LA investigation • • • Civil claim • Disciplinary/regulatory investigation
RELATIONSHIP WITH SAFEGUARDING AGENCIES • Sharing information (Worcestershire County Council & Worcestershire Safeguarding Children Board v HM Coroner for Worcestershire) Chief Coroner Law Sheet Number 3 and Mo. J Guidance • R (on the application of the Secretary of State for Transport) v HM Senior Coroner for Norfolk 2016) • Building relationship/improved communication and understanding • Presence at meetings/inquests
ANY QUESTIONS?